Abstract
The following case report is of a male diagnosed with renal calculi in left kidney. Renal calculi is a condition having hard deposits of mineral and acid salts that stick together in concentrated urine. When patient came for consultation, he was presented with pain in abdomen in the right hypochondrium, right lumbar and right iliac region. After thorough case taking, symptoms were aggregated to make the totality and the case was repertorised using Synthesis Repertory in which a few homoeopathic medicines including Aloes socotrina, Natrum muriaticum, Arsenicum album, Sulphur, Sepia, etc. came up. The final selection of remedy was done on the basis of presenting complaints, mental generals, and physical generals.
Keywords
renal calculi, risk factors, Aloes socotrina, homoeopathy
Abbreviations
e.g. – example, Rt. – right, yr – year
Introduction
Nephrolithiasis is a condition in which organic and inorganic masses form within the urinary tract. Stone formation may occur when the urinary concentration of crystals (e.g., calcium, oxalate and uric acid) is high and when the concentration of substances that inhibit stone formation (e.g., citrate) is low.1
Classification and pathophysiology
Kidney stones are broadly categorised into calcareous (calcium containing) stones, which are radio-opaque
and non-calcareous stones. On the basis of their com-position, stones are classified as shown in the table. The figure shows multiple calcium oxalate stones.
Recent evidence indicates that formation of kidney stones is a result of a nanobacterial disease akin to Helicobacter pylori infection and peptic ulcer disease.2 Nanobacteria are small intracellular bacteria that form a calcium phosphate shell (an apatite nucleus) and are present in the central nidus of most (97%) kidney stones and in mineral plaques (Randall’s plaques) in the renal papilla. Further crystallisation and growth of stone are influenced by endogenous and dietary factors. Urine volume, solute concentration, and the ratio of stone inhibitors (citrate, pyrophosphate, and urinary glycoproteins) to promoters are the important factors that influence crystal formation. Crystallisation occurs when the concentration of two ions exceeds their saturation point in the solution.
| Classification of kidney stones3 | ||
| Composition | Causative factors | Frequency (%) |
| Calcium oxalate, Phosphate or both | Underlying metabolic abnormality, idiopathic (25%) | 60-80 |
| Struviate (triple phosphate) | Infection | 10-15 |
| Uric acid* | Hyperuricaemia and Hyperuricosuria Idiopathic (50%) | 5-10 |
| Cystine | Renal tubular defect | 1 |
| Other (xanthine, indigo, triamterene, indinavir*, etc) | 1 | |
| *Pure uric acid and indinavir stones are radiolucent. Cystine stones are radio-opaque because of the sulphur content |
Risk factors for kidney stones
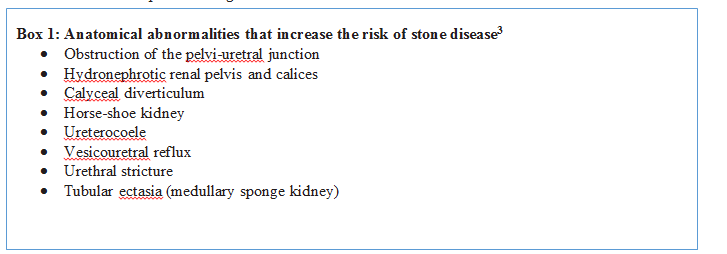
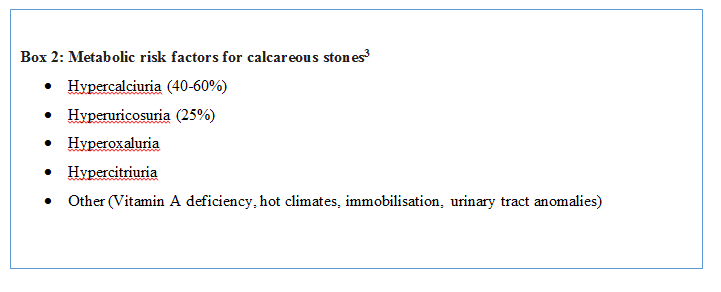
A precise causative factor is not identified in most cases. A family history of kidney stones (increases risk by three times), insulin resistant states, a history of hypertension, primary hyperparathyroidism, a history of gout, chronic metabolic acidosis, and surgical menopause are all associated with increased risk of kidney stones.4-10 In post-menopausal women, the occurrence of kidney stones is associated with a history of hypertension and a low dietary intake of magnesium and calcium.11 Incidence of stones is higher in patients with an anatomical abnormality of the urinary tract that may result in urinary stasis (box 1). Most patients (up to 80%) with calcium stones have one or more of the metabolic risk factors shown in box 2, and about 25% of stones are idiopathic in origin.
Case study
Introduction
A 36 year old male presented with the chief complaints of pain in right side of abdomen since 1 year associated with rumbling in abdomen, after eating, with stool passing during discharge of flatus. He had a history of renal calculi 2 years back which was treated with homoeopathically. He was having addiction of tobacco and alcohol 5years back.
Presenting complaints
- Pain in right sided abdomen (Rt hypochondrium, Rt iliac region, umbilicus) since 1 yr.
Pain with rumbling after eating something
Modalities: Aggravation – after eating,
Amelioration – passing flatus
- Stool during passing flatus
Physical Generals
- Appetite: Adequate
- Thirst: Regular, normal water
- Desire: Salty things
- Aversion: Nothing significant
- Intolerance: Nothing significant
- Stool: Regular, satisfactory
- Urine: Clear, non-offensive
- Sleep: 8 hours/day, refreshing
Mental generals
- Expressed his anger
- Did not want to talk when angry
- Did not want consolation during anger
- Desire for company
Analysis and evaluation of the case:
| Physical generalsIntensity | Desires salty things++ | |||||
| Mental generalsIntensity | Consolation aggravation++ | Doesn’t like to talk when angry+ | ||||
| ParticularsIntensity | Pain in right hypochondrium++ | Pain in umbilicus++ | Rumbling in abdomen after eating++ | Pain aggravates after eating anything++ | Pain ameliorates on passing flatus++ | Passage of stool on passing flatus++ |
Provisional diagnosis
Renal calculus12
Totality of symptoms
- Pain in right hypochondrium
- Pain in umbilicus
- Rumbling in abdomen after eating
- Pain aggravated after eating anything
- Pain ameliorated after passing flatus
- During passing flatus, there is passage of stool
- Desire for salty things
- Consolation aggravation
Reportorial analysis
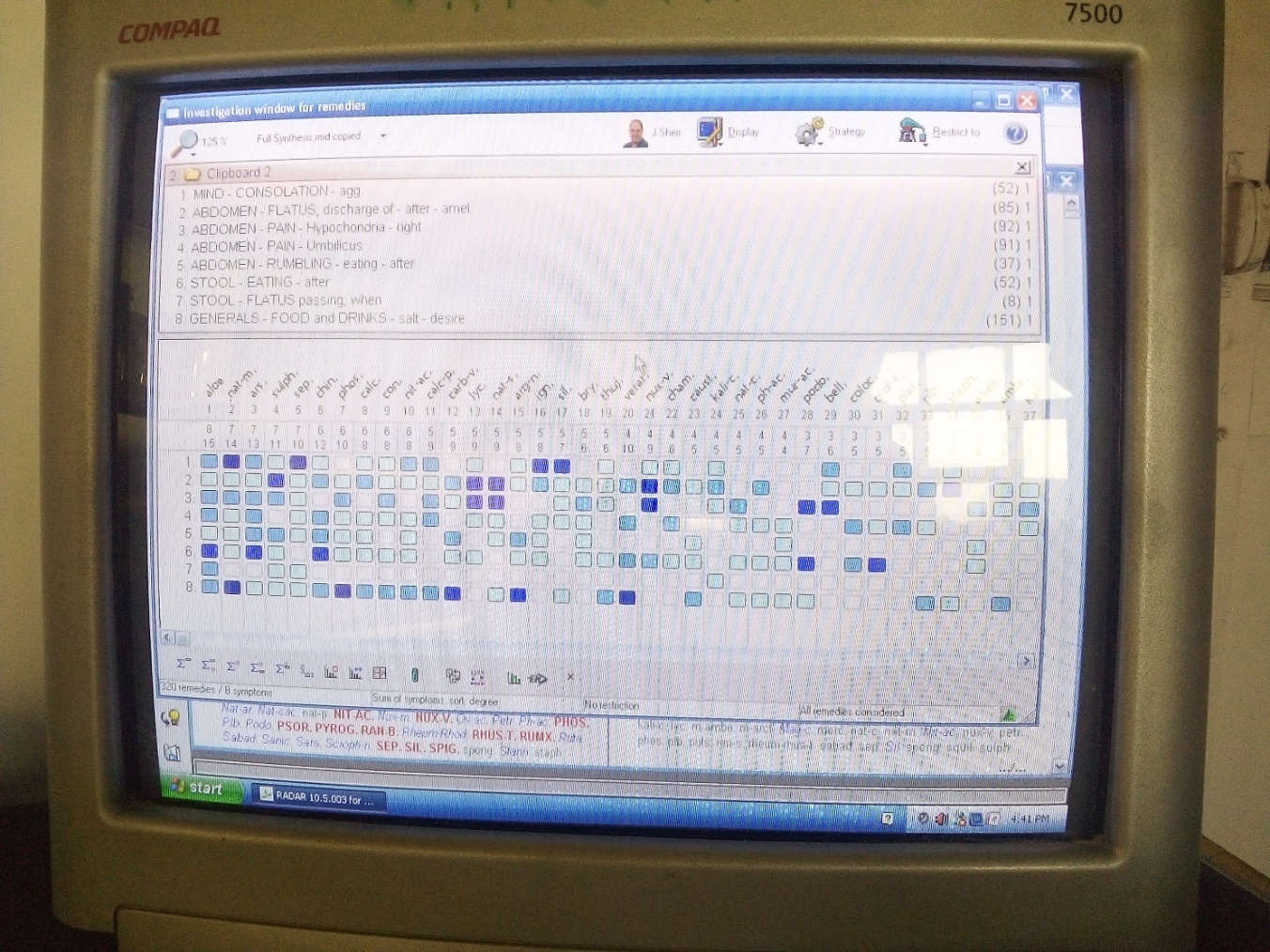
The case was repertorised with the help of Radar Software 10 using Synthesis repertory 2009.13 After the analysis and evaluation of the case, the totality of the case was constructed on the basis of the characteristic symptoms. “Pain in right hypochondrium with rumbling in abdomen amelioration after passing flatus, passage of stool during passing flatus, stool after eating anything, desires salty things were some important symptoms of the case. On the basis of reportorial analysis and consultation of the Boericke materia medica14, Aloes socotrina was found to be the simillimum to the case having the highest score, i.e. 15/8 covering all the rubrics.
Reportorial result13
- Mind- Consolation- Agg
- Abdomen- Flatus – Discharge of – after- amel
- Abdomen- Pain – Hypochondria- right
- Abdomen- Pain – Umbilicus
- Abdomen- Rumbling- Eating, after
- Stool- Eating- after
- Stool- Flatus passing, when
- Generals- Food and Drinks – salt – desire
Prescription
Aloes socotrina 30 / 4 dose
Basis of prescription
After analysing the reportorial result and consultation with The Guiding Symptoms of Our Materia Medica15 and The Dictionary of Practical Materia Medica16, Aloes socotrina 30/ 4 doses were prescribed (including symptoms such as consolation aggravation, pain in right hypochondrium, rumbling after eating and passing stool during flatulence, etc.). Although consolation aggravation and other characteristic symptoms of the case was also present in Natrum muriaticum, Arsenicum album and other remedies in the repertorial result. Aloes socotrina was selected as per the persisting abdominal symptoms. Aloes socotrina was given in 4 doses after which the patient showed improvement in his complaints followed by placebo for 1 month.
Potency– Sixth potency and higher. In rectal conditions, a few doses of the third, then wait.14
Follow Up
| Date | Symptoms | Prescription |
| 15-10-2021 | 1st visit of patient | Aloes socotrina 30 / 4 dose (“The dose of medicine (of the first prescription) that acts without producing new troublesome symptoms in to be continued while gradually ascending, so long as the patient with general improvement, begins to feel in the mild degree the return to of one or several old original complaints”.) (Aph 248,280)17 |
| 25-10-2021 | Slight relief in pain in abdomen | Placebo |
| 05-11-2021 | Pain in abdomen is better than earlier | Placebo |
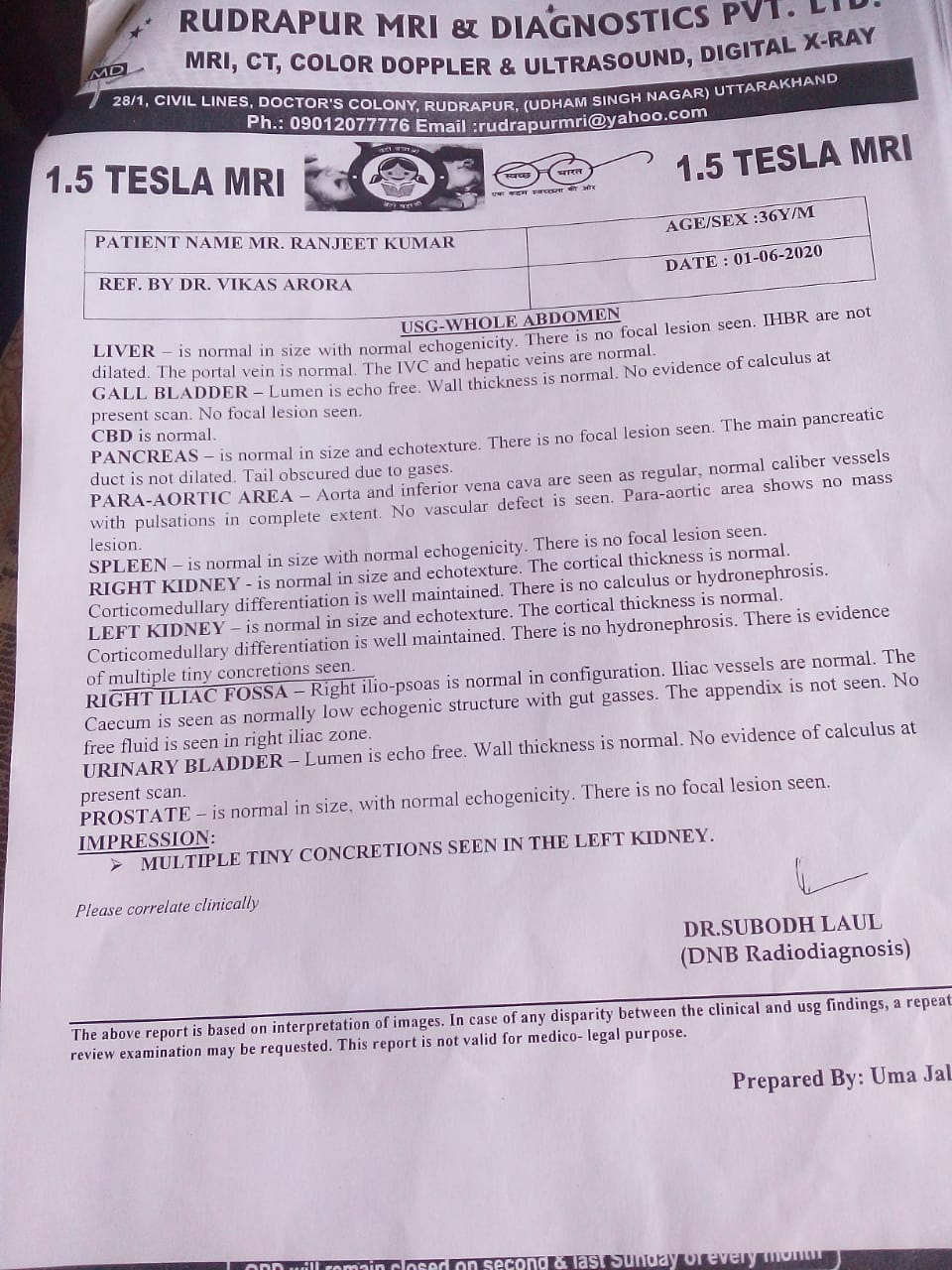
BEFORE
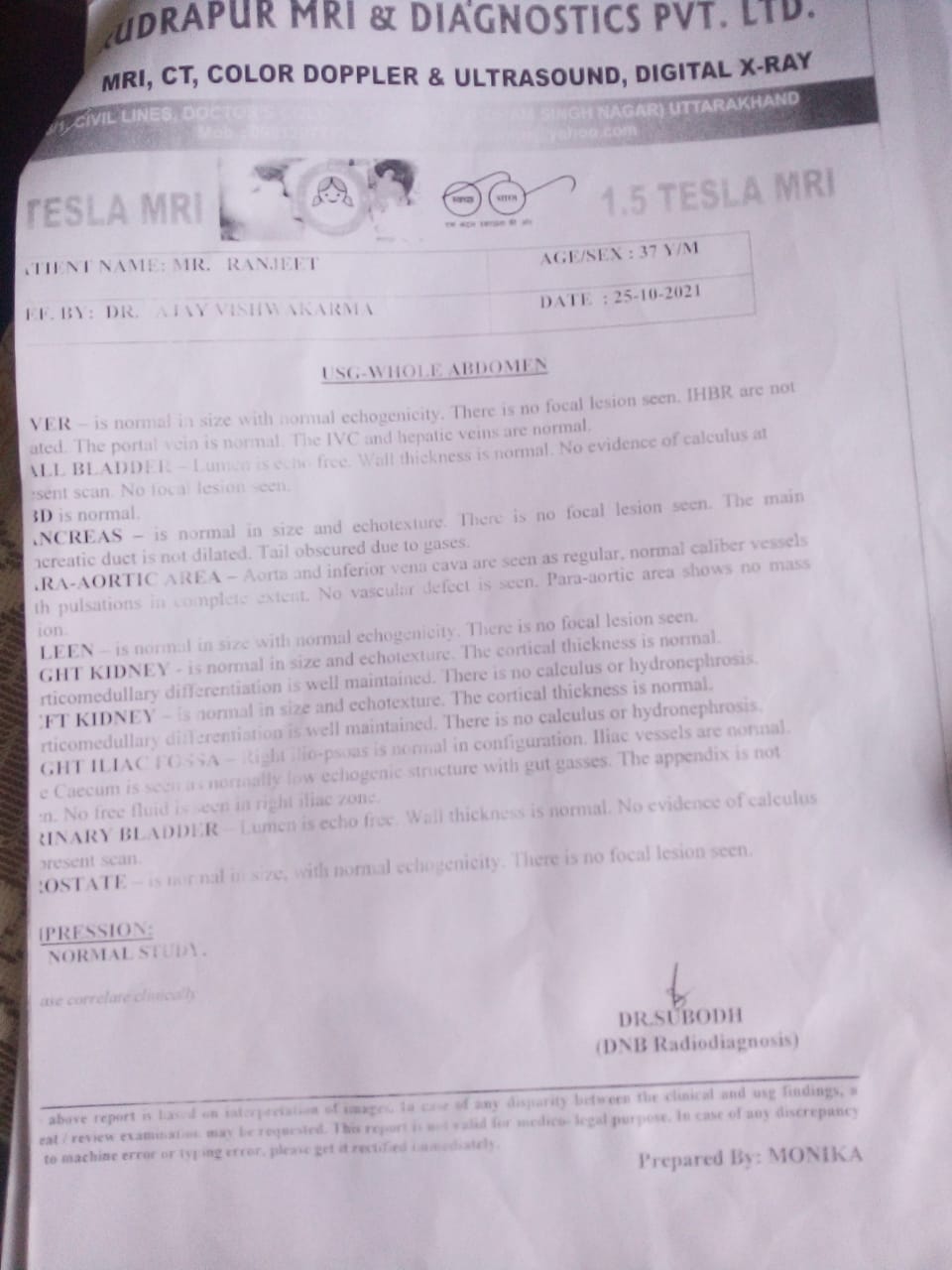
AFTER
Discussion and conclusion
This case of renal calculi is treated according to the cardinal principles of homoeopathy and the medicine selected on the basis of characteristic symptoms, i.e. stool passing with flatus, rumbling sensation in abdomen, etc., mental generals of the patient has proved to be very effective in this case of renal calculi. The potency was selected on the basis of susceptibility of the patient as the patient has a history of addiction of alcohol and tobacco and the pathological condition so the susceptibility of the patient is low this suggested the selection of low potency. The selected medicine, Aloes socotrina, has been given in 4 doses and then the follow up was done in every 10 days with no repetition only placebo was continued for further follow ups. The medicine shown its results in very few doses in a very short period of time this established the fast and gentle recovery according to the homoeopathic principles and philosophy.
The potency selection was done on the basis of susceptibility as stated by18:
Constantine Hering, “if the symptoms of the case generally have more resemblance to the primary symptoms of the drug, then lower potencies, on the contrary more resemblance with the later effects (secondary action) thence advocate higher potencies.”
Dr Close:
1. The greater the
characteristic symptoms of the drug in the case, the greater the susceptibility
to the remedy and the higher the potency required.
2. Age: medium and higher potencies for children
3. Higher potencies for sensitive, intelligent
persons.
4. Higher potencies for persons of intellectual
or sedentary occupation and those exposed to excitement or to the continual
influence of drugs.
5. In terminal conditions even the crude drugs
may be required
He also writes, “different potencies act
differently in different cases and individuals at different times under
different conditions. All may be needed. No one potency, high or low, will meet
the requirement of all cases at all times.”
References
- Alelign T, Petros B. Kidney Stone Disease: An Update on Current Concepts. Adv Urol. [Internet] 2018; [Accessed on 25 Nov 2021] 2018:3068365. Published 2018 Feb 4. doi:10.1155/2018/3068365
- Ciftcioglu N, Bjorklund M, Kuorikoski K, Bergstrom K, Kajander EO. Nanobacteria: an infectious cause for kidney stone formation. Kidney Int [Internet] 1999;56: [Accessed on 25 Nov 2021] 1893-8. [PubMed] [Google Scholar]
- Parmar M. S. Kidney stones. BMJ (Clinical research ed.), [Internet] (2004). [Accessed on 25 Nov 2021] 328(7453), 1420–1424. https://doi.org/10.1136/bmj.328.7453.1420
- Curhan GC, Willett WC, Rimm EB, Stampfer MJ. Family history and risk of kidney stones. J Am Soc Nephrol [Internet]1997;8: [Accessed on 25 Nov 2021] 1568-73. [PubMed] [Google Scholar]
- Sakhaee L, Adams-Huet B, Moe OW, Pak CYC. Pathophysiologic basis for normouricosuric uric acid nephrolithiasis. Kidney Int [Internet] 2002;62: [Accessed on 25 Nov 2021] 971-9. [PubMed] [Google Scholar]
- Cappuccio FP, Siani A, Barba G, Mellone MC, Russo L, Farinaro E, et al. A prospective study of hypertension and the incidence of kidney stones in men. J Hypertens [Internet] 1999;17: [Accessed on 26 Nov 2021] 1017-22. [PubMed] [Google Scholar]
- Mollerup CL, Vestergaard P, Frokjaer VG, Mosekilde L, Christiansen P, Blichert-Toft M. Risk of renal stone events in primary hyperparathyroidism before and after parathyroid surgery: controlled retrospective follow up study. BMJ [ Internet] 2002;325: [Accessed on 26 Nov 2021] 807. [PMC free article] [PubMed] [Google Scholar]
- Kramer HJ, Choi HK, Atkinson K, Stampfer M, Curhan GC. The association between gout and nephrolithiasis in men: the health professionals’ follow-up study. Kidney Int [Internet] 2003;64: [Accessed on 26 Nov 2021] 1022-6. [PubMed] [Google Scholar]
- Baldwin DN, Spencer JL, Jeffries-Stokes CA. Carbohydrate intolerance and kidney stones in children in the Goldfields. J Paediatr Child Health [Internet] 2003;39: [Accessed on 26 Nov 2021] 381-5. [PubMed] [Google Scholar]
- Mattix Kramer HJ, Grodstein F, Stampfer MJ, Curhan GC. Menopause and postmenopausal hormone use and risk of incident kidney stones. J Am Soc Nephrol [Internet] 2003;14: [Accessed on 26 Nov 2021] 1272-7. [PubMed] [Google Scholar]
- Hall WD, Pettinger M, Oberman A, Watts NB, Johnson KC, Paskett ED, et al. Risk factors for kidney stones in older women in Southern United States. Am J Med Sci [Internet] 2001;322: [Accessed on 27 Nov 2021] 12-8. [PubMed] [Google Scholar]
- World Health Organisation (WHO), icd10data.com, 2022 ICD-10 -CM Diagnosis code [Internet], Geneva, Switzerland, World Health Organisation 1993; [Accessed on 29 Nov 2021], https://www.icd10data.com/
- Schroyens F. Radar 10 Homoeopathic Repertory Software. CDROM. [Internet] Available from: http://www.archibel.com/radar10.html. [Accessed on 29 Nov 2021].
- Boericke W. Pocket Manual of Homoeopathic Materia Medica and Repertory. 9th Reprint ed. New Delhi: B Jain Publishers; 2007.
- Hering C. The Guiding symptoms of our Materia Medica, B.Jain Publishers, New Delhi.
- Clarke J H. The Dictionary of Practical Materia Medica, B.Jain Publishers, New Delhi
- Hahnemann S. Organon of Medicine. 6th ed. New Delhi: B Jain Publishers; 2002. p. 227-8
- Close S. M. The Genius of Homoeopathy: Lectures and Essays on homoeopathic philosophy. Homoint.org [Internet]. New York. Nanopathy, 1981. [Accessed on 29 Nov 2021]. http://www.homeoint.org/books4/close/index.htm.
About Author:
Dr Ajay Vishwakarma Principal I/C, (Associate Professor/ HOD,
Department of Anatomy, Chandola Homoeopathic Medical
College and Hospital, Rudrapur, U S Nagar, Uttarakhand)