Homoeopathic treatment of Bronchial Asthma: A case report
ABSTRACT
Bronchial asthma is one of the major public health problems. Previous studies on asthma have shown that homoeopathic treatment help in reducing the frequency and intensity of episodes of asthma and weaning of bronchodilator and other allopathic drugs. One such case report of bronchial asthma is presented below. A female patient aged 45 years attended outpatient department of State National Homoeopathic Medical College and Hospital, Lucknow chiefly for complaint of cough and dyspnoea since 5 years. She has been taking bronchodilator, corticosteroid inhaler and montelukast which help in controlling the paroxysm but her condition remain unchanged. After unsatisfactory outcome with modern medicine, Patient turned to homoeopathic treatment. After detailed case taking and repertorisation a single dose of Phosphorus was given in 200 C, and patient was followed for 3 months and during this period she was free from cough and dyspnoeic episodes and she has stopped taking inhaler and montelukast. The assessment was made by AQLQ(S) Score. The AQLQ(S) Score at baseline was 3 and after completing of treatment was 5. That shows there is marked improvement in symptom and quality of life of patient after homoeopathic treatment.
Key Words: Homoeopathy, Bronchial Asthma, Phosphorus, AQLQ(S), Dyspnoea
Abbreviations: AQLQ(S) – asthma quality of life questionnaire score, IgE – immunoglobulin E, CCRH – Central Council of Research in Homoeopathy, TDS – thrice a day.
INTRODUCTION
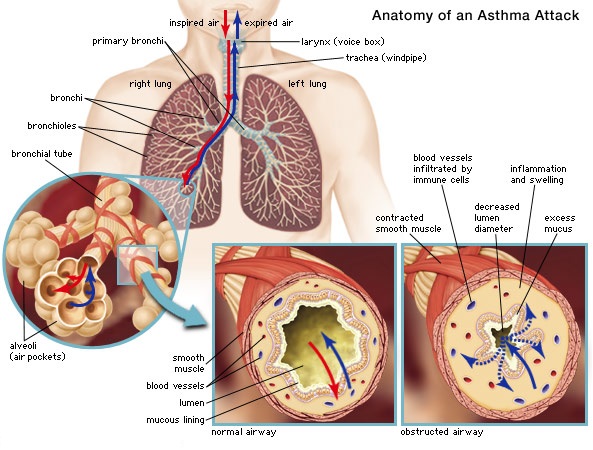
Bronchial asthma clinically presents with symptoms of wheeze, cough, chest tightness and dyspnoea. It has a hereditary predisposition and runs in family. Some of the factors which predispose to asthma are swelling of turbinates, deviation of nasal septum, nasal polyp, adenoids and enlarged tonsils. Majority of patients are sensitive to dust which can excite a paroxysm of attack of asthma.In about 70 percent of patient less than age of 30 years, the asthma is caused by hypersensitivity with increased IgE level, and these antibodies cause allergic reaction when they react with the specific antigen such as plant pollen. In older people, the cause is almost always hypersensitivity to non-allergic types of irritant in the air, such as irritant in smog and exposure to cold, these people present with negative family history of allergy, negative skin test, and normal IgE. These are termed as idiosyncratic.1,2,3
The diagnosis of asthma involves a thorough medical history, physical examination, and objective assessments of lung function to document variable expiratory airflow limitation (spirometry preferred, both before and after bronchodilator). Bronchoprovocation challenge testing and assessing for markers of airway inflammation may also be helpful for diagnosing the disease, particularly when objective measurements of lung function are normal despite the presence of asthma symptoms.4,5
A randomized controlled trial on efficacy of individualised homeopathy in bronchial asthma in adults was conducted by CCRH which found significant treatment benefit of adjunctive individualized homeopathy in bronchial asthma in comparison to adjunctive placebo.6 A review of council clinical research pertaining to Asthma was done which found 20 publications on Asthma. A positive outcome in controlling acute episodes of asthma, reducing the frequency and intensity of subsequent episodes and weaning of bronchodilator and other allopathic drugs have been reported. 7
To assess the clinical results, asthma quality of life questionnaire with standardised activities AQLQ(S) has been used in this case. The AQLQ has 32 questions in four domains (symptoms, activity limitations, emotional function and environmental stimuli).Patient are asked to recall their experience in last 2 weeks and to respond to each question on a 7-point scale (7= no impairment, 1=severe impairment). The overall AQLQ (S) score is the mean of the responses to each of the 32 questions. Therefore, all the 32 responses were added and the total is divided by 32. The resultant overall score will be in between 1 and 7. The best score is 7, which means that the patient has no impairments due to their asthma. However, once the score begins to drop, this means that the patient is experiencing some degree of impairment even if mild. 1.0 is at the other end of the range and indicates severe impairment.
Case report
45 year old, married women presented with cough, breathlessness and wheezing since 5 years.
- She had been suffering from dry cough with suffocative sensation while talking, laughing, from exposure to dust, cold, smell of cooking food and from taking spices. Cough > by expectoration and drinking water. Expectoration was scanty. When attack gets worse, dyspnoea and wheezing starts with cough and she has to take inhaler to get relief. She takes inhaler 2-3 times in a day.
- Headache and soreness in chest while coughing.
- Breathlessness and weakness on exertion like ascending stairs.
HISTORY OF PRESENTING COMPLAINTS
In march 2000, patient suffered from tuberculosis after delivery of her second child for which she took anti tubercular treatment for 1 year from KGMU, Lucknow and got better. In 2015, she started suffering from cough, breathlessness and wheezing for which she took treatment from KGMU, Lucknow. In KGMU, investigations were done, spirometry showed airflow limitation, her chest X-ray was normal, eosinophilic count was 650 cubic mm and was diagnosed of bronchial asthma. She was prescribed corticosteroid inhaler, bronchodilators and montelukast which she has been continuing. In 2017 she had an acute attack of cough and dyspnoea for which she got admitted to Sahara Hospital, Lucknow for 3 days.
PAST HISTORY
Pulmonary tuberculosis in March 2000 took 1 year ATT from KGMU, Lucknow and got relief.
PERSONAL HISTORY
She was a housewife and belonged to middle class socio-economic group.
GYNAECOLOGICAL AND OBSTETRICAL HISTORY
Menopause – 1 year back and menarche was established at the age of 10 years. Also, had a history of profuse menses which last for about 1 week and her menstrual cycles were regular.
Obstetrical history included gravida-6, para-2, abort-4, live-2. Her first child was male aged 19years, she had full term normal vaginal delivery and second child was female aged 15 years, full term normal vaginal delivery. Before delivery of her first child, she had 3 miscarriages and 1 after delivery of her second child.
Generals
Patient was tall, lean, thin, emaciated in appearance as she lost weight. Thermal reaction of patient was chilly and she preferred warm temperature. She liked sweets and cold drinks, but avoided cold as it caused throat complaint. A general feeling of weakness accompanies the patient most of the time. Patient always kept herself busy in household works. She liked to do knitting, cooking, etc. and was very caring for her family. She got irritated and angry easily because of her disease. She had anxiety about health of her family members. There was also anxiety and palpitation when she heard any bad news.
On auscultation, bilateral ronchi were heard.
Analysis of the case
After analysing the symptoms of the case, the characteristics particular and generals were considered for framing the totality. Analysis and evaluation is given in table 1. Cough and dyspnoea on talking loud and laughing, amelioration by drinking water, headache and pain in chest while coughing were the characteristics particular. History of early menarche was also taken in to totality. Patient told that her first menses were established at the age of 10 years that was too early. Early menarche has no relation with asthma but as per homoeopathic point of view it is a peculiar general of patient. A study on age of menarche between generations and factors associated with it found that the mean age of menarche in adolescent girls 12.5±1.42 years and their mother is 14±1.1 years.8 So on average during patient’s generation first menses should be established from 13-15 years. So, 10 years is quiet early and found to be uncommon and peculiar to patient and taken in to totality of symptoms. History of menorrhagia, tendency to miscarriage, weakness, anxiety and palpitation are the marked generals. Considering the above symptomatology, kent’s repertory was preferred and using ZOMEO software, repertorisation was done. The repertorisation chart is given in table 2.9
Table 1. Analysis and evaluation of symptoms
| S.NO | SYMPTOM/GRADATION | Mentals | Physicals | PARTICULAR | COMMON | UNCOMMON |
| 1. | Cough with dyspnoea and wheezing(3) | ü | ü | |||
| 2. | Cough<talking(3) | ü | ü | |||
| 3. | cough<laughing(3) | ü | ü | |||
| 4. | Cough<smell, dust(2) | ü | ü | |||
| 5. | Cough>drinking water(3) | ü | ü | |||
| 6. | Cough>expectoration(2) | ü | ü | |||
| 7. | Dyspnoea on exertion(3) | ü | ü | |||
| 8. | Weakness and suffocation(3) | ü | ü | |||
| 9. | Headache while coughing(3) | ü | ü | |||
| 10. 11. | Anxiety for health about others(3) | ü | ü | |||
| 12. | Menarche-early(3) | ü | ü | |||
| 13. | Tendency to miscarriage(3) | ü | ü | |||
| 14. | Menorrhagia(2) | ü | ü | |||
| 15. | Weight loss | ü | ü |
Table 2. Repertorisation chart
Remedy and follow up
After repertorisation, Phosphorus came out to be the first grade remedy. The rubrics which were chosen are given in table 2. Phosphorus covered 6 symptom out of 7, many other medicines were competing with each other namely Ipecacuanha, Belladonna, Sulphur, Pulsatilla nigricans and Causticum. After consulting materia medica, Phosphorus was chosen. As dry cough on talking and laughing is the key note of Phosphorus. Patient is lean, tall, emaciated, weak with history of tuberculosis, so the constitution also matches with Phosphorus. The Patient has anxiety and palpitation when hears bad news, has anxiety about health which is found in Phosphorus. Patient has desire for cold drinks but avoid it as it causes throat complaint. 10
So, Phosphorus 200C, 1 dose followed by placebo was prescribed on 21-01-2021. According to Boericke, Phosphorus should not be repeated frequently in too low doses in case of TB. As patient has history of TB, so in this case single dose was prescribed.11 Patient is followed for a period of 3 months and during this period patient no longer suffer from cough and dyspnoiec episodes and she has stopped taking inhaler and montelukast. The detail of Follow up is given in table 3. The patient improved symptomatically which was assessed by AQLQ(S) score. The AQLQ(S) score at baseline was 3 and after completing of treatment was 5.
Table 3. Detail of follow up
| Date | Sign and symptoms (mentioning improvement, if any and new symptoms) | Prescription |
| 21-01-21 | According to totality, Phosphorus is prescribed and as per Boericke Phosphorus should not be given in too low and too frequent doses in case of tuberculosis. As she had a history of tuberculosis and very weak, only single dose of 200 potency was selected. | First prescription Phosphorus 200C /1 dose Placebo 30/TDS/ 7days |
| 27-01-21 | Cough-better Dyspnoea-better Takes inhaler occasionally , have stop taking anti-allergic medicines Weakness and anxiety better | Placebo 30/ TDS/10days |
| 8-02-21 | Patient had no cough and dyspnoea. Now she is not taking any allopathic medicine. Anxiety, weakness better. | Placebo 30/TDS/2 weeks |
| 20-02-21 | No complaint, slight weakness on exertion | Placebo 30/TDS/2 weeks |
| 5-03-21 | Patient complained of dyspnoea since 5 days. Weakness is same as before. No other complaint. As Hahnemann mention that every perceptible and striking amelioration precludes repetition. As patient starts complaining of dyspnoea again another dose of phosphorus 200C was given.12 | Phosphorus 200/ 1dose Followed by Placebo 30/TDS/2 weeks |
| 13-03-21 | No complaints. | Placebo 30/TDS/2 weeks |
| 25-03-21 | No complaints. | Placebo 30/TDS/2 weeks |
| 6-04-21 | No complaints. | Placebo 30/TDS/2 weeks |
| 15-04-21 | No complaints. | Placebo 30/TDS/2 weeks |
Discussion and conclusion
In this case, characteristic particulars like cough on talking, laughing and amelioration by drinking, chest pain and headache while coughing were taken in to repertorial totality. Other generals which are marked like abortion, early menarche are also taken in to reportorial totality. These symptoms are converted in to rubrics. After repertorisation medicines which came out were Phosphorus, Ipecacuanha, Belladonna, Sulphur, Pulsatilla nigricans, Causticum in which Phosphorus was the first grade remedy. Other symptoms which were common but present in high intensity in patient were weakness, history of tuberculosis, anxiety, history of menorrhagia. These symptoms were looked in materia medica for final selection. These symptoms were also found in Phosphorus and it was prescribed in 200C. Patient was followed up for 3 months and there is no cough, dyspnoea and wheezing. Also patient stopped taking bronchodilator, corticosteroid inhaler and montelukast.
This case was assessed by AQLQ(S) score. At baseline, the score was 3 and after three months the score came out to be 5. This showed there is improvement in symptoms and quality of life of patient after homoeopathic treatment. This case clearly indicates that homoeopathy proves to be helpful in improving the symptoms of asthma, reducing the episodes of cough, wheezing and dyspnoea, providing permanent relief without relapse, improving the general health of patient and weaning of bronchodilator, corticosteroid inhaler and anti-allergic medicines.
References
- Guyton Arthur. Textbook of Medical Physiology. 10th ed. W.B. Saunders Company International; 2000; 250-260
2. Davidson. Principles and Practice of Medicine. 20th ed. Elsevier Limited; 2006; 670-678
3. Harrison. Principles of Internal Medicine.20th ed. America: Mc Graw Hill Education; 2018. Volume 1:281
4. Jaclyn Quirt et al. Allergy Asthma and Clinical immunology. AACI Journal.2018; Volume 14
5. Standard Treatment Guidelines in Homoeopathy. Central Council For Research in Homoeopathy; 2018; 69- 76
6. Mohammad Qutubuddin et.al. Efficacy of Individualised Homoeopathy in Bronchial Asthma in Adults: Double–blind, Randomized, Placebo-controlled, Clinical Trial in the context of Usual Care. Advances in Integrated Medicine. 2018; Volume 6 (issue 2): 58-65
7. Bindu Sharma, Ritika Hassija Narula, Raj.K. Manchanda. Homoeopathy for the Management of Asthma- a review of council clinical research. IJRH; 2015; Volume 9:69-78
8. Balaji Ramraj et. al. Study on age of menarche between generations and factors associated with it. Clinical epidemiology and global health. 2021; Volume 11(issue 3)
9. Kent J.T. Repertory of the Homoeopathic Materia Medica. 6thAmerican ed. B. Jain publishers Pvt. Ltd; 2005
10. Allen H.C. Keynotes & characteristics Rearranged with Comparison of some of the Leading Remedies of the Materia Medica with Bowel Nosodes. 8thedition. B Jain Publishers Pvt Ltd; 2016
11. Boericke W. Boericke’s New Manual of Homoeopathic Materia Medica with Repertory. 3rd revised & augmented edition based on 9th edition. B Jain Publishers Pvt Ltd; 2016
12. Hahnemann S. Organon of Medicine. Fifth and sixth edition combined. B Jain Publishers Pvt Ltd; 2011;125
About Author:
Meera Sharma1, Komal Prajapat2
PG Scholar, State National Homoeopathic Medical College, Lucknow, U.P.