Abstract – Psoriasis is an autoimmune disease, which can affect any single part such as scalp, nail, trunk, extremities, lips, genitals, etc. or more than one part of body and mind, thereby impacting their quality of life. It predominantly affects the males, chiefly in their third or fourth decades. The diagnosis is mainly clinical and topical therapy is the standard treatment. Many studies have been done and homoeopathy has been found beneficial in treating the disease as well as helps in preventing its recurrence in long run. This article discusses the epidemiology, an etiology, pathophysiology, clinical manifestations, diagnosis, treatment of psoriasis and its homoeopathic management.
Keywords- psoriasis, psychology, homoeopathic management.
Abbreviations – USA – United States of America UVP – ultrasonic vibration potential, UV – ultraviolet, PUVA – psoralen and ultraviolet A radiation
INTRODUCTION-
Psoriasis is a group of common, chronic, inflammatory and proliferative conditions of the skin, associated with systemic manifestations in many organ systems. The most characteristic lesions consist of red, scaly, sharply demarcated, indurated plaques, present particularly over the extensor surfaces and scalp. The extent and severity varies enormously over time and between individuals. Other than physical manifestation of the disease, it has many emotional and psychological effects on the person which affect their social functioning and inter-personal relationships.
Both genetic and environmental influences have a critical role in the aetiology and pathogenesis.[1] Normally in our body, there is a process called cell turnover in which skin cells grows deep in skin and then rise to the surface. This process takes a month but in psoriasis, it happens in just few days because cells rise too fast.
EPIDEMIOLOGY-
Worldwide prevalence of psoriasis is found more in USA and Canada in comparison to Europe, African and Asian countries. According to published reports in 2010, prevalence in different populations varies from 0% to 11.8%.
The studies conducted in India are mostly hospital-based which presents the comparative data from various epidemiological studies on psoriasis. In accordance to data collected from various medical colleges, the incidence of psoriasis among total skin patients ranged between 0.44 and 2.2%, with over all incidence of 1.02%. The ratio of male to female is 2.46:1 with highest incidence noted in the age group of 20-39 years in which the mean age of onset in males and females was comparable.[2][3]
QUALITY OF LIFE AND PSYCHOLOGICAL ASPECTS:
Psoriasis does not affect survival but it has negative effect on patient quality of life like many other chronic diseases. In recent studies, it is stated that nearly one third of the patients of psoriasis have pathological worry and anxiety. There is a feeling of disgrace by their skin condition leading to avoidance behaviour and the belief that they are being evaluated on the basis of their skin disease. Therefore, depression and suicidal tendencies are being found in more than 5% of the patients.
The severity of psoriasis depends upon the physical and psychological factors. In 60% of patients, stress is a key exacerbator of the disease and it is found that psychological stress has the potential to regulate the immune response in which there is an abnormal hypothalamic–adrenal axis response to acute stress, and there are lot of evidences that shows abnormal neuro-endocrine responses to stress which may contribute to the pathogenesis of chronic autoimmune diseases.[4]
AETIOLOGY:
Psoriasis is genetically complex and a large number of genes are thought to be important in its pathogenesis. Empirical studies suggest that if one parent has psoriasis, then the chance of child being affected is 15-20%, and if both parents are affected, then this chance increases to 50%.
FACTORS CAUSING FLARE-UPS OF PSORIASIS:
Trauma- Lesions appear in areas of skin damage such as scratches or surgical wounds (Koebner phenomenon) when the condition is erupting.
Infection- β- haemolytic streptococcal throat infection, often precede guttate psoriasis.
Sunlight- UVR rarely
Drugs- Antimalarial, β-adrenoceptor antagonists (β blocker), and lithium.
Rebound after systemic corticosteroids or potent local corticosteroids are stopped.
Emotion- stress, anxiety, suppression.[5]
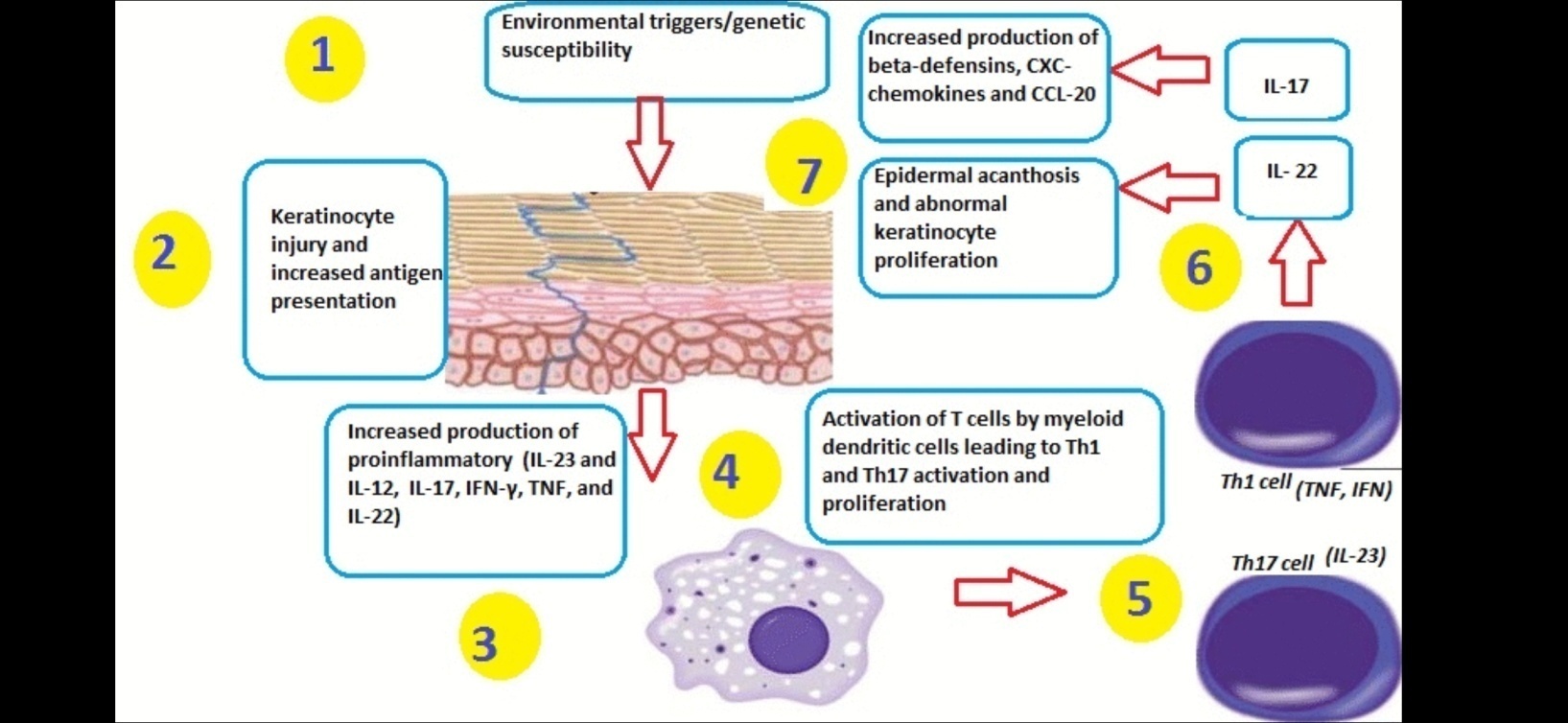
PATHOGENESIS:
Psoriasis is characterised by 3 main pathogenic features: Abnormal differentiation; keratinocyte hyperproliferation; and inflammation. Maintenance of psoriatic lesions is considered an ongoing autoreactive immune response. [5]
CLINICAL MANIFESTATION[5]
Pruritus is reasonably common, especially in scalp and anogenital psoriasis.
Skin lesions- The classic lesion of psoriasis is a sharply marginated erythematous papule with a silvery-white scale.
Scales are lamellar, loose, and easily removed by scratching. Removal of scale results in the appearance of minute blood droplets (auspitz sign ). Papules grow to sharply marginated plaques with lamellar scaling that coalesce to form polycyclic or serpiginous patterns.
May occur anywhere on the body but there are classic predilection sites palms and soles, scalp, face, anogenital, nails.
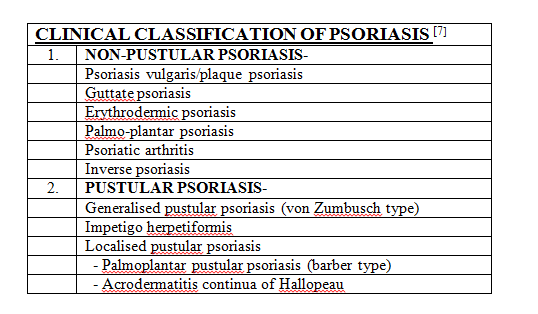
DIAGNOSIS[7]
Psoriasis is a chronic, multisystem inflammatory disease with predominantly skin and joint involvement. The diagnosis is primarily clinical and a skin biopsy is seldom required. Clinical presentation of various types are as follows-
Psoriasis vulgaris or plaque psoriasis- it is symmetric erythematous plaques with sharp boundaries and covered with pearlescent squamae, localised on knees, elbows, scalp, and sacral region.
Guttate psoriasis- Lesions appear like small droplets, or as squamous psoriatic papules, are generally seen on the trunk, proximal part of extremities, face, and scalp.
Erythrodermic psoriasis- erythematous lesions with indistinct desquamation.
Palmoplantar psoriasis- presents as pinkish-yellow erythema, symmetrically over palms and soles, mostly involves thenar than hypothenar regions.
Psoriatic arthritis- arthritic symptoms with nail involvement are present along with psoriasis.
Inverse psoriasis- Lesions manifest as bright red, symmetric, fissured plaques with sharp contours are diagnostic
Generalised pustular psoriasis- It onsets suddenly on an erythematous, is rarely seen and progresses with pustules.
Impetigo herpetiformis- It is characterised by erythrematous lesions covered with pustules, which start and radiate from flexural regions and have tendency to agglomerate.
Localised pustular psoriasis
1) Pustular psoriasis of the barber type: it is 2–4 mm-sized pustules localised on palmoplantar region, especially erythematous thenar and hypothenar regions.
2) Acrodermatitis continua: It is a sterile pustular eruption involving fingers and toes.
MANAGEMENT
Many effective treatment options are available for psoriasis. For initial treatment of mild to moderate cases of the disease topical therapy is the standard option. If diseases do not respond to such treatment then dermatological assessment should be done where systemic therapy with topical adjunct might be suitable.[8]
Conventional treatment
Conventional treatment includes : topical agents like emollients, corticosteroids, vitamin D agonists, weak tar or preperations; UV therapies like UVP or PUVA; and systemic agents like immunosuppressives[5]
Homoeopathic management
Organon of Medicine
Dr Hahnemann states (aphorism 5), homoeopathy treats the patient as a whole and constitution is taken into consideration, while selection of remedy. Constitutional diagnosis is done by proper case taking of a patient and following points should be considered physical makeup, temperament, thermals, physical generals, miasm, diathesis, susceptibility, etc.
In his writings, Dr Hahnemann (aphorisms 224,225) mentioned about mental and emotional diseases which are one-sided in nature and can lead to physical symptoms due mental causes like stress or vice-versa.[9] The main cause of such diseases which act as an obstacle to cure is fundamental cause or psora.
Psoriasis is a tri-miasmatic disease covering all the three miasms, namely psora, sycosis, and syphilis but predominantly psoro-sycotic[10]
Psoric skin lesions are dry, rough, dirty, unhealthy skin with or without pus and blood, voluptuous itching and burning, eruptions are papular in form with intense itching, the scales and crusts are thin, light, fine and small. Itching is more frequent, unbearable, late in the evening, before midnight, heat of bed, cracks in the hands and feet.[10][11]
Sycotic skin lesions are localised or in circumscribed spots, skin is oily which peels off and scaly in character. Psoriasis has the gouty element[10][11]
Syphilitic skin lesions are oily and greasy, eruptions are observed about joints, flexures surface of the body or arranged in circular group, scales and crusts are very thick and heavy, and on scalp they are patchy or in circumscribed spots, fish like scales.[12]
Rubrics related to psoriasis
Some rubrics indicative of psoriasis are mainly found in skin, head, back and extremities chapter in synthesis repertory. These are-
SKIN,eruption,psoriasis
HEAD,eruptions,psoriasis
BACK,eruptions,psoriasis,patches
EXTREMITIES,joints,psoriatic
Some other rubrics in synthesis repertory are found in different chapters of face, ear, abdomen, chest under sub-rubric eruptions, and sub-sub-rubric scales[13]
Homoeopathic medicines for psoriasis-
According to some studies most affective drugs in cases of psoriasis are Arsenicum album, Calcarea carbonicum, Hydrocotyle asiatica, Ignatia amara, Kalium arsenicosum, Lycopodium clavatum, Natrum muriaticum, Nux vomica, Opium, Petroleum, Psorinum, Sepia officinalis, Sulphur, Thyroidinum, Tuberculinum.[12]
Indication of some medicines[14]
Arsenicum iodatum – it is preferred in persistently irritating, corrosive discharges with debilitating night sweats. Lesions are dry, scaly, itching with marked exfoliation of skin in large scales, leaving a raw exuding surface beneath.
Chrysarobinum – it is used successfully in skin diseases especially in ringworm, psoriasis, herpes, acne rosacea. Vesicular or squamous lesions, associated with foul smelling discharge and crust formation, tending to become confluent and to give the appearance of a single crust covering the entire area. There is violent itching on thighs, legs and ears. Presence of dry, scaly eruption, especially around eyes and ears, scabs with pus underneath.
Graphites – Skin is rough, hard, persistent dryness unaffected by eczema. Eruptions which ooze out a sticky exudation with rawness in bend of limbs, groins, neck, behind ears. Ulcers discharging a glutinous fluid which is thin and sticky. Skin is unhealthy and every little injury suppurates.
Kalium arsenicosum – Intolerable itching, worse while undressing. Dry, scaly, wilted. Acne; pustules worse during menses. Chronic eczema; itching worse from warmth, walking, undressing. Psoriasis, lichen. Phagedenic ulcers. Fissures in bends of arms and knees. Worse on change of weather.
Kalium bromatum- Itching in lesions which are worse on chest, shoulders, and face. There is anaesthesia of skin along with profound melancholic delusion, religious depression and night terrors.
Manganum aceticum – Suppuration of skin around joints with red, elevated spots with itching better by scratching. There are deep cracks in bends of elbows with burning.
Petroleum- Itching at night. Skin is dry, constricted, very sensitive, rough and cracked, leathery, thick, greenish crusts, with burning, itching and cracks that bleed easily.
Thyroidinum- very dry skin without eruptions, psoriasis with adiposity and peeling of skin of lower limbs.
CONCLUSION
Psoriasis is not just a skin disease, but it results from faulty functioning of the immune system. Certain genetic predisposition makes one prone to psoriasis. It also affects the psychology of the individual affecting the quality of their life. Homoeopathy treats the individual as a whole not only the bodily configuration of the individual but also the intellectual and emotional attributes as revealed to us through his reaction to environment. Homoeopathic medicines have the potential to stimulate the body’s natural healing capacity and restore its normal functioning. Psoriasis cases can be managed effectively by well-selected homoeopathic medicines which are selected by thorough case taking on the basis of totality of medicine.
References
- Griffiths, C. Et al. Rook’s Textbook of Dermatology, Ninth Edition, Published by John Wiley & Sons, 2016, chapter 35, Pg no. 35.1
- Dogra S, Yadav S. Psoriasis in India: Prevalence and pattern. Indian J Dermatol Venereol Leprol [serial online] 2010 [cited 2020 Dec 30];76:595-601. Available from: https://www.ijdvl.com/text.asp?2010/76/6/595/72443
- Dogra S, Mahajan R. Psoriasis: Epidemiology, clinical features, co-morbidities, and clinical scoring. Indian Dermatol Online J. 2016 Nov-Dec;7(6):471-480. doi: 10.4103/2229-5178.193906. PMID: 27990381; PMCID: PMC5134160.
- Langley RGB, Krueger GG, Griffiths CEM Psoriasis: epidemiology, clinical features, and quality of life Annals of the Rheumatic Diseases 2005;64:ii18-ii23.
- Wolff, K. Et.al. Fitzpatrick’s color atlas and synopsis of clinical dermatology sixth edition, Published by Mc Graw Hill companies inc. 2009, Pg no. 53,54
- Pathophysiology of psoriasis-google search 11:06pm19.09.2021 https://s3.amazonaws.com/static.wd7.us/4/45/Psorpatho.gif
- Sarac G, Koca TT, Baglan T. A brief summary of clinical types of psoriasis. North Clin Istanb. 2016 Jun 14;3(1):79-82. doi: 10.14744/nci.2016.16023. PMID: 28058392; PMCID: PMC5175084.
- Kim WB, Jerome D, Yeung J. Diagnosis and management of psoriasis. Can Fam Physician. 2017 Apr;63(4):278-285. PMID: 28404701; PMCID: PMC5389757.
- Hahnemann S. Organon of medicine, 5th & 6th edition combined: B.Jain Publishers, Delhi 2016
- Banerjea Kumar S. Miasmatic prescribing, second extended edition B.jain publishers, 2010
- Choudhury H. Indications of Miasm, second edition, B. Jain Publishers, 2005
- Manchanda R.K. Et.al. Evaluation of homoeopathic drugs of psoriasis, CCRH quarterly bulletin http://aohindia.in/xmlui/bitstream/handle/123456789/3095/Evaluation.pdf?sequence=1&isAllowed=y
- Software radar 10.5.003, Synthesis Repertory version 8.1
- Boericke W. Boericke’s New Manual of Homoepathic Materia Medica with Repertory, 9th edition, B. Jain Publishers, 2011.
About Author:
Dr Madhurima Ved,
PG Scholar,
Department of Materia Medica & Therapeutics,
DYPHMCRC, Pune, Maharashtra