
Abstract:
The most prevalent cause of infectious oesophagitis is oesophageal candidiasis. Of patients that have infectious oesophagitis, 88% are from candida albicans. Candida infections of the esophagus are considered opportunistic infections and are seen most commonly in immunosuppressed patients. A case is presented in this paper with radiological evidence of candida infection noted in the esophagus with positive Rapid Urease Test. Malignancy and HIV were excluded. The patient was treated with constitutional homoeopathic medicines – Nux vomica 0/1, 16 doses up to Nux vomica 0/4 16 doses each. Follow-up imaging at 5 months showed complete resolution of the oesophageal candidiasis. This case report suggests homoeopathic treatment as a promising complementary or alternative therapy and emphasises the need of repertorisation in individualised homoeopathic prescription.
Keywords
Oesophageal candidiasis; quality of life; homoeopathy; case report.
Abbreviations
HIV: human immunodeficiency virus, AIDS: acquired immunodeficiency syndrome, HARRT: highly active antiretroviral therapy, OPD: outpatient department, aqua dist.: distilled water, RUT: rapid urease test, HPUS: United States Homoeopathic Pharmacopoeia, PDF: potential differential field.
Introduction:
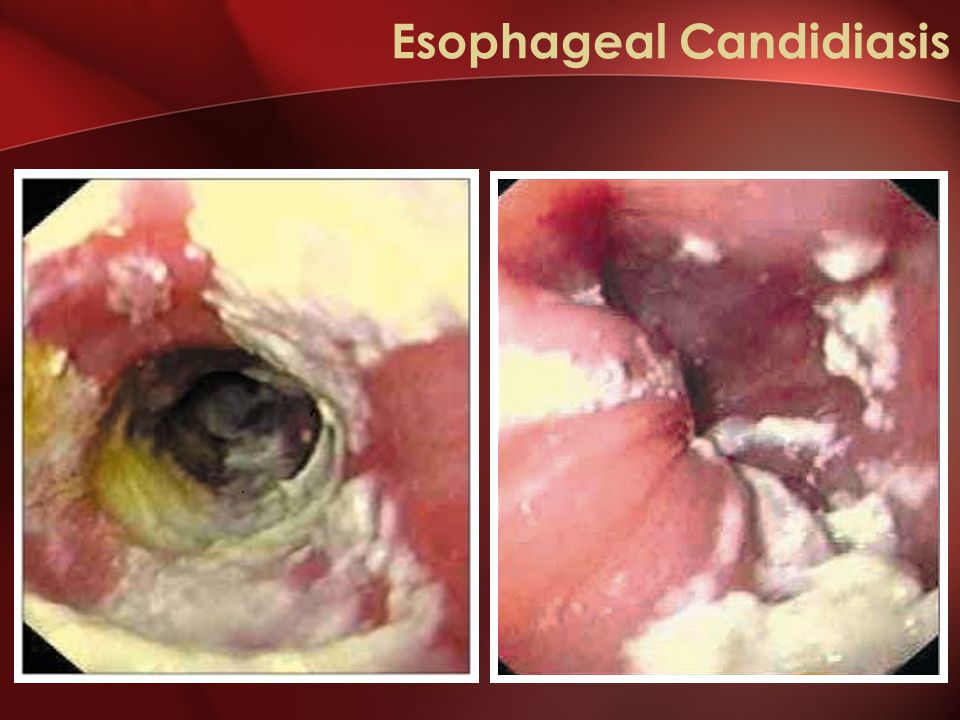
The most prevalent cause of infectious oesophagitis is oesophageal candidiasis. Of patients having infectious oesophagitis, 88% are from candida albicans1. The most common symptoms include dysphagia, odynophagia, and retrosternal pain. Candida infections of the esophagus are considered opportunistic infections and are seen most commonly in immunosuppressed patients. Candida can be part of the normal oral flora. When host defense mechanisms are impaired, this allows for a proliferation of candida on the oesophageal mucosa forming adherent plaques.1, 2
The highest risk factor for developing oesophageal candidiasis is impaired cell-mediated immunity. Immunosuppressed patients at risk for oesophageal candidiasis include HIV positive and AIDS patients, chemotherapy patients, antibiotic therapy, patients on chronic systemic or topical inhaled corticosteroids, diabetes mellitus, and advanced age.1, 2
The prevalence of oesophageal candidiasis in HIV-infected patients appears to be decreasing due to the effectiveness of highly active antiretroviral therapy (HARRT) 4. However, the incidence in non-HIV patients appears to be increasing, possibly due to co-morbidities such as diabetes mellitus or from medications such as antibiotics and corticosteroids. Some studies show that smoking tobacco also correlates with developing oesophageal candidiasis.2, 3, 4
Diagnosing oesophageal candidiasis is via upper gastrointestinal endoscopic evaluation. Visualising the candida on the oesophageal mucosa as white plaques or exudates confirms the diagnosis. There may also be mucosal breaks or ulcerations. Biopsies of the plaques can undergo testing for histological confirmation of the infection.1
Evidences in support of individualised homoeopathic treatment of oesophageal candidiasis remains compromised; not a single case report could be identified after a careful search in different electronic databases.
Case study:
A female patient, aged 48 years, residing in Gosaba, West Bengal came to the outpatient department of National Institute of Homoeopathy on August 3, 2018 (OPD No. 549882/18) with complaints of aching pain and heaviness of left side of upper abdomen since 8 years which are aggravated after eating with sour eructation and relief after drinking water. There was a concomitant symptom of burning pain in lower abdomen since 3 years, aggravated in empty stomach.
History of presenting complaints: Onset gradual, duration 8 years, aching pain in left side of upper abdomen with sour eructation, aggravates after eating and relief by taking cold water, history of allopathic treatment without any remarkable improvement.
Past history: Ringworm (tinea corporis) at the age of 31 years.
Family history: Father having breathing difficulty (bronchial asthma?)
Physical generals:
- Appetite normal, preferred hot food, sour test in mouth.
- Thirst less, drank little in long intervals.
- Desire for sour spicy food, fatty food, meat.
- Intolerance of milk.
- Urine frequent, clear, offensive.
- Stool regular, sometimes mucoid.
- Sleep adequate.
- Dreams of eating.
- Tongue dry with scanty salivation.
- Thermal reaction: hot patient.
- Menstruation irregular, stays for 3-4 days; black clotted.
- Perspiration moderate, offensive with black staining.
Mental generals: Easily irritable, expressive only at home, mild, desire for company.
Totality of symptoms5:
- Desire for company.
- Expressive only at home.
- Easily irritable.
- Desire for spicy food, fatty food, meat.
- Intolerance of milk.
- Pain in left side of upper abdomen with sour eructation.
- Past history of ringworm.
Prescription: After considering totality of symptoms, prescribed Nux vomica 0/1 16 doses in 100 ml aqua dist, one dose every morning in empty stomach. But after completion, some symptoms remain as before. So the case was retaken, followed by evaluation and repertorisation.
Timeline: Radiological imaging was done twice during the period of treatment, on March 11, 2018 and August 25, 2018.
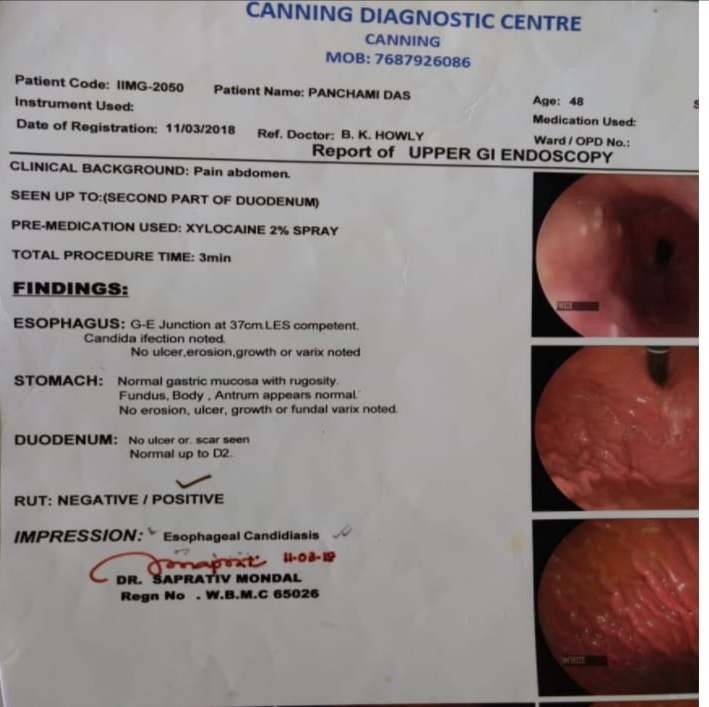
| Upper gastroesophageal endoscopy on March 11, 2018 shows oesophageal candidiasis with positive RUT |
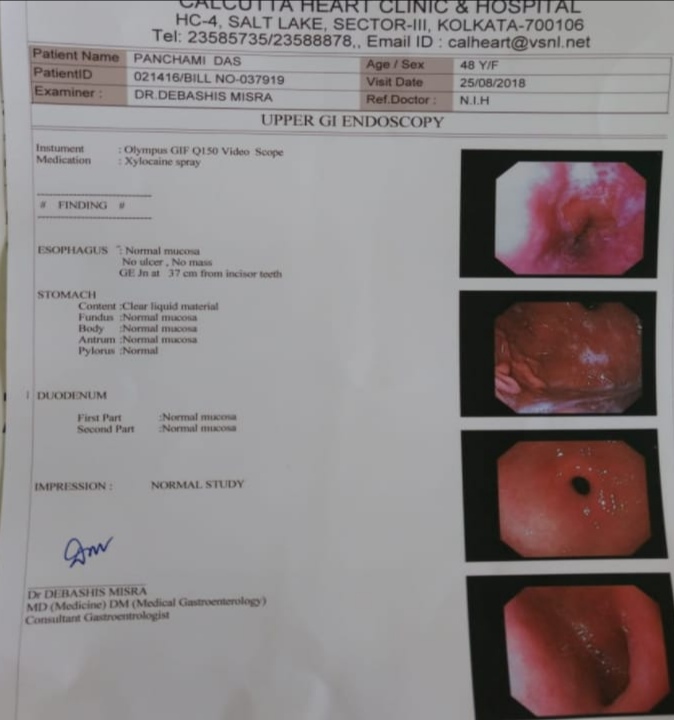
| Upper gastrointestinal endoscopy on August 25, 2018 showed normal study |
Evaluation of symptoms:
- Mental generals: desire for company, irritability ++.
- Physical generals: desire for fatty food, desire meat, easily satiety of food, aversion to milk, perspiration of offensive odour.
- Characteristic particulars: aching pain in left side of upper abdomen with sour eructation since 5 months.
Repertorial sheet:
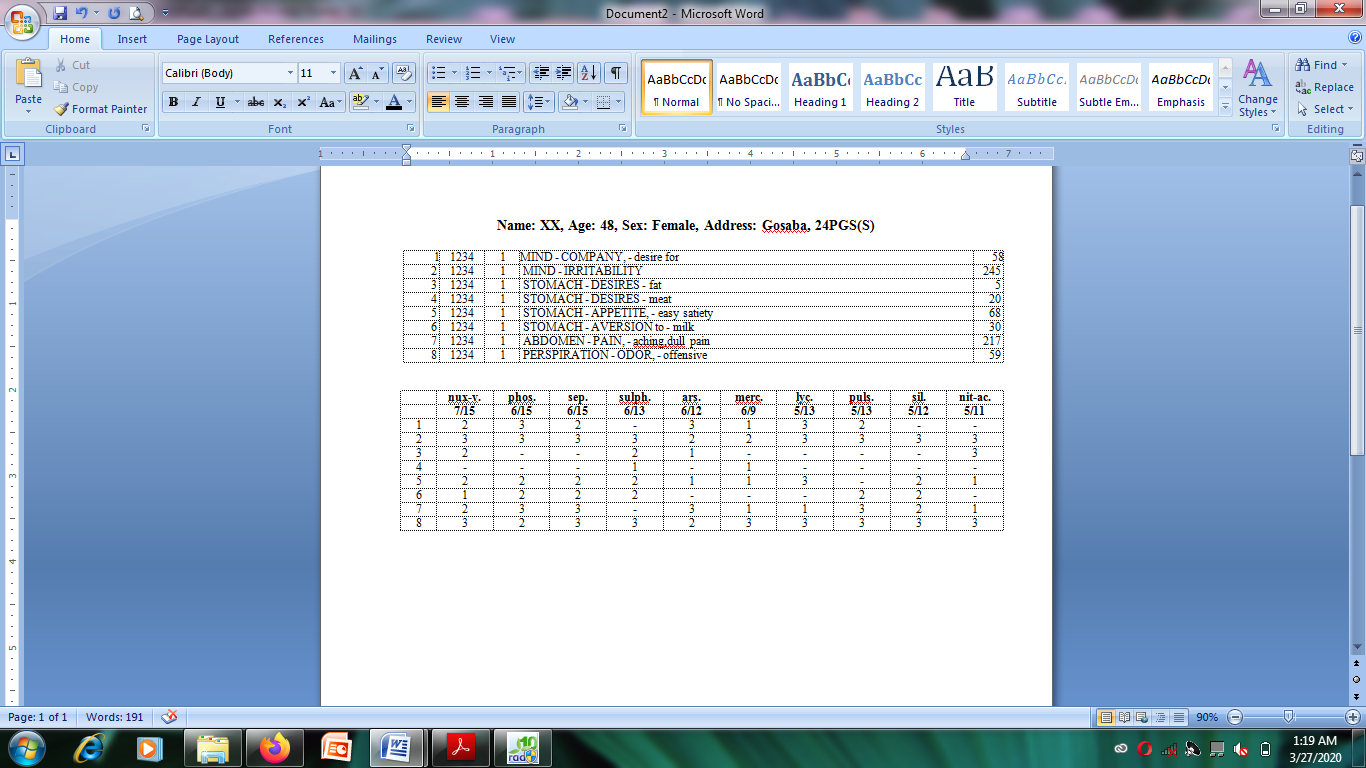
This case was repertorised using the software RADAR®, using Kent’s Repertory5. The reportorial results were analysed giving more importance on the mentals as well as physical general symptoms than particular symptoms for selection of medicine. Fortunately, repertorisation showed highest grade medicine was Nux vomica which already prescribed. Then in subsequent follow-ups from August 11, 2018 to August 27, 2018, potency was gradually increased up to 0/4 with gradual improvement in symptoms with a general improvement.
Assessment by modified Naranjo score:
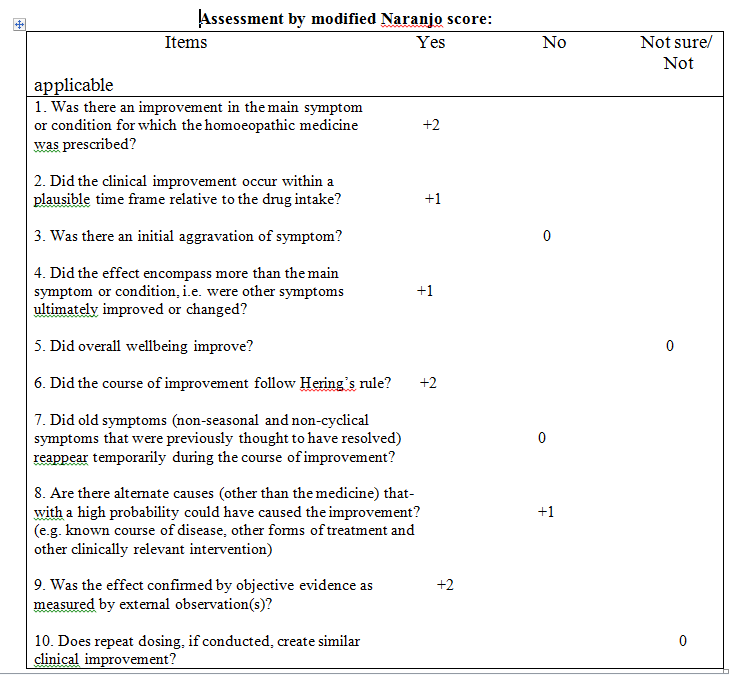
The final causal attribution score in this case was assessed using the modified Naranjo criteria, as proposed by the HPUS clinical data working group, June 20146. The total score was 8, thus suggesting a “probable” association between the medicine and the outcome
. Reporting of this case adhered to the hom-CASE-CARE guideline7.
Conclusion:
A case presented with radiological evidence candida infection noted in the oesophagus with positive rapid urease test. The patient was treated with constitutional homoeopathic medicines – Nux vomica 0/1 – 0/4, 16 doses each. Follow-up imaging at 5 months showed complete resolution of the oesophageal candidiasis. This case report suggested homoeopathic treatment as a promising complementary or alternative therapy and emphasises the need of repertorisation in individualised homoeopathic prescription. Totality of symptoms gives the clue about the selection of medicine which has resemblance to the potential differential field (PDF), but sometimes it may mislead the plan of treatment. At this point, repertorisation is needed for confirming the selection of remedy and treating the cases in better way.
References:
- Rosołowski M, Kierzkiewicz M. Etiology, diagnosis and treatment of infectious oesophagitis. Prz Gastroenterol. 2013; 8 (6):333-7.
- Alsomali MI, Arnold MA, Frankel WL, Graham RP, Hart PA, Lam-Himlin DM, Naini BV, Voltaggio L, Arnold CA. Challenges to “Classic” Oesophageal Candidiasis: Looks Are Usually Deceiving. Am. J. Clin. Pathol. 2017 Jan 01; 147(1):33-42.
- Takahashi Y, Nagata N, Shimbo T, Nishijima T, Watanabe K, Aoki T, Sekine K, Okubo H, Watanabe K, Sakurai T, Yokoi C, Kobayakawa M, Yazaki H, Teruya K, Gatanaga H, Kikuchi Y, Mine S, Igari T, Takahashi Y, Mimori A, Oka S, Akiyama J, Uemura N. Long-Term Trends in Oesophageal Candidiasis Prevalence and Associated Risk Factors with or without HIV Infection: Lessons from an Endoscopic Study of 80,219 Patients. PLoS ONE. 2015; 10(7):e0133589.
- Choi JH, Lee CG, Lim YJ, Kang HW, Lim CY, Choi JS. Prevalence and risk factors of Oesophageal candidiasis in healthy individuals: a single center experience in Korea. Yonsei Med. J. 2013 Jan 01; 54(1):160-5.
- Kent JT. Repertory of the Homoeopathic Materia Medica and a Word Index. Enriched Indian Edition. Reprinted From 6th American Edition, Edited and Revised by Kent CL, Low Priced Edition. New Delhi; B. Jain Publishers Pvt. Ltd., 2005.
- Rutten L. Data collection: Treat every variable as a treasure. Homeopathy. 2015; 104 (3):190-196.
- Haselen V. RA. Development of a supplement (HOM-CASE) to the CARE clinical case reporting guideline. Complement Ther Med. 2016; 25:78-85.
About Author:
Preeti Verma1, Palas Ghosh1, Birendra Prasad Srivastava2, Aniruddha Banerjee*3
1. Postgraduate Trainee, Dept. of Case Taking and Repertory, National Institute of Homoeopathy, Govt. of India
2. Professor, Dept. of Case Taking and Repertory, National Institute of Homoeopathy, Govt. of India
3. Lecturer, The West Bengal University of Health Sciences, Govt. of West Bengal; Former Postgraduate Trainee, Dept. of Case Taking and Repertory, National Institute of Homoeopathy, Govt. of India



