Keywords– Individualized homoeopathic medicine, Hyperthyroidism, Case report
Abstract-
The most common presentations of thyroid diseases is Hyperthyroidism. Hyperthyroidism is defined as a disorder due to dysfunction of thyroid gland and regulation systems of thyroid hormone actions including dysfunction of the pituitary, hypothalamus or thyroid hormone receptor 1.It is well known fact that many etiological factors are responsible for the development of hyperthyroidism, but psychological and stress full life events are well known factors that play an important role in the causal relationship of development of hyperthyroidism. This case report describes a 27yrs old female presented with enlarged thyroid gland and irregular menses treated effectively with Individualized Homoeopathic Medicine Ferrum.met 200 without any conventional supplements. After case taking, individualized homoeopathic medicine was prescribed according to the totality of symptoms. The prognosis of the case was assessed by thyroid profile and symptomatic relief of the symptoms which emphasized on the documentary evidence about the effectiveness of Individualized Homoeopathic Medicine through its action on PNEI Axis and thus regulating the endocrinal dysfunction. Modified Naranjo Criteria For Homoeopathy [MONARCH] was used to assess causal relationship between homoeopathic treatment and the clinical outcome.
Introduction-
Hyperthyroidism is a term used for overproduction of the hormones secreted by the thyroid gland. It is a symptom complex arised due to raised levels of thyroid hormones2. The global prevalence of hyperthyroidism in iodine-sufficient countries is estimated at 0.2-2.5%3. The prevalence of overt hyperthyroidism, defined as low thyroid stimulating hormone [TSH] with elevated triiodothyronine [T3] and/or free thyroxine [T4], is approximately 0.2-1.4%. The prevalence of subclinical hyperthyroidism, defined as low TSH with normal peripheral thyroid hormone, is approximately 0.7-1.4%3,4. Psychological disturbances and stressful life events are well known disorders in patients with hyperthyroidism5.Recent researches have been done on psychoneuroendocrinoimmunology (PNEI) to study the intimate chemical relationship between the brain and the endocrinal glands. A close relationship between the hypothalamus and the PNEI has been demonstrated, about its inputs and outputs towards the immune system, its relationship between hormonal processes, with stress states, and with psychological processes. PNEI have demonstrated a model of research and the interpretation of health and disease emerges that sees the human body as a structured and interconnected unit, where the psychic and biological system mutually connects each other6.
Untreated hyperthyroidism can cause cardiac arrhythmias, congestive heart failure, osteoporosis, adverse obstetric outcomes, and metabolic derangements such as increased resting energy expenditure and gluconeogenesis7. Treatment in conventional system of medicine includes symptom relief, as well as therapy with antithyroid medications, radioactive iodine, or thyroidectomy. However, studies have shown that antithyroid medications are not much effective as these medications release performed thyroid hormones8. On the other hand, Homoeopathy is a system of medicine purely based on symptom similarity and individualisation. Studies reveal that in endocrine disorders, homoeopathic medicines act to stimulate the gland, in cases of deficient secretion and to quiet it in the cases of excess secretion9.Here, a case of hyperthyroidism successfully treated with individualised homoeopathic medicine based on the role of PNEI axis on the development of endocrinal dysfunction and how homoeopathic medicines are efficacious in reversing the pathological processes by reverting the psychological disturbances. To assess the improvement, levels of T3, T4 and TSH were measured and prognosis was assessed on the basis of Modified Naranjo criteria.
CASE REPORT-
Presenting complaints
Ms. SG, a 27yrs old women, had been experiencing irregular menses since1year; her menses were frequently delayed, often for 2-3 months. Her menstrual flow was profuse making her pale and weak. Flow lasted for a period of 4-5 days with bright red flow, no clots and no offensiveness. She had lost her weight 4kgs since last 1 year. She also has swelling in the anterior aspect of throat since last 6 months.
physical examination, she was afebrile, pallorness was present. Her pulse was 76/min, BP 110/60mmHg and weight 52kgs. Systemic examination does not reveal any abnormality.
Family History: No similar complaint among family members.
Past History- No past history of treatment for presenting complaint.
No history of chickenpox,dengue,malaria,typhoid etc
No surgical history .
Physical generals- Appetite reduced2+, thermally- Hot
Life situation
The patient was born and brought up in Ratnagiri. she came from a join family. During schooling she was an average student. she is very ambitious and had interest in learning beautician course and her dream was to start her own beauty parlour. Her parents wanted her to pursue Nursing and be a part of medical world for which she was never ready. She was very angry at that time and she opposed her parents and joined beautician course, which she completed within 1 year. She was very guilty for opposing her parents. But, as her parents wanted her to do nursing, she joined nursing college. Initially she was least interested in the course, but as year progressed and when she started to attend patients, she eventually started loving her profession. As a person she is very bold and confident. She gets angry if people goes against her. She is very sensitive and she gets irritable by slightest noise.
Selection of Approach
The case contains of characteristic and qualified mentals and physical symptoms hence kent`s approach was selected for this case.
Diagnostic Assessment
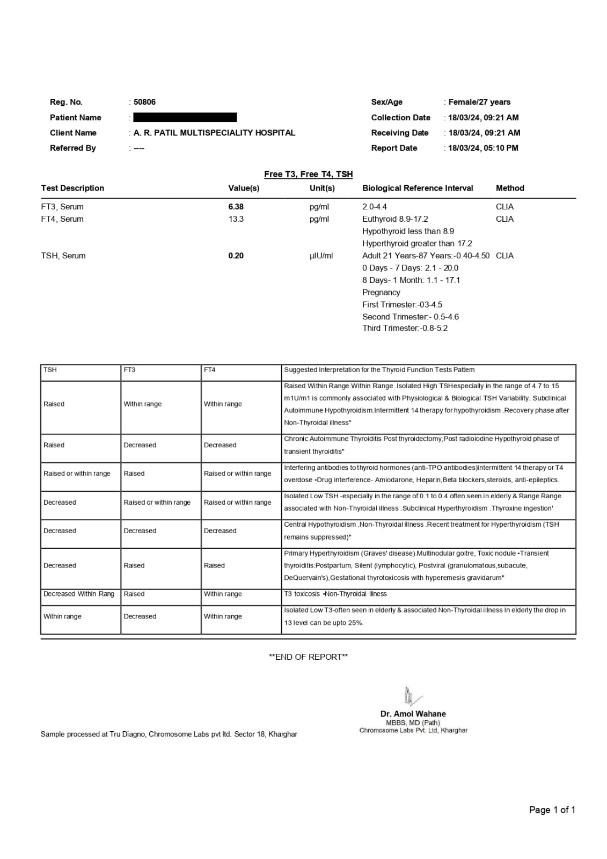
Thyroid profile and ultrasonography (abdomen and pelvis) was done by the patient. Where USG did not reveal any structural abnormality but, her thyroid profile was deranged FT3- 6.38pg/ml, FT4-13.3 g/ml, TSH- 0.20Iu/ml and the patient was diagnosed with Hyperthyroidis
Before Treatment
Diagnosis Challenges- Nothing specific
Diagnosis – HYPERTHYROIDISM
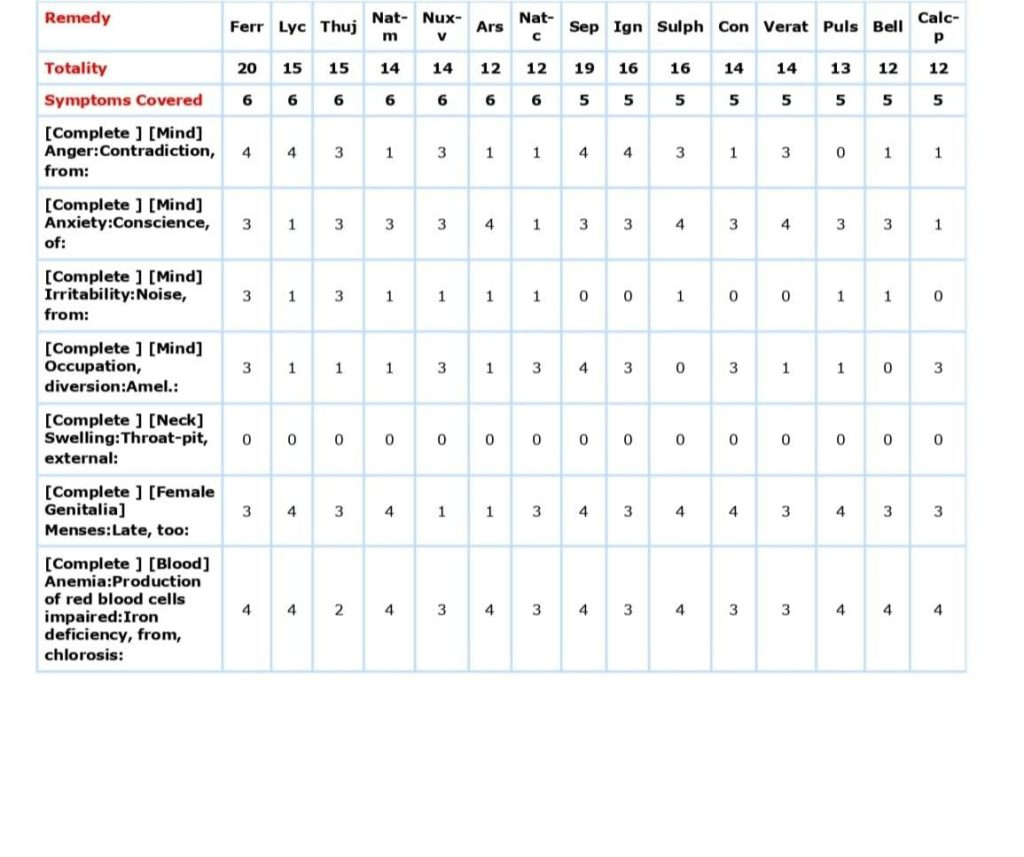
REPERTORIAL TOTALITY
- Anger contradiction from2+
- Anxiety conscience about
- Sensitiveness to noise2+
- Occupation interest in
- Swelling in the throat
- Menses irregular3+
- Chlorosis2+
After repertorisation with complete repertory, the top five remedies as per their hierarchy are as follows:
Ferr. – 20/6
Lyc.- 15/6
Thuja- 15/6
Nat-m -14/6
Nux-v -14/6
Considering the characteristic mentals of the patient, especially anger from least change of opinions of others and the anxiety due to guilt of not obeying her parents. The boldness and confidence was felt in the patient during the case taking. In this case, the central core of the patient is sensitivity which got triggered when she was compelled to do things against her wish. The final remedy selected was Ferrum.Met , so the treatment was started with Ferrum. Metallicum 200 /1 dose stat and sac.lac 30 BD for 15 days. Details of follow ups are given in Table 1.
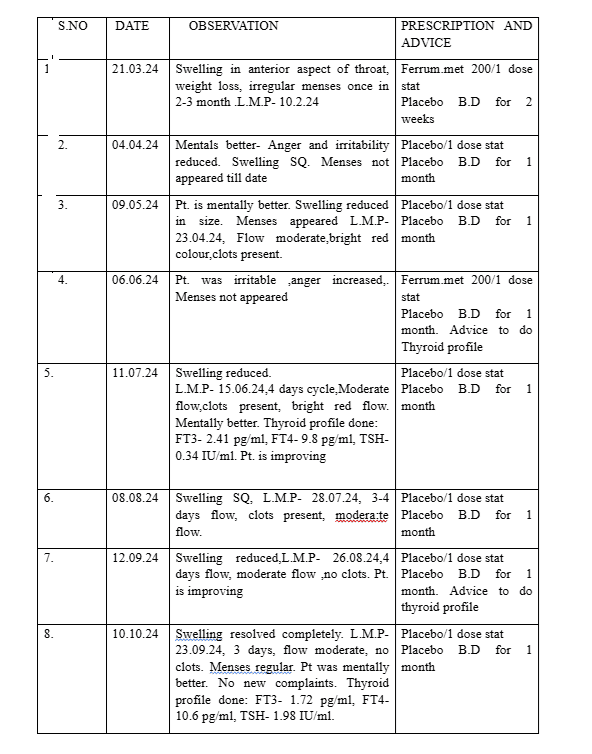
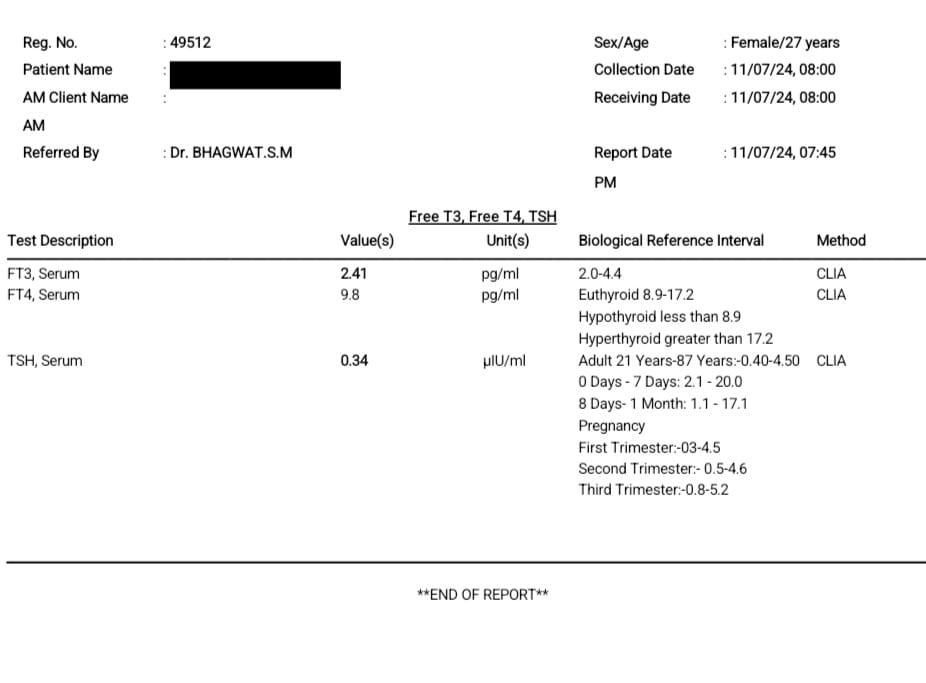
DURING TREATMENT
The final outcome was assessed on the basis of Modified Naranjo Criteria For Homoeopathy (MONARCH) which helped to gain causal relationship between homoeopathic treatment and the clinical outcome10. It has also helped to assess the prognosis of the case.
| DOMAINS | YES | NO | NOT SURE |
| Was there an improvement in the main symptom or condition for which the homoeopathic medicine was prescribed? | +2 | ||
| Did the clinical improvement occur within a plausible timeframe relative to the drug intake? | +1 | ||
| Was there an initial aggravation of symptoms? | 0 | ||
| Did the effect encompass more than the main symptom or condition(i.e where the other symptoms ultimately improved or changed)? | +1 | ||
| Did the overall well being improved? | +1 | ||
| 6A. Direction of cure: did some symptoms improve in the opposite order of the development of symptoms of the disease? | 0 | ||
| 6B. Direction of cure: did at least two of the aspects apply to the order of improvement of symptoms:From the organs of more important to those of less importance?From deeper to more superficial aspects of the individual?From the top downwards? | 0 | ||
| Did old symptoms reappear temporarily during the course of improvement? | 0 | ||
| Are there alternate causes that with high probability could have caused the improvement? | 0 | ||
| Was the health improvement confirmed by any objective evidence? | +2 | ||
| Did repeat dosing, if conducted, create similar clinical improvement? | +1 | ||
| TOTAL | 9 |
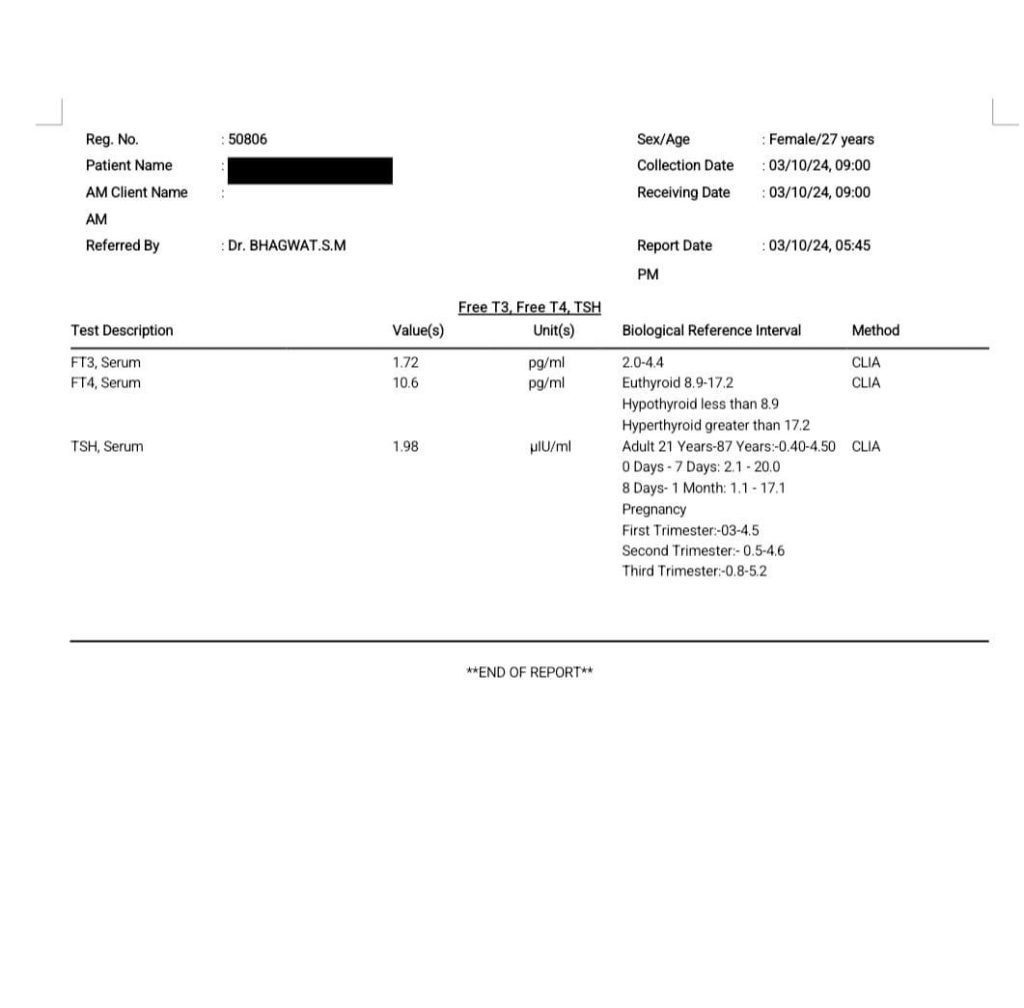
AFTER TREATMENT
Conclusion
Psychoneuroendocrinoimmunology (PNEI) is the study of intimate relationship between immune, physical, emotional and psychological aspects. PNEI is inserted as a link between medicine and psychology, with a mind-body model that includes all the physiological, emotional, psychological, behavioural, and social processes understood as an organic and unitary system: a network of systems biology6. This case report demonstrates how psychological factor or an emotional stress can cause hormonal imbalance and affect the PNEI axis and develop an endocrinal dysfunction. In this case, Modified Naranjo criteria was used in this case to assess the prognosis of the disease. The total score of outcome in this case was 9, which was close to the maximum score of 13 as per Modified Naranjo Criteria. Although, not much research have been done, in the development of hyperthyroidism due to stress and psychological factors much scientific evidences has to be collected by conducting clinical trials in this regard.
DECLARATION OF PATIENT CONSENT
Patient’s consent not required as the patients identity is not disclosed or compromised.
FINANCIAL SUPPORT AND SPONSORSHIP- Nil
CONFLICTS OF INTEREST
There are no conflicts of interest.
BIBILIOGRAPHY
1. Malarkey WB, Mills PJ. Endocrinology: the active partner in PNI research. Brain Behav Immun. 2007 Feb;21(2):161-8. doi: 10.1016/j.bbi.2006.10.008. Epub 2006 Dec 15. PMID: 17174524; PMCID: PMC2569824. https://pmc.ncbi.nlm.gov/articles/pmc2569824/
2. Goel M, Gautam P, Gogoi J. A case of hyperthyroidism treated with individualised homoeopathic medicine: A case report. J Intgr Stand Homoeopathy. 2024;7:160-5. doi: 10.25259/JISH_39_2023
3. Taylor PN, Albrecht D, Scholz A, et al. Global epidemiology of hyperthyroidism and hypothyroidism. Nature Reviews Endocrinology. 2018; 14(5):301–316. doi:10.1038/nrendo.2018.18
4. Chung JH. Update on Thyroid Hormone Levels and Thyroid Dysfunction in the Korean Population Based on Data from the Korea National Health and Nutrition Examination Survey VI (2013 to 2015). Endocrinol Metab (Seoul). 2020;35(1):7–13. doi:10.3803/EnM.2020.35.1.7 [PubMed: 32207259]
5. I-Te Lee, Wayne Huey-Herng Sheu, Yi-Ju Liau, Shih-Yi Lin, Wen-Jane Lee, Chih-Chien Lin; Relationship of Stressful Life Events, Anxiety and Depression to Hyperthyroidism in an Asian Population. Hormone Research 11 July 2003; 60 (5): 247–251. https://doi.org/10.1159/000074039
6. Bitzer-Quintero OK, Ortiz GG, Jaramillo-Bueno S, Ramos-González EJ, Márquez-Rosales MG, Delgado-Lara DLC, Torres-Sánchez ED, Tejeda-Martínez AR, Ramirez-Jirano J. Psycho-Neuro-Endocrine-Immunology: A Role for Melatonin in This New Paradigm. Molecules. 2022 Jul 30;27(15):4888. doi: 10.3390/molecules27154888. PMID: 35956837; PMCID: PMC9370109.
7. Sun Y. Lee, MD, MSc1, Elizabeth N. Pearce, MD, MSc1;Section of Endocrinology, Diabetes, Nutrition, and Weight Management, Boston University Chobanian and Avedisian School of Medicine, Boston, Massachusetts JAMA. 2023 October 17; 330(15): 1472–1483. doi:10.1001/jama.2023.19052 https://pmc.ncbi.nlm.nih.gov/articles/PMC10873132/pdf/nihms-1958909.
8. Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid. 2016;26(10): 1343–1421. doi:10.1089/thy.2016.0229 [PubMed: 27521067]
9. Pandya AL. ‘Love me only, at all times’ – The case of a young woman with hypothyroidism. J Intgr Stand Homoeopathy 2020;3(4):100-3.
10. Lamba CD, Gupta VK, Van Haselen R, Rutten L, Mahajan N, Molla AM, et al. Evaluation of the modified naranjo criteria for assessing causal attribution of clinical outcome to homeopathic intervention as presented in case reports. Homeopathy. 2020;109:191-7.
[CrossRef] [PubMed] [Google Scholar]Co Author – Dr Swati Bhagwat