Abstract
Menorrhagia in adolescent girls is a common yet distressing clinical condition, often influenced by hormonal, physical, and emotional factors. This case study highlights an evidence-based homeopathic approach to managing menorrhagia triggered by acute emotional trauma, specifically fear following a distressing incident. The case demonstrates the importance of understanding the psycho-emotional state of the patient and selecting an individualized remedy based on the totality of symptoms.
Introduction
Homeopathy emphasizes the role of emotional and mental causative factors in disease manifestation. Fear, shock, and emotional trauma are well-recognized triggers that can disturb the menstrual cycle, particularly in sensitive adolescent girls.
Menorrhagia is defined as cyclical menstrual bleeding occurring at normal intervals but with excessive duration or quantity.
Blood loss >80 ml per cycle, or
Menstrual duration >7 days, or Both
Normal Menstrual Parameters
Parameter Normal
Cycle length 21 TO 35 days
Duration of flow 3 TO 7 days
Blood loss 30 TO 80 ml
A. Organic Causes
1. Uterine Causes
- Fibroid uterus (especially submucous fibroid)
- Adenomyosis
- Endometrial polyp
- Endometrial hyperplasia
- Endometrial carcinoma
2. Ovarian Causes
- Estrogen-secreting tumors
- Persistent ovarian cysts
3. Pregnancy-Related Causes
- Incomplete abortion
- Missed abortion
- Ectopic pregnancy
- Gestational trophoblastic disease
4. Pelvic Infections
- Endometritis
- Pelvic inflammatory disease (PID)
B. Dysfunctional Uterine Bleeding (DUB)
DUB is diagnosed when no organic pathology is found.
Types:
1. Ovulatory DUB
- Common in reproductive age
- Due to corpus luteum defect
- Prolonged estrogen stimulation
2. Anovulatory DUB
- Common in adolescence and perimenopause
- Due to unopposed estrogen
- Irregular and heavy bleeding
C. Systemic Causes
- Hypothyroidism
- Bleeding disorders (e.g., Von Willebrand disease)
- Liver disease
- Renal disease
D. Latrogenic Causes
- IUCD (Copper-T)
- Hormonal imbalance due to contraceptives
- Anticoagulant therapy
Pathophysiology
Menorrhagia results from one or more of the following mechanisms:
- Increased endometrial surface area
- Hormonal imbalance (estrogen excess)
- Defective prostaglandin metabolism
- Impaired myometrial contraction
- Local vascular abnormalities
Clinical Features
Excessive menstrual bleeding
Passage of clots
Prolonged periods
Fatigue and weakness
Symptoms of anaemia:
Pallor
Breathlessness
Palpitations
Investigations
- General Investigations
- Hemoglobin estimation
- Complete blood count
- Thyroid function tests
- Coagulation profile (if indicated)
- Imaging
- Ultrasonography (Pelvis)
- Saline infusion sonography (SIS)
Case
- Patient Details
- Name: ABC
- Age: 12 years
- Sex: Female
- Date of Consultation: 24 August 2023
- Chief Complaint
The patient presented with prolonged menstrual bleeding. Her last menstrual period (LMP) started on 15 August 2023, and bleeding was ongoing at the time of consultation.
- Menstrual History
- Duration: Prolonged bleeding
- Character of blood: Dark red
- Clots: Present (+++)
- Pad usage: 3–4 pads per day
- Investigations
The patient had undergone an USG (Abdomen + Pelvis) prior to consultation, which revealed:
Mild endometrial thickening
Endometrial thickness: 11.3 mm
History of Present Illness
According to the mother, the bleeding initially decreased around the 7th day but subsequently increased again. In the previous menstrual cycle, bleeding started on 26 July 2023 and lasted 6 to 7 days, with heavy bleeding during the first three days followed by gradual reduction.
On further inquiry, a significant emotional incident was revealed. Two to three days prior to the increase in bleeding, the patient experienced a traumatic event while returning from coaching classes.
Emotional and Mental State
The patient reported that an unknown man followed her, came very close, touched her inappropriately, and then disappeared into a nearby street. She expressed intense fear that he might abduct, rape, or kill her. During narration, the patient broke down and cried.
She described herself as extremely sensitive and timid, with a tendency to cry easily. She finds it difficult to express herself, especially in confrontational situations. Even minor emotional disturbances, such as a friend not sharing secrets – make her cry.
She also expressed emotional sensitivity related to relationships, noting that while her best friend has a male friend and shares experiences with her, she herself does not have any male friends.
- Physical Generals
Thermal reaction: Chilly
Desire: Spicy food
Thirst: Thirstless
Perspiration: Scanty
Bowel habits: Constipation with hard stool, passed with difficulty
Flatus: Offensive (++), since one week
Sleep: Sound
Dreams: Non-specific
Analysis and Evaluation of Symptoms
The totality of symptoms indicated the need for a remedy covering the following key aspects:
- Fear of being raped
- Timid disposition
- Weeping tendency
- Hemorrhagic diathesis
- Hypersensitivity to external impressions
- Emotional and sexual sensitivity
Repertorization and Remedy Selection
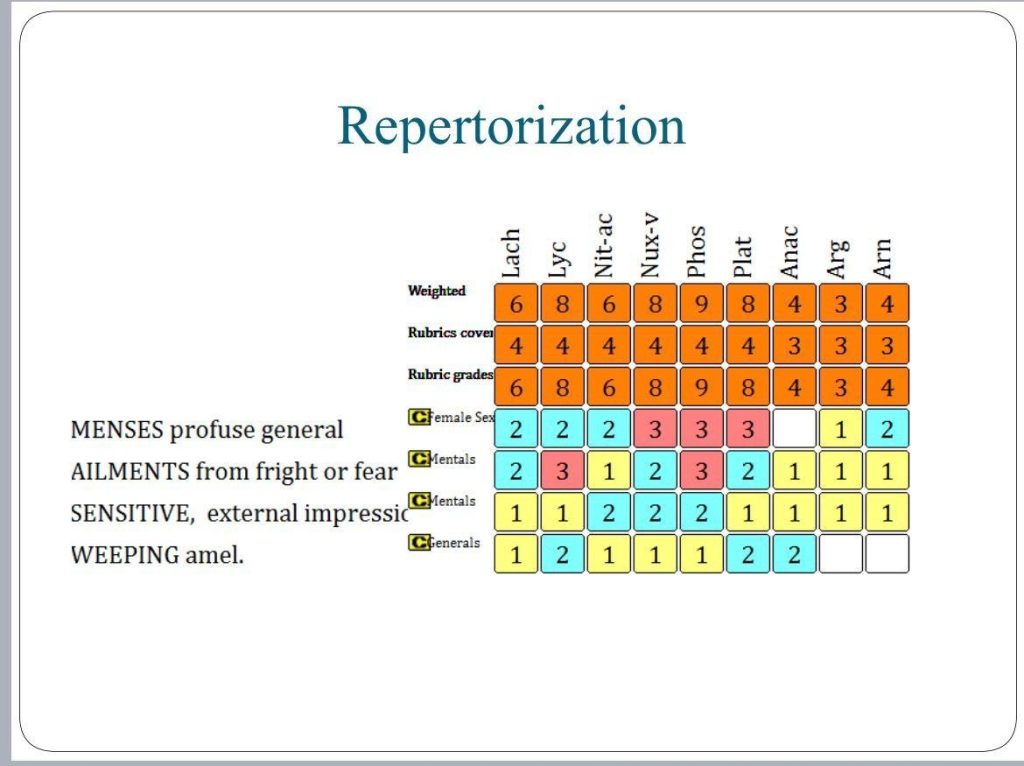
Based on repertorial analysis and individualization, Cenchris was selected as the constitutional remedy from reference of Materia medica.
Prescription
Cenchris 200 Single dose
Rubrum 4 pills, twice daily, for one week
Follow-Up and Outcome
Within one week of treatment:
Menstrual bleeding gradually reduced and stopped completely
The patient reported feeling energetic and fresh
Emotional state showed noticeable improvement
Conclusion
This case highlights the profound impact of emotional trauma on menstrual health in adolescents. Homeopathy, through individualized remedy selection based on mental and physical totality, can offer gentle yet effective management of menorrhagia triggered by fear. Addressing the emotional causation proved crucial for sustained recovery in this young patient.
Acknowledgement
We express our sincere gratitude to our mentors and guides for their blessings and support, and pay homage to Dr. Samuel Hahnemann, whose principles continue to guide us in holistic healing.
References
1. D.C. Dutta’s Textbook of Gynaecology
2. Shaw’s Textbook of Gynaecology
3.Kent JT. REPERTORY OF THE HOMOEOPATHIC MATERIA MEDICA NEW DELHI: B. JAIN PUBLISHERS (P) LTD.; 2014.
Co-Author –Dr. Dipti Mevada
MD Homoeopathy Scholar (Practice of Medicine)