ABSTRACT
Protein Energy Malnutrition – PEM is a range of pathological conditions arising from coincident lack, in varying proportion, of protein and calories occurring most frequently in young children and infants and commonly associated with infection. This article reviews about types of malnutrition, classification, indicators, epidemiology, clinical features, prevention, general management and its homeopathic management.
KEYWORDS
Protein energy malnutrition, kwashiorkor, marasmus, homeopathic management
ABBREVIATION
PEM-Protein Energy Malnutrition, WHO-World Health Organization
INTRODUCTON
Protein energy malnutrition can be defined as the impaired growth primarily due to inadequate intake food. Deficiency can be in both macronutrients and micronutrients.it is most wide spread condition affecting health of children, it makes the child more susceptible to infection, recovery is slower and mortality is higher and these children shall have reduced physical and mental health.
EPIDEMOLOGY
The prevalence of stunting among under five children India is 48% and wasting is 20% and with an underweight prevalence of 43%, it is highest in the world.
DETERMINANTS OF PEM
Environmental factors including the physical and social environment, behavioral factors, healthcare services related, biological factors and socio cultural factors including improper feeding technique and nutritional status of the mother.
CLASSIFICATION
Table1:WHO classification of malnutrition based on mid-arm circumference
|
Normal |
13.5cm-16cm |
|
Mild to moderate |
12.5cm-13.4cm |
|
Severe |
Less than12.5cm |
INDICATORS
Table2: Indicators of PEM
|
Indicators |
Interpretations |
|
|
Stunting |
low height for age |
Chronic malnutrition |
|
Wasting |
Low weight for age |
Acute malnutrition |
|
Under weight |
Low weight for height |
Combination of both acute and chronic malnutrition |
TYPES
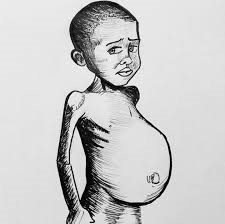
Based on the severity and onset, PEM can be of kwashiorkor and Marasmus.
Kwashiorkor occurs due to inadequate intake of proteins or energy ratio. (Fig 1.1)
Marasmus occurs due to inadequate intake of both protein and energy. (Fig 1.2)
CLINICAL FEATURES:
Difference between marasmus and kwashiorkor mentioned in table no: 3
Table 3: difference between marasmus and kwashiorkor
|
Criteria |
Marasmus |
Kwashiorkor |
|
Appearance |
Old man appearance, skin and bones, generalized wastingLoss of buccal pad of fat creates aged look referred to as monkey facies Baggy pant appearance refers to loose of skin of the buttocks hanging down |
Mooning of face, dependent oedema, upper limb wasted referred asFat sugar baby appearance |
|
age-group |
Infants |
1-5years |
|
Prevalence |
Common |
rare |
|
Weight |
Less than 60% |
60-80% |
|
growth retardation |
Present |
Mild |
|
Oedema |
Nil |
Present |
|
Mood |
Usually alert |
Irritable |
|
Appetite |
Good |
very poor |
|
Hair changes |
nil/mild |
Flag sign- alternate bands of hypo pigmented and normally pigmented hair |
|
Skin changes |
nil/mild |
Increased pigmentation, desquamation, dyspigmentation resembling flaky paint |
|
Infections |
Less prone |
More prone |
|
Recovery |
Early to recover |
Long to recover |
PREVENTION:
Promote early contact between mother and child
Promote correct breast feeding
Appropriate micro nutrient rich complementary food at 6 months of age
Identify children at risk of PEM and provide adequate social and health support
Basic health facilities to children to prevent infection
GENERAL MANAGEMENT
Daily intake of at least 150 kcal/kg/day
Frequent and appropriate feeding
Protein intake of 3g/kg/day
Include milk, oil and vegetables in diet
HOMEOPATHIC MANAGEMENT
Biochemic remedies
According to Dr. Schussler’s theory, any disturbance in the in the molecular motion of these cell salts in living tissues, caused by a deficiency in the requisite amount, constitute disease, which can be rectified and requisite equilibrium re-established by administering the same mineral salts in small quantities.
Calc-carb: Marasmus, defective nutrition, voracious appetite, swollen abdomen, craving for indigestible things, delayed dentition and learning to walk. Rapid emaciation with harsh and dry skin, unhealthy skin, the debility and irritable.
Calc-phos: Children anemic, emaciated and unable to stand. Large heads, defective bony development, open fontanelles and suture remain open too long, weak spine, curved, thin neck. Delayed teething and slow in learning to walk, Sallow complexion, sunken and flabby abdomen.
Mag-carb: Emaciation more marked in the back of head. Sallow complexion, undigested vomiting; griping and colicky pains; sour green grassy stools, improperly nourished; bloated abdomen and muscles flabby. Mentally irritable, puny and sickly in appearance.
Natrum-mur: Marasmus from defective nourishment, thin neck, ravenous appetite, losing of flesh while living well. Throat and neck of children emaciate rapidly during summer complaints. Craving for salty food and salt.
Silicea: Deficient and impaired nutrition, imperfect assimilation; rachitic and scrofulous child with large head open fontanelles and sutures, offensive sweat, distended abdomen and weak ankles; late learning to walk; late dentition.
Dynamized medicines:
Abrotanum: Marasmus of children with marked emaciation, especially of legs, skin is flabby and loose in folds, ravenous hunger, losing flesh while eating well.
Iodum: profound debility and great emaciation, ravenous hunger; eats freely and well, yet loses flesh all time, distended abdomen full of gas.
Tuberculinum: physically weak, emaciation of whole body which is rapid and highly pronounced; lose of flesh while eating well.
Sulphur: scrofulous children; emaciated and pot bellied, baby has dirty and filthy look, weak, tall, stoop shouldered and suffers from morning diarrhea.
Sarsaparilla: great emaciation; skin becomes shriveled or lies in folds.
Sanicula: emaciation; progressive; child looks old, dirty greasy and brownish, skin about neck wrinkled and hangs in folds.
BIBLIOGRAHY:
- GHAI Essentials of Pediatrics, 7th edition, CBS publishers and distributors Pvt.Ltd.
- Achar’s textbook of Pediatrics, 4th edition
- E Elizabeth, Nutrition and Child Development
- Park’s textbook of preventive and social medicine, 24th edition, Banarsidas Bhanot publishers.
- Allen H.C.; Keynotes Rearranged and Classified with leading remedies of the Materia Medica and Bowel Nosodes including reportorial index, 10th edition, B. Jain publishers (p)Ltd.
- Boericke & Dewey; The Twelve Tissue Remedies of Schussler comprising of The Theory, Therapeutic Application, Materia Medica & A Complete Repertory of Tissue Remedies, 6th edition, Jain publishers(p)Ltd.
- William Boericke, Pocket manual of Homeopathic Materia Medica & Repertory, 9th edition, Jain publishers (p)Ltd.
- K. Dubey, Text book of Materia Medica, 1st edition, Arunabha Sen Books and Allied (p) Ltd.
- DT Bhutia-Journal of Family Medicine Primary Care, 2014- ncbi.nlm.nih.gov
Searching Tags: Protein Energy Malnutrition, Protein Energy Malnutrition Examples, Protein Energy Malnutrition Classification, Homeopathic Management for Protein Energy Malnutrition