Holistic Neurological Wellness Through Homoeopathy: Managing Stroke and Beyond – A Case Report
Keywords
Apoptosis, Hypertension, Thromboembolism, Arteritis, Atheroma, Coagulation necrosis, Brain attack, Ischemic Stroke, Hemorrhagic Stroke.
Abstract
The brain is arguably the most complex of all the organs in your body. These three pounds of tissue compose the major nerve center of the body, which coordinates all of our bodily functions, including behavior, thought and emotions. Because your brain is a very hard-working organ, it requires constant supplies of oxygen and nutrients from the blood to function effectively. The heart pumps blood throughout the cerebral arteries, delivering blood to the brain. Any significant interruption to this supply of nutrients and oxygen will start killing brain cells. Damage to brain cells occurs almost immediately upon cessation or even significant restriction of blood flow to the brain. Minor damage to any part of the brain can have a serious adverse effect on the rest of the body. Significant damage to the brain can even result in death.
One relatively common cause of brain damage and death is referred to as a stroke. A stroke is similar to a heart attack, only in this case, blood flow to brain, rather than the heart, is blocked. The term “stroke” comes from the once popular idea that someone had received a “stroke of God’s hand” and was therefore damaged. Strokes are also called cerebrovascular accidents or “brain attacks” to emphasize the need to call get immediate medical attention when they occur.
Arterial blood vessels feeding the brain can become blocked on a permanent or temporary basis. The term stroke is generally reserved for more permanent blockages that do not rapidly and spontaneously resolve themselves. These blockages result in permanent brain damage and leave lasting physical or mental deficits. Transient and temporary blockages are called Transient Ischemic Attacks. TIAs temporarily alter behavior and thinking (for less than 24 hours), but do not end up creating lasting brain damage. Because the damage is temporary.
Definition
The term “Stroke” defined as rapid onset of focal neurological deficit resulting from disease of cerebral vasculature and its content.
Epidemiology
A who collaborative study in to countries showed in the populations studies stroke incidence rate ranged from 0.2 to 2.5 per 1000 population per year. WHO estimate 9.4 million deaths in India in year 1990 as so increasing.
Aetiology
Total occlusion of the vessels by thromboembolism cerebral atheroma thrombosis associated with arteritis. Disturbance in Blood Brain Barrier etc.
Condition like obesity, Hypertension are also contributed in stroke. The cigarette smoking is also promoting the condition of cerebrovascular disease.
Classification
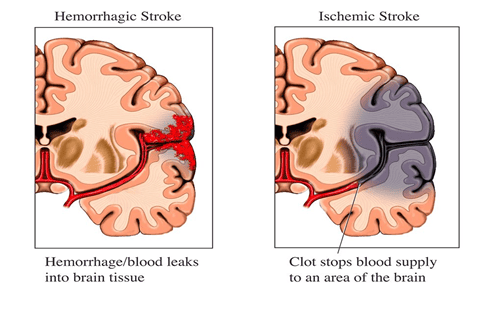
- Ischemic Stroke
- Hemorrhagic Stroke
- Strokes of undermined source.
Pathophysiology of Stroke
This brief presentation of pathophysiology of stroke reviews conditions that influence ischemic injury, mechanisms of death of neurons (coagulation necrosis vs apoptosis), cerebral blood flow and survival of brain tissue and features of hypotensive stroke. Ischemic penumbra and viability of brain tissue, and re-perfusion hemorrhage – a complication of restoration of cerebral blood flow to injured brain tissue are also explained.
Understanding of the pathogenesis of stroke is to understand how ischemia and hemorrhage cause injury. An ischemic stroke deprives neurons of oxygen and nourishment. Accumulation of noxious metabolites in the brain tissue originating from the injured or dying neurons increases with time, which then results in injury to the surrounding healthy neurons. This process can be halted or even reversed in the ischemic penumbral brain tissue if restoration of blood flow occurs within a critical time period. In hemorrhagic stroke, extra vascular release of blood causes damage by cutting off connecting pathways, resulting in local or generalized pressure injury.
Two major types of “strokes” cause brain damage: ischemic and hemorrhagic stroke. In ischemic stroke, which represents about 80% of total strokes, lack of circulating blood deprives neurons of oxygen and nourishment. The effects are fairly rapid because the brain does not store glucose and is incapable of anaerobic metabolism. Hemorrhagic stroke causes damage to brain tissue by disrupting connecting pathways resulting in local or generalized tissue injury.
Acute Ischemic Injury
The occlusion of a major artery such as the middle cerebral artery is rarely complete and cerebral blood flow (CBF) depends on the degree of obstruction and the collateral circulation. The vascular compromise leading to an acute stroke is a dynamic process that evolves over time and is influenced by many factors.
These conditions influence the progression and the extent of ischemic injury:
1) Rate and duration: The brain better tolerates an ischemic event of short duration than a prolonged period of ischemia. However, the rate of development of ischemia also influences the extent of ischemic injury. A slow ischemic event allows for collateral circulation to be established.
2) Collateral circulation: The impact of ischemic injury is greatly influenced by the state of collateral circulation in the affected area of the brain.
3) Systemic circulation: Adequate systemic blood pressure is required to maintain cerebral perfusion.
4) Coagulation: Any hypercoagulable state increases the progression and extent of micro thrombi, exacerbating vascular occlusion.
5) Temperature: Elevated body temperature is associated with greater ischemic injury
6) Glucose: Both hyper or hypoglycemia have deleterious effects on progression of ischemic injury.
Pathophysiology at Macro tissue Level
The normal cerebral blood flow (CBF) is approximately 50 to 60 ml/100gm/minute and varies in different parts of the brain. In response to ischemia, the cerebral auto regulatory mechanisms compensate for a reduction in CBF by local vasodilatation, opening the collaterals and increasing the extraction of oxygen and glucose from the blood. However, when the CBF is reduced to below 20 ml/100gm/minute, an electrical silence ensues and synaptic activity is greatly diminished in an attempt to preserve energy stores. CBF of less than 10 ml/100gm/minute results in irreversible neuronal injury.
Microscopic Mechanisms of Neuronal Injury
Micro-thrombi form in distal vessels after an occlusion of a major artery such as the middle cerebral artery. These microvascular occlusions progressively increase with time.
Accumulation of noxious metabolites, such as lactic acid, glutamate, aspartate etc., originating from injured neurons increases with time, which results in injuring adjacent healthy neurons. A destructive cascade becomes established.
Cellular Mechanisms of Neuronal Injury: Excitotoxicity
At a cellular level, the development of hypoxic-ischemic neuronal injury is greatly influenced by “overreaction” of certain neurotransmitters, primarily glutamate and aspartate. This process called “excitotoxicity” is triggered by depletion of cellular energy stores. Glutamate, which is normally stored inside the synaptic terminals, is cleared from the extracellular space by an energy dependent process. The greatly increased concentration of glutamate in the extracellular space in a depleted energy state results in the opening of calcium channels. This causes calcium, sodium, and chloride ions to move into the cells and potassium to leak out. Intracellular calcium activates a series of destructive enzymes resulting in the loss of integrity of the cell membrane, triggering an inflammatory cascade and eventually cell death. Reperfusion of the infarct site and cellular infiltration may further exacerbate the inflammatory response.
Timing of Neuronal Death
The two processes by which the injured neurons are known to die are
A) Coagulation Necrosis and apoptosis.
Coagulation necrosis refers to a process in which individual cells die among living neighbor cells without eliciting an inflammatory response. (This is in contrast to liquefaction necrosis, which occurs when cells die, leaving behind a space filled by “inflammatory response” or pus.) This type of cell death is attributed to the effects of physical, chemical or osmotic damage to the plasma membrane. The cell initially swells then shrinks and undergoes pyknosis – a term used to describe marked nuclear chromatin condensation. This process evolves over 6 to 12 hours. By 24 hours, extensive chromatolysis occurs resulting in pan-necrosis. Astrocytes then swell and fragment. Myelin sheaths degenerate causing irreversible injury. The morphology of dying cells in coagulation necrosis is different than that of cell death due to apoptosis.
Apoptotic mechanisms begin within 1 hour after ischemic injury whereas necrosis begins later – by 6 hours after arterial occlusion. This observation has important bearing on future direction of research. The manner in which apoptosis evolves is a focus of much research, since hypothetically neuronal death can be prevented by modifying the process of DNA cleavage that seems to be responsible for apoptosis.
B) Major Categories of Ischemic Stroke
Ischemic strokes can be grouped into three main categories: (a) Thrombotic, (2) Embolic and (3) Global ischemic (Hypotensive) stroke. The list of “infrequent” causes is very long. However, strokes caused by vasospasm (migraine, following SAH, hypertensive encephalopathy) and some form of “arteritis” stand out among the more infrequent causes of stroke.
- Thrombotic Stroke
Atherosclerosis is the most common pathological feature of vascular obstruction resulting in thrombotic stroke. Other pathological etiologies of vascular occlusion in thrombotic stroke are: clot formation due to hypercoagulable state, fibromuscular dysplasia, arteritis (Giant cell and Takayasu), dissection of vessel wall and hemorrhage into a pre-existing plaque leading to an obstruction of the blood flow.
- Embolic Stroke
Most emboli lodge in the middle cerebral artery distribution because 80% of the blood carried by the large neck arteries end up in MCA. The two most common sources of emboli are the left- sided cardiac chambers and “artery to artery” emboli – as in detachment of a thrombus from the internal carotid artery at the site of an ulcerated plaque. Embolic strokes are generally smaller than thrombotic strokes.
Many embolic strokes become “hemorrhagic” because ischemic tissue is often reperfused when the embolus lyses spontaneously and blood flow is restored to a previously ischemic area.
- Global – Ischemic or Hypotensive Stroke
Profound reduction in systemic blood pressure for any reason is responsible for “hypotensive stroke.” Cerebral gray matter is particularly vulnerable. Global ischemia causes greatest damage to areas between the territories of the major cerebral and cerebellar arteries known as the boundary zone or watershed area. The parietal-temporal-occipital triangle at the junction of the anterior, middle and posterior cerebral arteries is most commonly affected. Watershed infarct in this area causes a clinical syndrome consisting of paralysis and sensory loss predominantly involving the arm. Face is not affected and speech is spared.
Complications of Restoration of Blood Supply to a Previously Ischemic Area
Two main complications of restoring blood supply are hemorrhage and cerebral edema. An initial vascular obstruction is likely to occur at a bifurcation of a major vessel. The occlusion may obstruct one or both of the branches, producing ischemia of the distal tissue. Blood vessels as well as brain tissue are rendered fragile and injured. When the occluding embolus either lyses spontaneously or breaks apart and migrates distally, CBF is restored to the “injured or ischemic” arterioles. This can result in a hemorrhagic or “red infarct” in what had previously been a bloodless field. The areas that continue to be poorly perfused are referred to as “Anemic Infarcts”.
The following factors are associated with “red infarcts” or a hemorrhagic transformation of stroke:
(a) Size of the infarct- The bigger the infarct, the greater the possibility of hemorrhage.
(b) Richness of collateral circulation.
(c) The use of anticoagulants and interventional therapy with thrombolytic agents is associated with a higher incidence of hemorrhagic transformation.
Vasogenic edema follows loss of cerebral autoregulatory mechanisms in ischemic areas of the brain. Large infarcts are associated with a greater potential of developing cerebral edema. Post ischemic brain edema peaks at 48 to 72 hours after the onset of symptoms.
• Common Homeopathic Remedies
1) Arnica Montana: Helps with trauma, shock, and weakness after stroke. It’s best for patients who feel sore, fatigued, and weak after the initial stroke event.
2) Causticum: Useful for paralysis, especially of facial muscles and limbs. It’s ideal for stroke patients with long-term paralysis or weakness of one side of the body.
3) Cicuta Verosa – Recommended for case of sudden onset, severe neurological condition including stroke. Muscular rigidity and spasm in limbs resembling post stroke spasticity.
4) Nux Vomica: Helps with muscle stiffness, spasms, and digestive troubles post-stroke. It’s best for stroke survivors with high stress levels, irregular lifestyle, and digestive complaints.
5) Gelsemium: Effective for extreme weakness, trembling, and fatigue. It’s suitable for patients with general weakness, shaky movements, and lack of confidence after a stroke.
6)Baryta Carbonica: Supports memory issues, confusion, and difficulties in elderly patients. It’s best for elderly stroke patients struggling with memory loss and slow recovery.
7) Belladonna: Helps with vascular problems, congestion, throbbing pain, and excitement. It’s useful for relieving complaints that worsen with touch, movement, and noise.
8) Hypericum Perforatum: Considered neuroprotective and helpful in injuries involving nerve damage. It relieves nerve pain, tingling, numbness, and sadness.
9) Stramonium: Deals with seizures and inflammation of the brain.
10)Ferrum: Valuable remedy for brain ischemia.
11)Phosphorus: Treats brain ischemia and congestion.
12)Zincum Metallicum: Recommended for chronic cases of ischemia
As they are selected based on individual symptoms and require personalized treatment. Homeopathy can be used alongside conventional medical treatment and physiotherapy to support stroke recovery
A Case Report
Preliminary Data
Name – Mr. K.D
Age – 68 yr
Sex – Male
Adders – Malgaon
Occupation – Farmar
Religion – Muslim
Marital status – Married
D.O.I – 10/07/2023
O.P.D. – 2533/23
Chief Complaints
Complete loss of movement and sensation of feet and hand left side since 3 – 4 days.
H/o Chief Complaints
- Complete loss of movement and sensation of feet and hand left side
- Complaints of loss of sensation of left feet ad hand with loss of motor function
- Involuntary urination
- Very offensive urination
- Irritable and talking nonsense all the time
- Restless day and night
Past History
No any major illness in past
Family History
No any major illness in family
Personal History
Apatite – Good
Desire – Non-veg
Aversion – Not specific
Thrust – Short quantity at short interval
Bowel – Satisfactory
Micturition – 4-5/0-1, D/N
Perspiration – scanty
Sleep/dreams – sound /no dreams
Mind –Irritable and talking nonsense things
- Restless day and night
- Not recognizing any buddy but answers well
General Physical Examination
Built – Average
Nourishment – Average
Conjunctiva – Pink
Nail – Pink
Tongue – Clean
Cyanosis – Absent
Oedema – Absent
Pallor – Absent
Vital Data
Temperature – 99.6’f
Pulse – 80 Beats/min
B.P – 140/90 mm of Hg
Resp Rate – 18 Cyc/min
Systemic Examination
CNS – All superficial reflux is decreased and deep reflux is normal
- Patient is conscious co-operative
- Talkative
- Weakness of the Left Upper Limb & Lower Limb.
GIT – NAD CVS – NAD RS – NAD
Differential Disease Diagnosis
Ischemic stroke
Hemorrhagic stroke
Tetanus
Investigation
CT SCAN BRAIN – Massive infract seen at right Cerebrum
CBC
ESR
Final Diagnosis
Ischemia of Left Cerebrum
Analysis of Symptom
Mental General – Irritable and talking nonsense things
- Restless day and night
- Not recognizing any buddy but answers well
Physical General – Convulsion
- Twitching and spasmodic jerks all over body
Particulars – Backward bending
- Abdomen is distended and painful due to Gas accumulation
Evaluation of symptoms
Grade I – Irritable and talking nonsense things
- Restless day and night
- Not recognizing any buddy but answers well
- Twitching and spasmodic jerks all over body
Grade II – Abdomen is distended and painful due to gas accumulation
- Backward bending
- Desire non-veg
Differential Remedial Diagnosis
Cicuta verosa
Cuprum met
Gelsemium
Opium
Final remedial diagnosis
Cicuta verosa
Indication
- Irritable and talking nonsense things
- Restless day and night
- Not recognizing any buddy but answers well
- Twitching and spasmodic jerks all over body
- Abdomen is distended and painful due to gas Accumulation
- Backward bending
Homoeopathic Treatment
Prescription
Name –Mr. K.D
Age – 68 yrs Sex – Male
Rx
Cicuta Verosa 30
Unit dose
PL
4-4-4 X 7 days
Follow up
| 17/07/2023 | Mentals better Recognizing touch Slight movement of foot | Rx, PL. 4-4-4 X 4 days |
| 24/07/2023 | Patient feels better Improved movement and senses | Rx Cicuta Verosa 30 Unit dose X 2 days |
CONCLUSION
Stroke is one of the leading causes of morbidity and mortality worldwide large difference in incidence and prevalence and mortality have been noted between different parts of world; this has been attributed to differences in risk factors with higher levels of hypertension and other risk factors resulting in more severe stroke.
Understanding of the pathogenesis of stroke is to understand how ischemia and hemorrhage cause injury. An ischemic stroke deprives neurons of oxygen and nourishment. Accumulation of noxious metabolites in the brain tissue originating from the injured or dying neurons increases with time, which then results in injury to the surrounding healthy neurons. This process can be halted or even reversed in the ischemic penumbral brain tissue if restoration of blood flow occurs within a critical time period. In hemorrhagic stroke, extra vascular release of blood causes damage by cutting off connecting pathways, resulting in local or generalized pressure injury.
Two major types of “strokes” cause brain damage: Ischemic and hemorrhagic stroke. In ischemic stroke, which represents about 80% of total strokes, lack of circulating blood deprives neurons of oxygen and nourishment. The effects are fairly rapid because the brain does not store glucose and is incapable of anaerobic metabolism. Hemorrhagic stroke causes damage to brain tissue by disrupting connecting pathways resulting in local or generalized tissue injury.
REFERENCES
1. Jones TH, Morawetz RB, Crowell RM, et al. Thresholds of focal ischemia in awake monkeys. J Neurosurgery. 1981; 54:773-782.
2. Wass CT, Lanier WL, Glucose modulation of ischemic brain injury: review and clinical recommendations. Mayo Clin Proc. 1996; 71:801-812.
3. Bruno A, Biller J, Adams HP Jr, et al. Acute blood glucose level and outcome from ischemic stroke. Neurology. 1999; 52:280-284.
4. Reith J, Jorgensen HS, Pedersen PM, et al. Body temperature in acute stroke: relation to stroke severity, infarct size, mortality, and outcome. Lancet. 1996; 347:422-425.
5. Schwab S, Spranger M, Aschoff A, et al. Brain temperature monitoring and modulation in patients with severe MCA infarction. Neurology. 1997; 48:762-767.
6. Pulsinelli WA. The ischemic penumbra in stroke. Sci Med. 1995; 1:16-25.
7. Hakim AM. Ischemic penumbra, the therapeutic window. Neurology. 1998;51(Suppl 3): S44-S46.
8. Astrup J, Seisjo BK, Symon L. Thresholds in cerebral ischemia – the ischemic penumbra. Stroke. 1981; 12:723-725.
9. Zivin JA, Choi DW. Stroke therapy. Sci Med. 1991; 265:56-53.
10. Wise RJ, Bernardi S, Frackowiak RS, Legg NJ, Jones T. Serial observations on the pathophysiology of acute stroke: the transition form ischemia to infarction as reflected in regional oxygen extraction. Brain. 1983;106 (Pt 1):197-222.
Co-Author- Mr. Padmraj Jineshwar Yaligouda, B.H.M.S. Final Year.
Bharatesh Homoeopathic Medical College & Hospital, Belagavi, Karnataka. India.