
Unlocking the Psoric Barrier in Refractory Acne: Observations with 50 Millesimal Potencies – A Prospective Observational Study
Abstract
Psora, the fundamental chronic miasm in homoeopathic theory, is frequently implicated in chronic dermatological conditions such as acne vulgaris. This prospective open-label observational study was conducted on 30 patients with acne vulgaris to evaluate the role of psora and to assess the effectiveness of individualised homoeopathic medicines in 50 millesimal potencies. Acne severity was assessed using the Global Acne Grading System (GAGS) and quality of life using DLQI before and after treatment. The study population showed a female predominance (76.67%). Miasmatic analysis identified Psora as the dominant miasm (63.33%). Therapeutic intervention resulted in marked improvement in 73.33% of cases. Statistical analysis using a paired t-test yielded a significant p-value (<0.001), confirming the efficacy of the protocol. The use of 50 Millesimal potencies provides a gentle, rapid, and sustainable cure by addressing the constitutional dyscrasia without causing homoeopathic aggravation, making it the ideal scale for hypersensitive dermatological cases. The findings suggest that addressing the psoric miasm with individualised 50 millesimal potencies offers an effective and holistic approach in the management of acne vulgaris.
Keywords
Acne vulgaris, psora, 50 millesimal potency, LM potency, miasmatic treatment, Homoeopathy, Dermatology life quality index,
Abbreviations
Global Acne Grading System (GAGS), Dermatology Life Quality Index (DLQI), 50 Millesimal (LM), Acne Severity Index (ASI)
Introduction
Since the early foundations laid by Hahnemann, the study of miasms has remained central to the homoeopathic understanding of chronic diseases. Psora, the ‘Mother of all chronic miasmatic diseases,’ is the underlying and most contagious miasm behind a number of chronic diseases including skin ailments such as acne vulgaris. It represents a constitutional dyscrasia that leads to functional disturbances in the body, predisposing individuals to hypersensitivity, slow healing, and chronic inflammatory conditions.1, 2, 3, 4, 5, 6, 39
Psora is regarded as the primal chronic miasm affecting humankind.2, 3, 5, 7, 39 It is rooted in the deepest depths, almost indestructible and cannot be eradicated during one’s lifetime unless dynamically cured. It affects even the most robust constitutions, for the body alone is not strong enough to eliminate it naturally. Psora is often called the most hydra-headed of all chronic miasmatic diseases, owing to its ability to manifest in numerous forms across different individuals.
The manifestations of Psora are often insidious and not immediately evident. Many individuals carry latent Psora, a dormant state where the miasm remains hidden, without producing significant signs or symptoms. Those who do not acknowledge its hidden existence may regard such people as thoroughly healthy, despite the miasmatic force silently remaining.
Hahnemann writes, “Who does not know the signs of its latent presence, would suppose and declare such persons to be healthy and free from any internal malady, often for years it does not manifest disease.”
Latent Psora remains subdued as long as one has favourable conditions of life i.e., good food, emotional stability, and a healthy environment. But, when the body’s equilibrium is disturbed due to stress, dietary indiscretions, infections, or emotional turmoil, Psora can erupt converting into full-blown disease. In acne vulgaris, this translates to external stimuli like hormonal changes, diet, and stressors that arouse the dormant Psoric miasm, leading to stubborn, chronic outbreaks.
Acne vulgaris is a chronic inflammatory disease of the pilosebaceous unit, affecting up to 80–90% of adolescents and a substantial proportion of adults, with considerable psychosocial impact. Conventional therapies often provide only temporary relief and are limited by side effects, recurrence and antibiotic resistance.15, 16, 18, 20, 21, 32, 33
The employment of 50 millesimal potencies gained importance in homoeopathic practice due to its ability to provide gentle, rapid, and deep-acting results. They are known for their ability to stimulate the vital force in a mild yet effective manner, reducing the risk of aggravation while ensuring sustained healing. It is particularly beneficial in chronic conditions like acne vulgaris, where a gradual yet steady improvement is required without causing undue stress to the patient’s system.
Moreover, 50 millesimal potencies allow frequent repetitions and are particularly suitable to those with heightened sensitivity or those prone to aggravations, a trait commonly observed in individuals with marked psoric predispositions.2, 27, 28, 29, 30, 31.
This research aims to analyse the impact of Psora on acne vulgaris and by conducting a detailed study on acne patients, it will also assess the effectiveness of 50 millesimal potency in alleviating symptoms, reducing recurrence, and improving overall skin health hence, curing the patient. The study will include symptomatological analysis, case documentation, and treatment outcomes in resolution of acne vulgaris.
Through this research, a deeper understanding of the relationship between Psora and acne vulgaris will be established, providing valuable insights into the role of homeopathic miasmatic treatment in dermatological disorders. Furthermore, it will help refine the application of 50 millesimal potency in clinical practice, ensuring a more effective and sustainable approach to treating acne in homeopathy.
Objectives of the study
- To understand the role of psora as a miasmatic and constitutional factor in acne vulgaris.
- To assess the effectiveness of homoeopathic medicines in 50 millesimal potency in the treatment of acne vulgaris using objective clinical scales.
Materials and Methods
Study design and setting
An open-label prospective observational study was conducted on patients diagnosed with acne vulgaris attending the outpatient department / clinic over a period of 6 months. A total of 30 patients fulfilling the inclusion criteria were enrolled and followed up at regular intervals.
Inclusion criteria
- Clinically diagnosed cases of acne vulgaris.
- Patients of both the genders, aged between 15 to 35 years.
- Cases deemed manageable within the scope of homeopathic practice and relevant to the study’s objectives.
- Patients willing to give informed consent and comply with follow-up.
Exclusion criteria
- Patients with comorbidities other than thyroid disorders and PCOS.
- Other serious dermatological conditions likely to confound assessment.
- Pregnant and lactating women.
- Patients presenting with acute medical emergencies.
Assessment tools
- Global Acne Grading System (GAGS) to grade acne severity at baseline and at subsequent visits.14, 23, 24
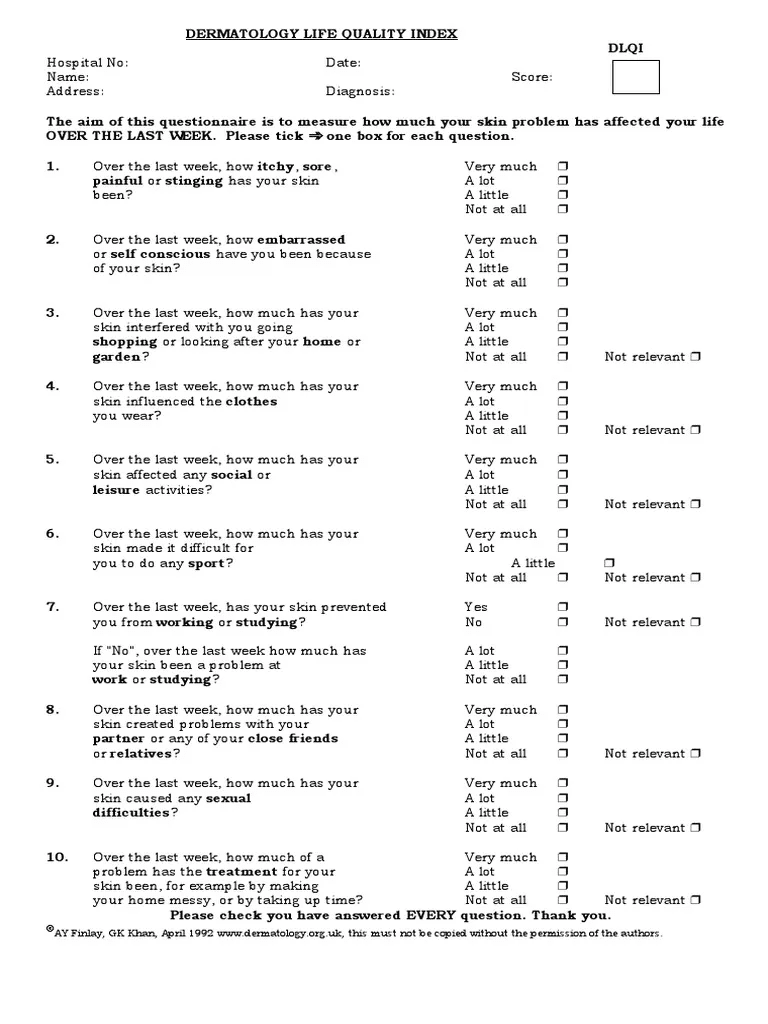
- Dermatology Life Quality Index (DLQI) to assess impact on quality of life.22
- Hormonal Workup: For female patients with signs of hyperandrogenism (e.g., hirsutism, menstrual irregularities), a hormonal panel – Thyroid profile, Testosterone, DHEA-S, LH, FSH and pelvic ultrasound were advised.
- Routine Blood Tests: CBC and ESR were used as baseline inflammatory markers.
Details of Intervention A detailed case taking was performed using a standardized case record form to capture physical, mental, and constitutional symptoms.
Repertorisation: Cases were analysed using standard repertories (Kent, BBCR, Murphy) via software such as HOMPATH and Synthesis 9.0.8, 9, 10, 11, 12, 13
Prescription: The individualized constitutional remedy based on totality of symptoms, miasmatic background and repertorial analysis was administered in 50 Millesimal potency (starting from 0/1, 0/2, ascending based on clinical response).
Administration: Patients were instructed to succuss the remedy bottle before every dose to slightly alter the dynamization, preventing vital force resistance.
No topical homoeopathic or allopathic applications were allowed; basic non-medicated skin-care advice was given uniformly.
Outcome Assessment Criteria: Clinical outcomes were measured using the Dermatology Life Quality Index (DLQI), a validated questionnaire administered before and after treatment.
- Marked Improvement: DLQI score < 10.
- Moderate Improvement: DLQI score 10–20.
- No Improvement: DLQI score 20–30.
Statistical significance was determined using the paired t-test.
Follow-up and outcome criteria
Patients were followed at intervals (e.g. every 15/30 days) for the study duration. At each visit, the following were recorded:
- DLQI score.
- Miasmatic evolution (psoric, mixed or other).
- Any aggravations, new symptoms or adverse events.
Primary outcome: change in mean GAGS score before and after treatment.
Secondary outcomes: change in DLQI, proportion of patients improving by at least one GAGS grade, and qualitative miasmatic changes.
Statistical analysis
Paired observations (pre and post-treatment scores) were analysed using the paired t-test.
With n = 30, ∑d = 45 and ∑d² = 83, the mean difference, standard deviation, standard error and t-value were calculated.
The calculated t-value was compared with the tabulated t value at 0.05 significance level (df = 29; t = 2.045) to test the null hypothesis.
Observations & Results:
Demographic profile: Age distribution of 30 cases
| Age group in years | No. of cases | Percentage |
| 15 -19 | 6 | 20% |
| 20 – 24 | 15 | 50% |
| 25 – 29 | 7 | 23.33% |
| 30 – 34 | 2 | 6.67% |
| TOTAL | 30 | 100% |
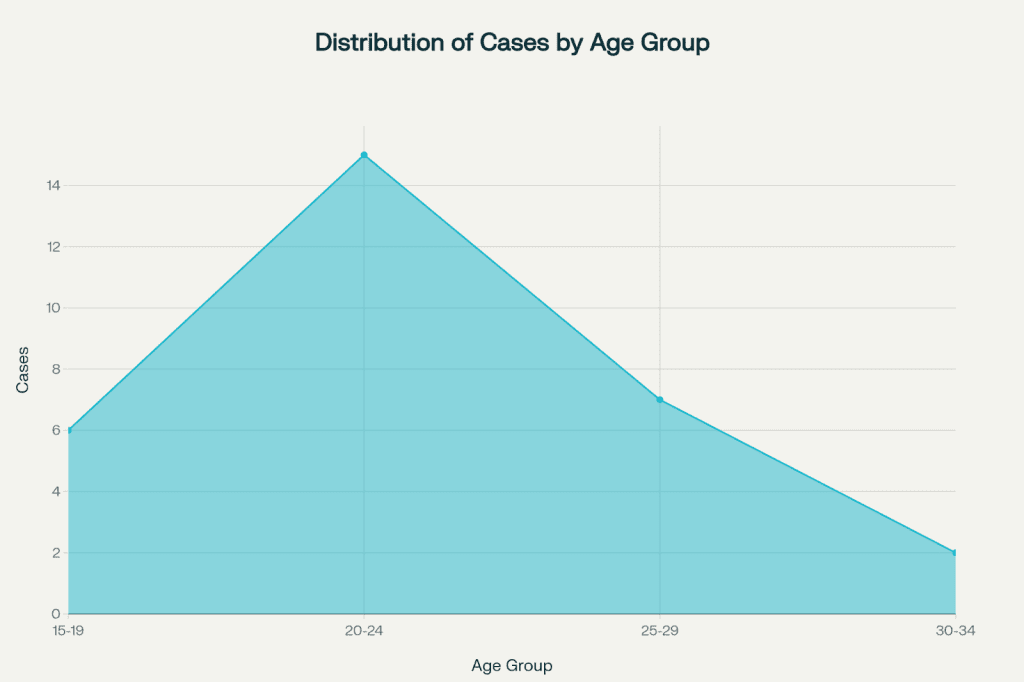
Table no. 1 Showing distribution of age
Demographic profile: Gender distribution of 30 cases
| Gender | No. of cases | Percentage |
| Female | 23 | 76.67% |
| Male | 7 | 23.33% |
| TOTAL | 30 | 100% |
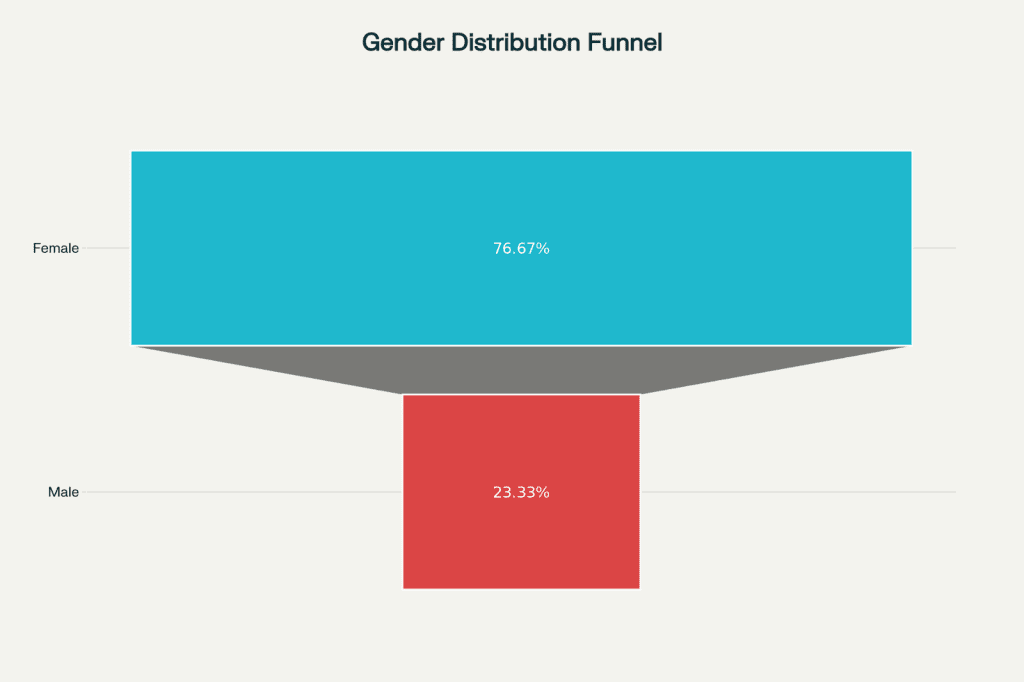
Table no. 2 showing distribution of gender
Triggering factors: Dietary factors, menses, sun exposure, stress, cosmetics, cold weather, sweat, alcohol.
| S. No | Triggering factor | No. of cases | Percentage |
| 1. | Diet | 13 | 43.33% |
| 2. | Menses | 12 | 40% |
| 3. | Sun exposure | 6 | 20% |
| 4. | Stress | 6 | 20% |
| 5. | Cosmetics | 4 | 13.33% |
| 6. | Cold weather/ Winter | 3 | 10% |
| 7. | Sweat | 2 | 6.67% |
| 8. | Alcohol | 1 | 3.33% |
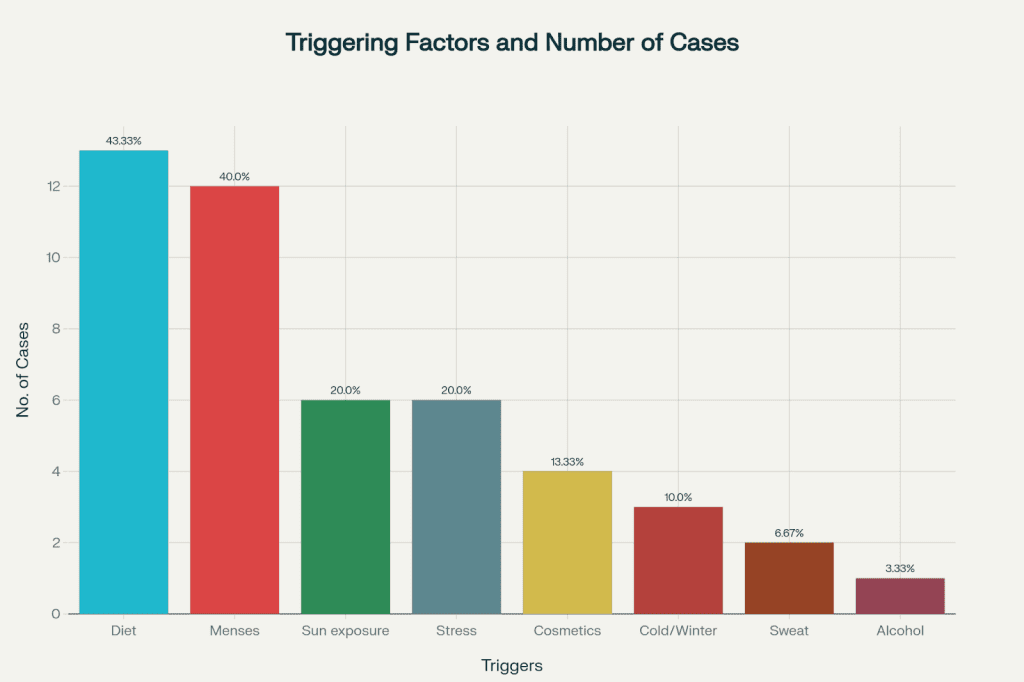
Table no. 3 showing the incidence of triggering facto
Family history: Positive or negative family history of acne
.
| S. No | Family H/o Acne | No. of cases | Percentage |
| 1. | Negative family history | 20 | 66.67% |
| 2. | Positive family history | 10 | 33.33% |
| TOTAL | 30 | 100% |
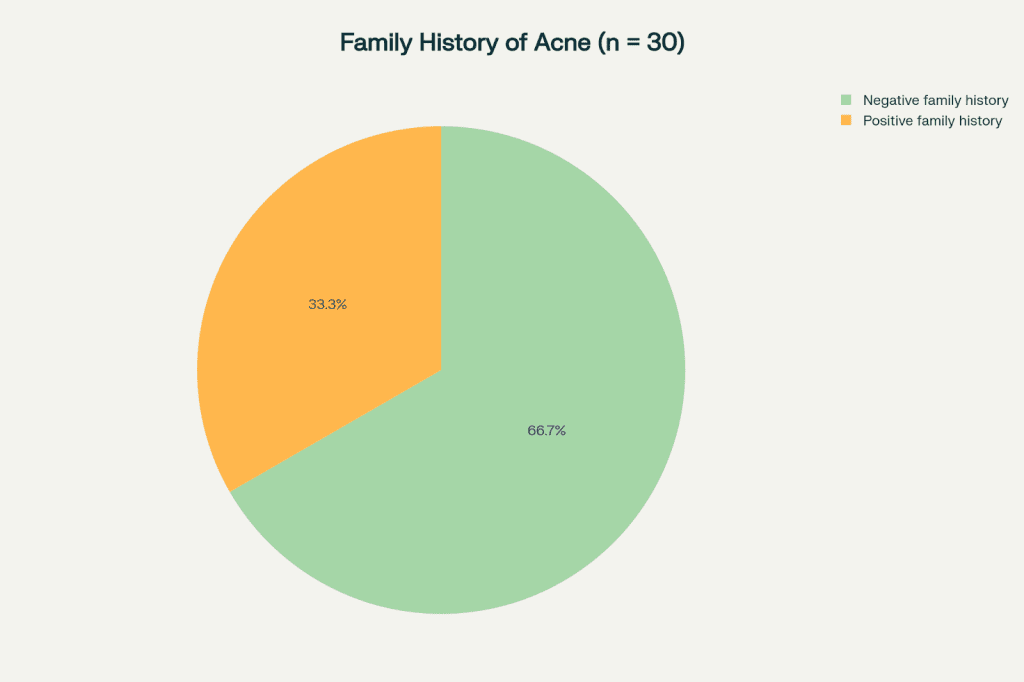
Table no. 4 showing distribution of cases in relation to family history
Comorbidities: Number / percentage of cases with co-morbidities.
| Co – morbid condition | No. of cases | Percentage |
| Absent | 23 | 76.67% |
| Present | 7 | 23.33% |
| TOTAL | 30 | 100% |
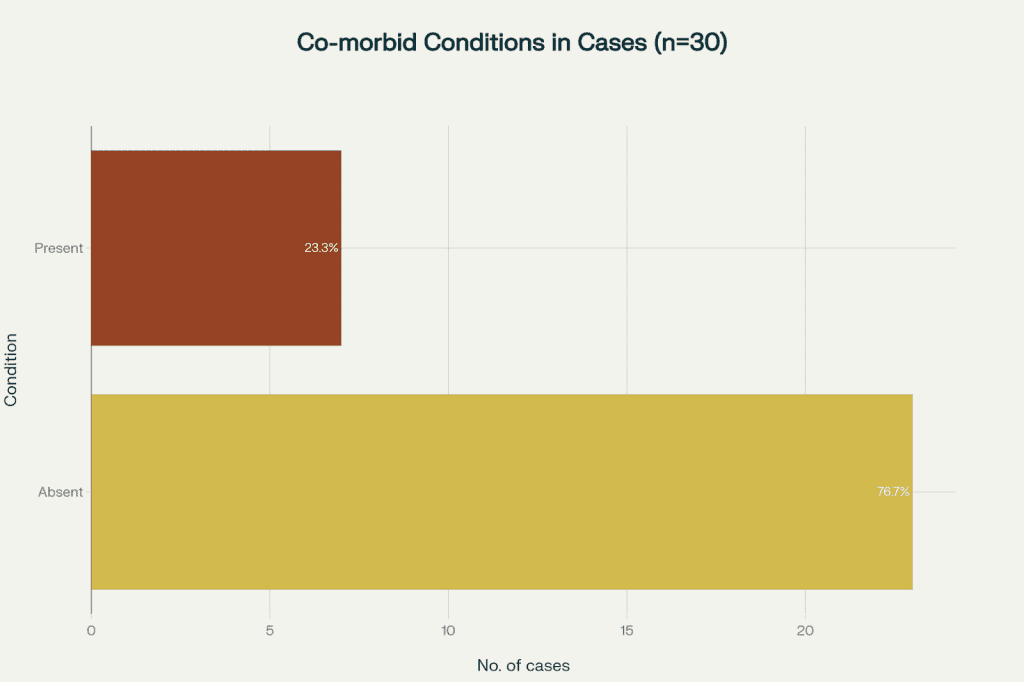
Table no. 5 showing cases relation with co-morbid condition
Comorbidities: Cases relation with co-morbid condition
| Co – morbid condition | No. of cases | Percentage |
| PCOS | 4 | 13.33% |
| Hypothyroidism | 1 | 3.33% |
| PCOS & Hypothyroidism | 2 | 6.67% |
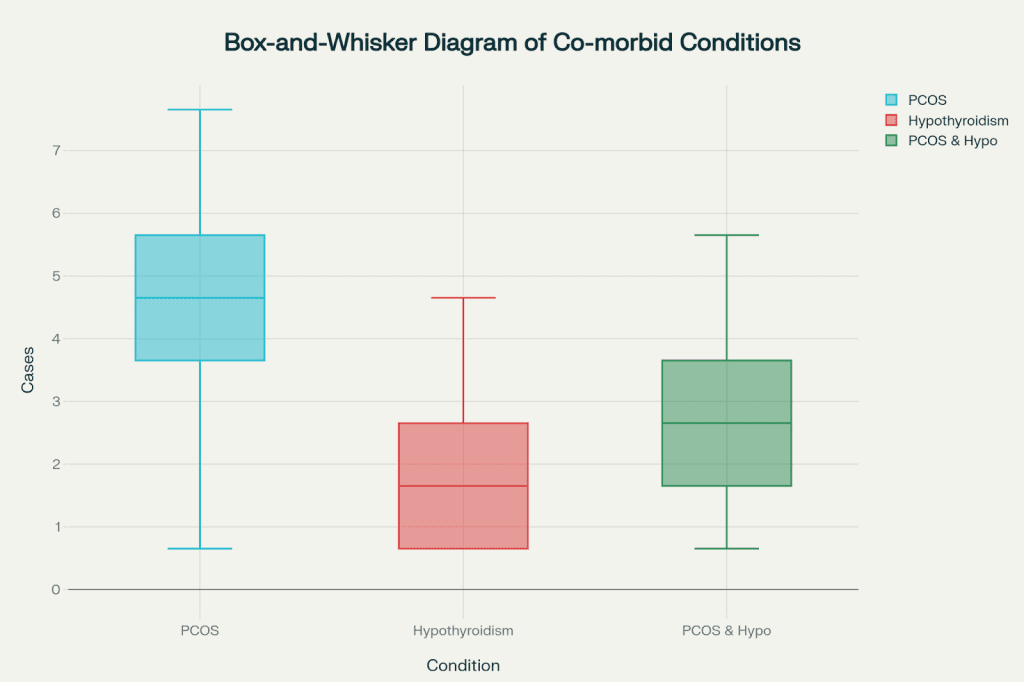
Table no. 6 showing different co-morbid conditions
Disease classification: Number/ percentage of fully and one-sided cases.
| Disease classification | No. of cases | Percentage |
| Fully developed | 20 | 66.67% |
| One sided | 10 | 33.33% |
| TOTAL | 30 | 100% |
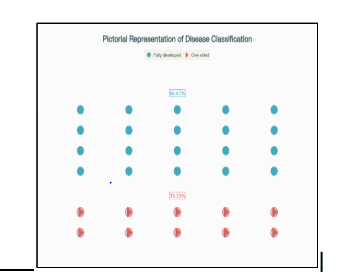
Table no. 7 showing the cases as per Hahnemannian clinical classification of disease
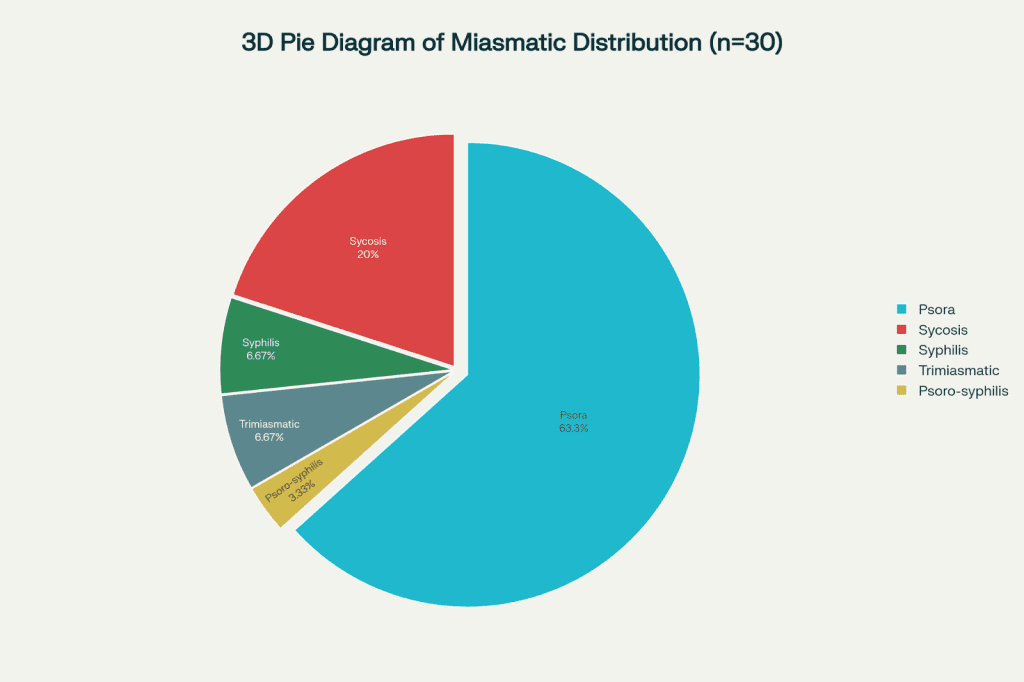
Miasmatic distribution: Numbers/percentages of psoric, sycotic, syphilitic or mixed cases
| S. No | Miasms | No. of cases | Percentage |
| 1. | Psora | 19 | 63.33% |
| 2. | Sycosis | 6 | 20% |
| 3. | Syphilis | 2 | 6.67% |
| 4. | Trimiasmatic | 2 | 6.67% |
| 5. | Psoro – syphilis | 1 | 3.33% |
| TOTAL | 30 | 100% |
Remedy profile: Table of remedies used (e.g. Sulphur, Natrum muriaticum, Pulsatilla, etc.) with frequency and response pattern.
| S. No | Medicine | No. of cases | Percentage |
| 1. | NATRUM MURIATICUM | 6 | 20% |
| 2. | PULSATILLA NIGRICANS | 5 | 16.67% |
| 3. | LYCOPODIUM | 3 | 10% |
| 4. | ANTIMONIUM CRUDUM | 2 | 6.67% |
| 5. | CALCAREA CARBONICA | 2 | 6.67% |
| 6. | SEPIA | 2 | 6.67% |
| 7. | ARGENTUM NITRICUM | 1 | 3.33% |
| 8. | CAUSTICUM | 1 | 3.33% |
| 9. | GRAPHITES | 1 | 3.33% |
| 10. | HEPAR SULPHURIS | 1 | 3.33% |
| 11. | IGNATIA AMARA | 1 | 3.33% |
| 12. | KALI BROMATUM | 1 | 3.33% |
| 13. | LACHESIS | 1 | 3.33% |
| 14. | NUX VOMICA | 1 | 3.33% |
| 15. | SILICEA TERRA | 1 | 3.33% |
| 16. | SULPHUR | 1 | 3.33% |
| TOTAL | 30 | 100% |
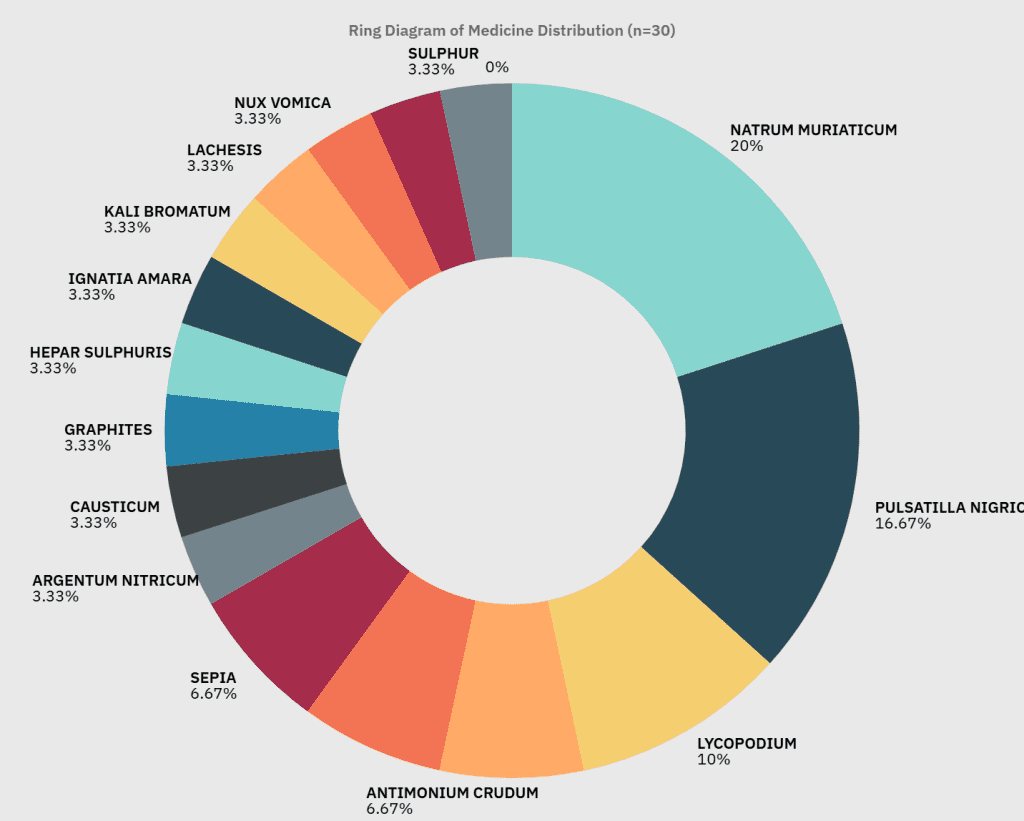
Table no. 9 showing remedies administered during the study
Results of the study:
| Improvement | No. of cases | Percentage |
| Marked improvement (DLQI: < 10) | 22 | 73.33% |
| Moderate improvement (DLQI: 10-20) | 6 | 20% |
| No improvement (DLQI: 20-30) | 2 | 6.67% |
| TOTAL | 30 | 100% |
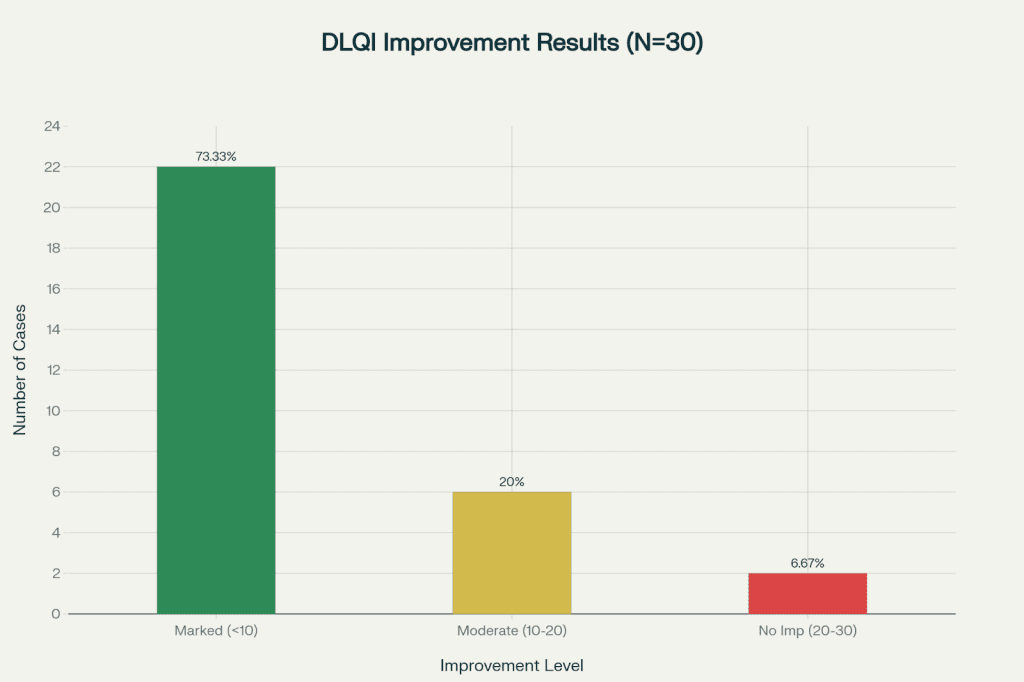
Table no. 10 showing results of the study
Discussion
This study provides a comprehensive overview of acne vulgaris, connecting contemporary biomedical understanding with the principles of classical homeopathy. In particular, the study addresses the miasmatic theory of Psora as an underlying diathesis and examines the clinical application of 50 millesimal potencies in managing this common, yet complex, dermatological condition.
This approach is grounded in Hahnemann’s miasm theory. Psora is considered a fundamental vulnerability underlying a wide spectrum of chronic diseases, including acne. It is also substantiated by Kent and other pioneers of homoeopathy, who recorded the systemic as well as psycho-emotional conditions most commonly associated with cutaneous manifestations.
The occurrence of such concomitant features, from gastrointestinal irregularities to anxiety states, hypersensitivity, and lowered self-esteem, points to an internal imbalance that extends beyond the local skin pathology. This offers a strong rationale for a treatment approach directed at this underlying susceptibility, that extends beyond the simple suppression of symptoms.
Complementing the homeopathic perspective, biomedical research demonstrates that the pathogenesis of acne is multifactorial. Predisposition is caused by anatomical factors like follicular and glandular structure, while endocrine processes, specifically androgens but also with the influence of oestrogens, adrenal, pituitary, and thyroid hormones, regulate sebum production and modulation.
The action of growth factors and inflammatory cytokines further explains the local tissue environment favourable to the formation of acne. This intricate interplay is significantly heightened in situations such as polycystic ovarian syndrome (PCOS), wherein hormonal disturbances directly intensify cutaneous manifestations.
Additionally, lifestyle and environmental determinants such as urban pollutants 34, prescription drugs, and smoking have been established as major determinants that act on an individual’s individual physiological terrain.
The geographic and demographic differences in acne prevalence, including its higher prevalence in humid climates and among certain groups, highlight the significance of contextual, epidemiological variables.
In this context,
Age And Gender Distribution:
As per tables 1 and 2, majority of affected individuals in this study were young females. According to Gollnick, (2014) & Williams et al., (2012), acne among young women tends to persist beyond adolescence, shaped by hormonal fluctuations, societal pressure, and contemporary lifestyle. 16, 17
Triggering Factors:
As per table 3, Diet was identified as a trigger in 43.33% cases, menses in 40% cases. Sun exposure and stress each accounted for 20% cases, while cosmetics were implicated in 13.33% cases and so on.
Banerjea, (2021) describes how dietary indiscretions, cyclical hormonal changes, and psycho-emotional stress act together or independently to provoke or exacerbate acne eruptions, creating a self-perpetuating cycle if not dealt with holistically. 5
Current dermatological manuals such as James et al., (2020) & Oxford Handbook, (2020) corroborate that high glycaemic diets and emotional stressors are potent modulators of sebaceous gland activity and acne severity.18, 19
Family History:
Karciauskiene et al., (2014) highlight the influence of genetic predisposition, affirming that individuals with a family history of acne are at notably higher risk of developing clinically significant cases. 38
Comorbidity Profile:
The intersection between acne and endocrinopathies such as PCOS and hypothyroidism is thoughtfully discussed by Gupta et al. (1998), who suggest that underlying hormonal disturbances can both intensify and prolong cutaneous manifestations The data from table no. 5 & 6 are consistent with these observations, with a proportion of cases presenting combined clinical features.37
Miasmatic Analysis:
Banerjea, (2015) & Mathur, (2021) systematically address the role of miasmatic influence in chronic skin ailments, asserting that a psora dominates many cases of persistent acne and demands recognition in individualized treatment plans. Consistent with this philosophical and clinical insight, psora emerged as the principal miasm as depicted in table 8. 5, 6
Treatment Outcomes:
Hahnemann (6th Ed) says that the dynamic energy of 50 millesimal potencies offers a unique balance between efficacy and tolerability for chronic skin conditions. This proposition is substantiated in modern clinical cases by Kumari & Vinod (2024), who observed significant, lasting improvement in cutaneous disorders using the 50 millesimal scale. 30
The present analysis corroborates these perspectives. The overall success rate of 93.33%, comprising both marked (73.33%) and moderate (20%) improvement, suggests a significant therapeutic effect, with statistical rigor established by paired t-test.
Improvements were observed not only in the acne lesions but also in related problems such as dandruff, hair fall, and leucorrhoea. This reflects the holistic and overall effect of the prescribed remedies, supporting the classical homeopathic view that the right remedy, given in right potency can lead to a general improvement in health.
Limitations Of the Study
Every research study has its limitations, and this one is no exception. The main constraints of this study include a relatively small sample size, being conducted at a single institution, and the lack of blinding. These factors may limit the generalizability of the findings and increase the potential for bias.
Recommendations For Future Research
Given these limitations, it is recommended that future studies be larger, multicentric, and rigorously controlled, in order to provide clearer insights into the outcomes and mechanisms of individualized homeopathic treatment for chronic skin diseases such as acne.
Incorporating modern assessment tools, such as the Dermatology Life Quality Index (DLQI), will enable a more comprehensive evaluation of patient outcomes.
Additionally, including participants from varied socio-economic and genetic backgrounds is advised for broader applicability and relevance of the findings.
Collectively, the findings of this study indicate that individualized homoeopathic treatment, particularly using the 50 millesimal scale, can lead to significant and lasting improvement in patients with chronic acne vulgaris. These results support the importance of constitutional prescribing and individualized patient care in current clinical practice. By integrating the miasmatic model with a thorough understanding of biomedical pathophysiology, this approach provides a distinctive and effective treatment option for a condition that impacts both physical health and psycho-social well-being.
Conclusion
This clinical study titled “Analysing the Impact of Psora on Acne Vulgaris and Assessing the Effectiveness of 50 Millesimal Potency in Its Remedial Protocol” examined the individualized homeopathic management of acne vulgaris, with a particular emphasis on understanding the miasmatic background, predominantly psora, and evaluating the role of 50 millesimal potencies in therapeutic outcomes.
A total of 30 patients diagnosed with acne vulgaris were observed and followed up over a period of 6 to 12 months. The demographic findings indicated that while acne affects both males and females, its prevalence was notably higher among young women, often linked to underlying hormonal disturbances such as polycystic ovarian syndrome (PCOS) and hypothyroidism.
Several contributing factors, including environmental pollution, unhealthy dietary choices rich in oily or greasy foods, excessive cosmetic use, psychological stress, poor hygiene, and urban lifestyle influences, were identified as significant aggravating elements in disease expression. These factors provided deeper insights into the manifestation of psora and its impact on chronic skin conditions.
The study also noted that acne vulgaris extended beyond its dermatological presentation, often accompanied by digestive irregularities, disturbed sleep, and emotional stress, further highlighting the holistic dimension of psoric influence and the importance of treating the individual as a whole rather than merely addressing surface symptoms.
Remedy selection in this study was guided by a thorough evaluation of the patient’s totality of symptoms, encompassing physical, mental, and emotional aspects in accordance with classical homoeopathic principles.
Among the most frequently prescribed remedies were Natrum muriaticum, Pulsatilla nigricans, and Lycopodium clavatum, each reflecting distinct constitutional patterns commonly seen in acne patients.
A remarkable 73.33% of the cases documented significant improvement, 20% showed moderate progress, and only 6.67% exhibited minimal or no response, culminating in an impressive overall success rate of 93.33%. Additionally, improvement in concomitant complaints suggested enhanced systemic well-being, reaffirming the holistic and integrative nature of homeopathic care.
The use of 50 millesimal potencies proved particularly beneficial, allowing individualized dose adjustments, reducing the risk of aggravations, and promoting patient compliance, ultimately leading to more stable and sustained therapeutic results.
The study demonstrates that acne vulgaris, though primarily a dermatological condition, is deeply influenced by internal susceptibility and miasmatic factors, chiefly psora. An individualized, miasmatic-based homoeopathic approach incorporating 50 millesimal potencies offers an effective, gentle, and enduring treatment option for managing chronic acne and its associated systemic symptoms.
Beyond visible skin improvement, the holistic protocol was instrumental in restoring balance at the physical, emotional, and psychological levels, thereby enhancing the overall quality of life of patients.
However, the study acknowledges certain limitations, including a relatively small sample size and a short follow-up duration. To strengthen the evidence base and establish long-term efficacy, future research with large sample size and extended observation period are recommended.
Despite these limitations, this study contributes valuable insights into the interplay between psora and acne vulgaris and highlights the effectiveness of the 50 millesimal scale in achieving sustained recovery through individualized homeopathic treatment.
Bibliography
- Hahnemann S. Organon of Medicine. 6th ed. New Delhi: B. Jain Publishers.
- Hahnemann S. The Chronic Diseases, Their Peculiar Nature and Their Homoeopathic Cure. New Delhi: B. Jain Publishers.
- Allen JH. The Chronic Miasms: Psora and Pseudo-Psora. New Delhi: B. Jain Publishers.
- Kent JT. Lectures on Homoeopathic Philosophy. New Delhi: B. Jain Publishers.
- Banerjea SK. Miasmatic Diagnosis: Practical Tips with Case Examples. New Delhi: B. Jain Publishers.
- Mathur M. The concept of miasm evolution and present-day perspective. Dept. of Practice of Medicine, Nehru Homoeopathic Medical College & Hospital.
- Master FJ. Diseases of the Skin & Their Homeopathic Therapeutics. New Delhi: B. Jain Publishers.
- Boericke W. Pocket Manual of Homeopathic Materia Medica & Repertory. New Delhi: B. Jain Publishers.
- Boger CM. Boger Boenninghausen’s Characteristics and Repertory. New Delhi: B. Jain Publishers.
- Kent JT. Repertory of the Homeopathic Materia Medica. New Delhi: B. Jain Publishers.
- HOMPATH Software. Homoeopathic Repertory Software, version in use.
- Synthesis Repertory, Version 9.0.
- Boenninghausen CM. Boenninghausen’s Characteristics and Repertory (BBCR).
- Doshi A, Zaheer A, Stiller MJ. A comparison of current acne grading systems and proposal of a novel system. Int J Dermatol. 1997;36:416–418.
- Zaenglein AL, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74(5):945-973.e33.
- Williams HC, Dellavalle RP, Garner S. Acne vulgaris. Lancet. 2012;379(9813):361-372.
- Gollnick HPM, Zou Boulis CC. Not all acne is acne vulgaris. Dtsch Arztebl Int. 2014;111(17):301-312.
- James WD, Berger TG, Elston DM. Andrews’ Diseases of the Skin: Clinical Dermatology. 12th ed. Elsevier Saunders.
- Oxford Handbook of Medical Dermatology. 2nd ed. Oxford University Press.
- “Acne Vulgaris – StatPearls.” StatPearls Publishing, NCBI Bookshelf.
- “Physiology, Integument – StatPearls.” StatPearls Publishing, NCBI Bookshelf.
- “Dermatology Life Quality Index (DLQI).” Cardiff University. Available from: https://www.dermatology.org.uk/quality/quality-life-dlqi.html
- “Global Acne Grading System (GAGS).” KBLim Skin Clinic. Available from: https://kblimskinclinic.com/global-acne-grading-system-gags-2/
- “Global Acne Grading System (GAGS).” OneSkin. Available from: https://oneskin.com/?page_id=1573
- Bell IR, et al. Improved clinical status in chronically ill patients after homeopathic treatment: a prospective study in a multisite practice. J Altern Complement Med. 2004;10(6):965-973.
- Adler UC, et al. The influence of the “Paris casebooks” on homeopathic practice. Homeopathy. 2011;100(4):253-260.
- Nayak C, Singh V, Jain S, et al. Homeopathic individualized LM-potencies versus Centesimal potencies for pain management of cervical spondylosis: a multicentre prospective randomized exploratory clinical study. Indian J Res Homoeopathy. 2012;6(4).
- Wulfsberg T. LM Potencies, sometimes a must. Homoeopathic Links. 2019.
- “Fifty Millesimal Potencies – An Overview.” Homeopathy360. Available from: https://www.homeopathy360.com/fifty-millesimal-potencies-an-overview/
- Kumari P, Vinod A. Application of Homeopathic Medicines in 50th Millesimal Potency for Treating Skin Conditions: Insights from Clinical Cases. Int J AYUSH Case Rep. 2024;8(2):261-275.
- “Application of Homeopathic Medicines in 50th Millesimal Potency for Treating Skin Conditions.” IJACARE. Available from: https://www.ijacare.in/index.php/ijacare/article/download/584/410
- “Acne vulgaris and its homoeopathic management: a review.” The Journal of Homoeopathy and Integrated Medicine Sciences (TJHMS).
- “Homoeopathic Perspective on Acne Vulgaris.” IJIRT. Available from: https://ijirt.org/publishedpaper/IJIRT182425_PAPER.pdf
- “The role of diet in acne and rosacea.” J Am Acad Dermatol. Available from: https://pubmed.ncbi.nlm.nih.gov/20363566/
- Karciauskiene J, et al. The prevalence and risk factors of adolescent acne among schoolchildren in Lithuania: a cross-sectional study. J Eur Acad Dermatol Venereol. 2014;28(6):733-740.
- Mallon E, et al. Psychosocial impact of acne vulgaris: evaluating the evidence. Skin Therapy Lett.
- Gupta MA, et al. Psychosocial impact of acne vulgaris. Skin Therapy Lett. 1998.
- Hazarika N, et al. Psychological impact of acne vulgaris among adolescents and adults attending a tertiary care hospital.
- Sehgal VN, et al. Psora: A reappraisal. Indian J Dermatol. 2003;48(4):201-204.


