
Abstract : Hemorrhoid disease ranks fourth in outpatient gastrointestinal diagnosis, Between 45 and 65 years old. In particular, higher socioeconomic status is associated with higher prevalence. Factors that contribute to the increase in the incidence of symptomatic hemorrhoids include conditions that increase internal pressure in the abdomen, such as pregnancy and exercise, or conditions that weaken supporting tissues. Although the prevalence and incidence of hemorrhoids are low, they have a significant impact on the quality of life and have been treated with various surgical and non-surgical therapies.
In this article, we will discuss the anatomy, manifestation, and management of symptomatic hemorrhoid diseases.
Anatomy and Pathophysiology
Hemorrhoids are a group of vascular tissue, smooth muscle and connective tissue distributed in three rows along the anal canal: left lateral, right anterior, and right posterior. Since some of them do not contain muscle walls, these groups can even be treated as sinusoids rather than arteries or veins. In healthy people, hemorrhoids always appear in the form of pillows that surround the anastomoses between the upper arteries and the upper, middle, and lower rectal veins. However, the term hemorrhoids is sometimes used to characterize the biological process of symptomatic hemorrhoids. It is a disease, not a normal anatomy.
The classification of hemorrhoids corresponds to their position relative to the tooth line. External hemorrhoids are located under the teeth and develop from the ectodermal layer. They are covered with an anode composed of squamous epithelium and are innervated by somatic nerves. It provides perianal skin and therefore produces . The outflow of blood vessels from external hemorrhoids flows through the inferior rectal vein, into the genital blood vessels, and then into the internal veins. In contrast, internal hemorrhoids are located above the dental floss and originate from the endoderm. They are covered by columnar epithelium innervated by visceral nerves. The fiber therefore does not cause pain. The vascular outlet of internal hemorrhoids includes the upper and middle veins of the rectum, and then flows into the inner blood vessel.
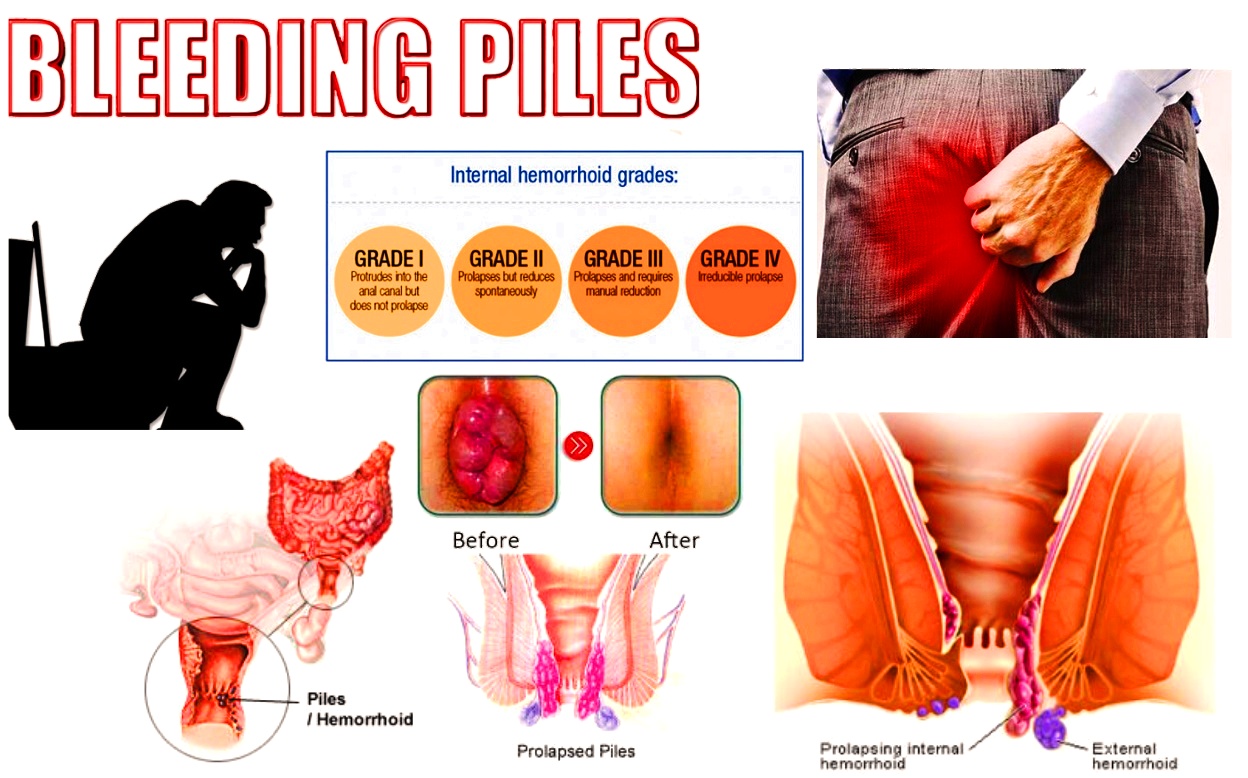
Although the classification of external hemorrhoids is not used clinically, internal hemorrhoids are further stratified according to the severity of prolapse. Secondary hemorrhoids fall out of the tube due to defecation or fatigue, but they contract spontaneously. Third-degree hemorrhoids fall out of the tube and need to be reset manually. Even with the help of the operation, fourth-degree hemorrhoids cannot be eliminated. The exact pathophysiology of symptomatic hemorrhoid disease is unclear. Early theories of hemorrhoids such as anorectal varicose veins are outdated. As suggested by Goenka et al. the incidence of hemorrhoids in patients with malignant hypertension and varicose veins is not high.
The widely accepted concept of sliding anal cushions suggests that hemorrhoids can occur when the supporting tissues of the anal cushion are destroyed. It is believed that age and activities (such as weightlifting, defecation, and sitting for long periods of time) contribute to the ongoing process. Therefore, hemorrhoids is a pathological term that explains the abnormal downward displacement of the anal pillow and causes varicose veins. In histopathological examination, abnormal varicose veins, blood vessel thrombosis, degeneration of collagen fibers and fibrous elastic tissue, and deformities were observed in the anal pillow. In severe cases, the rupture of the anal sub epithelial muscle involves severe inflammatory reactions involving the vessel wall and surrounding tissues, which are related to mucosal ulcers, ischemia and thrombosis.
Symptoms and manifestations
A total of 40% of hemorrhoids patients are asymptomatic. Symptomatic hemorrhoids vary greatly in the range of symptoms. In addition, many other anorectal diseases, such as anal fissures, fistulas, pruritus, conjunctivitis, and even anal cancer, are often referred to as “hemorrhoids” by non-experts.
As the most frequently reported symptom. Bleeding episodes are usually related to bowel movements and are almost always painless. The blood is bright red and covers the stool above the intestines. Blood was found dripping on toilet paper or spilled on the toilet. Another common symptom is the sensation of tissue prolapse, a frequent symptom is that the sensation of tissue prolapse. Prolapsed internal hemorrhoids might accompany delicate unclean incontinence, mucus discharge, sensation of porta fullness, and irritation of perianal skin. Pain is considerably less common with internal hemorrhoids than with external hemorrhoids, however will occur within the setting of prolapsed, strangulated internal hemorrhoids that develop unhealthy changes thanks to the associated ischemia. In contrast, external hemorrhoids are additional likely to be related to pain, thanks to activation of porta innervations related to thrombosis. Patients usually describe a painful porta mass thats tender to palpation. This painful mass could additionally be initially increasing in size and severity over time. haemorrhage also can occur if ulceration develops from mortification of the obstructed hemorrhoid, and this blood tends to be darker and additional clogged than the haemorrhage from internal disease. Painless external skin tags typically result from previous unhealthy or obstructed external hemorrhoids.
HOMOEOPATHIC APPROACH
Aesculus hippocastanum
When this remedy is needed, hemorrhoids are sore and aching, with a swollen feeling. Pain may last for hours after the bowels have moved. People who need this remedy often have the sensation of a lump, or a feeling that a lot of small sharp sticks are inside the rectum, poking them. Sharp and shooting pains may be felt in the rectum and back. A person who needs this remedy may also have low back problems.
Aloe
Hemorrhoids that are swollen and protrude “like a bunch of grapes” and are soothed by cold soaks or compresses may be helped with this remedy. Hemorrhoids may alternate with diarrhea, and the person may have a lot of flatulence.
Graphites
relieves constipation without urges, very large and dry stools, with feeling of heaviness in the lower abdomen, and often associated with anal itching and burning and hemorrhoids.
Nux vomica
relieves hemorrhoids caused by a sedentary lifestyle, and overeating and drinking, especially of spicy and rich foods and alcohol.
Pulsatilla
When this remedy is indicated, hemorrhoids are itchy and uncomfortable, with sticking pains. They are likely to protrude, with improvement after lying down. Warmth often aggravates the symptoms. This is a very helpful remedy for hemorrhoids that appear during pregnancy or around the menstrual period.
Sulphur
Itching, burning, oozing hemorrhoids accompanied by a feeling of fullness and pressure in the abdomen suggest a need for this remedy. The anus is inflamed and red and may protrude significantly. The person may feel worse from warmth and bathing, and have flatulence with a strong, offensive odor.
Arnica montana
Sore, bruised-feeling hemorrhoids may be relieved with this remedy, especially when straining or over-exertion (for instance, childbirth or heavy lifting) has brought on the hemorrhoids.
Calcarea fluorica
This remedy may be indicated for hemorrhoids with bleeding and itching in the anal region, or internal hemorrhoids causing soreness in the very low back and sacrum. The person may also have problems with flatulence and constipation.
Hamamelis virginiana
improves venous circulation and relieves hemorrhoids that are painful with the slightest contact and bleed easily.
Ignatia
Hemorrhoids accompanied by spasms and stabbing pain in the rectum suggest a need for this remedy—especially if the person is sensitive and emotional. Stitching pains can be felt in the rectal area when coughing. Bleeding and pain are often worse when the stool is loose, and rectal prolapse sometimes follows bowel movements.
Dosage Directions
Select the drugs that the majority closely matches the symptoms. In conditions where self-treatment is acceptable , unless otherwise directed by a physician, a lower potency (6X, 6C, 12X, 12C, 30X, or 30C) should be used. additionally , instructions to be used are usually printed on the label.
Many homeopathic physicians suggest that medicines be used as follows: Take one dose and await a response. If improvement is seen, still wait and let the drugs work. If improvement lags significantly or has clearly stopped, another dose could also be taken. The frequency of dosage varies with the condition and therefore the individual. Sometimes a dose could also be required several times an hour; other times a dose could also be indicated several times a day; and in some situations, one dose per day (or less) are often sufficient. If no response is seen within an inexpensive amount of your time , select a special medicine.
Conclusion
Hemorrhoid disease may be a common but complex disease. Patients who present with signs and symptoms of hemorrhoids should be carefully evaluated to exclude other masquerading entities. There are a mess of options for the management of hemorrhoid disease and specific treatment choice should be supported individual patient and clinical factors.
References
1. Everhart J E, Ruhl C E. Burden of digestive diseases in the United States part I: overall and upper gastrointestinal diseases. Gastroenterology. 2009;136(2):376–386. [PubMed] [Google Scholar]
2. Johanson J F, Sonnenberg A. The prevalence of hemorrhoids and chronic constipation. An epidemiologic study. Gastroenterology. 1990;98(2):380–386. [PubMed] [Google Scholar]
3. Shafik A. London: Springer; 2009. Surgical anatomy of hemorrhoids. Surgical Treatment of Hemorrhoids; pp. 7–13. [Google Scholar]
4. Banov L Jr, Knoepp L F Jr, Erdman L H, Alia R T. Management of hemorrhoidal disease. J S C Med Assoc. 1985;81(7):398–401. [PubMed] [Google Scholar]
5. Goenka M K, Kochhar R, Nagi B, Mehta S K. Rectosigmoid varices and other mucosal changes in patients with portal hypertension. Am J Gastroenterol. 1991;86(9):1185–1189. [PubMed] [Google Scholar]
6. Thomson W H. The nature of haemorrhoids. Br J Surg. 1975;62(7):542–552. [PubMed] [Google Scholar]
7. Morgado P J, Suárez J A, Gómez L G, Morgado P J Jr. Histoclinical basis for a new classification of hemorrhoidal disease. Dis Colon Rectum. 1988;31(6):474–480. [PubMed] [Google Scholar]
8. Riss S, Weiser F A, Schwameis K. et al.The prevalence of hemorrhoids in adults. Int J Colorectal Dis. 2012;27(2):215–220. [PubMed] [Google Scholar]
9. Alonso-Coello P, Mills E, Heels-Ansdell D. et al.Fiber for the treatment of hemorrhoids complications: a systematic review and meta-analysis. Am J Gastroenterol. 2006;101(1):181–188. [PubMed] [Google Scholar]
10. Tjandra J J, Tan J J, Lim J F, Murray-Green C, Kennedy M L, Lubowski D Z. Rectogesic (glyceryl trinitrate 0.2%) ointment relieves symptoms of haemorrhoids associated with high resting anal canal pressures. Colorectal Dis. 2007;9(5):457–463. [PubMed] [Google Scholar]
11. Sneider E B, Maykel J A. Diagnosis and management of symptomatic hemorrhoids. Surg Clin North Am. 2010;90(1):17–32. [PubMed] [Google Scholar]
12. Iyer V S, Shrier I, Gordon P H. Long-term outcome of rubber band ligation for symptomatic primary and recurrent internal hemorrhoids. Dis Colon Rectum. 2004;47(8):1364–1370. [PubMed] [Google Scholar]
13. Buchmann P, Seefeld U. Rubber band ligation for piles can be disastrous in HIV-positive patients. Int J Colorectal Dis. 1989;4(1):57–58. [PubMed] [Google Scholar]
14. Nelson R S Ewing B M Ternent C Shashidharan M Blatchford G J Thorson A G Risk of late bleeding following hemorrhoidal banding in patients on antithrombotic prophylaxis Am J Surg 20081966994–999., discussion 999 [PubMed] [Google Scholar]
AUTHORS:
DR. ASHOK YADAV
HEAD OF DEPARTMENT OF PRACTICE OF MEDICINE (HOM.)
DR.M.P.K. HOMOEOPATHIC MEDICAL COLLEGE HOSPITAL AND RESEARCH CENTRE
DR. NAVNEET KAUR , DR.MANSI MISHRA
MD SCHOLAR, DEPARTMENT OF PRACTICE OF MEDICINE (HOM.)
DR.M.P.K.HOMOEOPATHIC MEDICAL COLLEGE HOSPITAL AND RESEARCH CENTRE A CONSTITUENT COLLEGE OF HOMOEOPATHY UNIVERSITY



