Background:
Obsessive–compulsive disorder (OCD) is a chronic psychiatric condition associated with significant functional impairment [1,2]. Evidence on the role of individualized homoeopathy in OCD is limited [9].
Objective:
To evaluate the clinical presentation of OCD and assess the effectiveness of individualized homoeopathic treatment using the Yale–Brown Obsessive Compulsive Scale (Y-BOCS) [3].
Methods:
A prospective observational clinical study was conducted on 30 diagnosed OCD patients attending the outpatient department of Dr. B.D. Jatti Homoeopathic Medical College and Hospital, Dharwad. Diagnosis was confirmed according to ICD-10 criteria [4]. Individualised homoeopathic remedies were prescribed based on totality of symptoms. Y-BOCS scores were recorded before and after treatment. Statistical analysis was performed using paired t-test.
Results:
Out of 30 cases, 24 patients showed significant clinical improvement, 2 showed no change, and 4 showed no improvement. Paired t-test revealed a statistically significant reduction in Y-BOCS scores (p < 0.05). Arsenicum album and Lycopodium were the most frequently prescribed remedies.
Conclusion:
Individualised homoeopathic treatment demonstrated significant improvement in OCD symptoms; however, larger controlled studies are required to confirm efficacy [10].
Keywords
Obsessive–Compulsive Disorder, Homoeopathy, Y-BOCS, Individualised Treatment, Clinical Study
Introduction
Obsessive–compulsive disorder (OCD) is a chronic and disabling neuropsychiatric disorder characterized by the presence of obsessions, compulsions, or both, resulting in significant distress and impairment in social, occupational, and personal functioning [1,2]. Obsessions are recurrent and persistent thoughts, urges, or images experienced as intrusive and
unwanted, while compulsions are repetitive behaviours or mental acts performed in response to these obsessions in an attempt to reduce anxiety or prevent feared consequences [7]. Common obsessions include contamination fears, pathological doubt, aggressive thoughts, and need for symmetry, whereas compulsions frequently involve excessive washing, checking, counting, arranging, or reassurance-seeking behaviours.
OCD affects individuals across all age groups and cultures, with an estimated lifetime prevalence of approximately 2–3% worldwide [2]. The disorder usually begins during adolescence or early adulthood and often follows a chronic fluctuating course if left untreated. In many patients, OCD is associated with considerable impairment in academic performance, occupational productivity, interpersonal relationships, and quality of life. Patients frequently experience social isolation, emotional distress, reduced self-esteem, and coexisting anxiety or depressive symptoms [5,8].
The exact etiopathogenesis of OCD remains multifactorial and incompletely understood. Neurobiological theories suggest dysfunction in cortico-striato-thalamo-cortical (CSTC) circuits along with abnormalities in serotonergic, dopaminergic, and glutamatergic neurotransmission [8]. Genetic predisposition, environmental stressors, personality traits, and psychological factors also contribute to disease development and progression. Conventional management of OCD primarily includes pharmacotherapy with selective serotonin reuptake inhibitors (SSRIs) and cognitive behavioural therapy (CBT), particularly exposure and response prevention therapy [5]. Although these treatments are evidence based and beneficial for many patients, a significant proportion of individuals continue to experience residual symptoms, medication-related adverse effects, relapse, or inadequate therapeutic response.
In recent years, complementary and integrative systems of medicine have gained increasing attention in mental health care, especially in chronic psychiatric conditions where individualized and holistic management approaches are sought [9]. Homoeopathy, based on the principle of individualization and totality of symptoms, aims to address both psychological and somatic dimensions of illness. Individualised homoeopathic prescribing considers mental generals, emotional characteristics, behavioural patterns, constitutional traits, and associated physical symptoms while selecting the appropriate remedy.
Despite the growing interest in complementary medicine, scientific evidence regarding the role of individualized homoeopathic treatment in OCD remains limited. Existing literature highlights the need for well-documented clinical studies using validated psychiatric assessment tools and standardized reporting methods [6,10]. The Yale–Brown Obsessive Compulsive Scale (Y-BOCS) is widely regarded as the gold standard instrument for assessing OCD severity and treatment response due to its reliability and validity [3].
The present observational clinical study was therefore undertaken to evaluate the clinical presentation and therapeutic outcomes of individualized homoeopathic treatment in patients diagnosed with OCD using the Y-BOCS scoring system. The study also aimed to
analyse the pattern of homoeopathic remedies prescribed in OCD patients attending a tertiary homoeopathic teaching hospital.
Aim and Objectives
Aim: To study the clinical presentation of OCD and evaluate the effectiveness of individualized homoeopathic treatment.
Objectives:
1. To assess baseline severity using Y-BOCS scale.
2. To evaluate clinical outcomes after treatment.
3. To analyse remedy distribution pattern in OCD.
Diagnosis was confirmed using ICD-10 diagnostic criteria [4].
Symptom severity was assessed using the Yale–Brown Obsessive Compulsive Scale (Y BOCS), a validated clinical rating instrument for OCD [3].
The study was conducted and reported in accordance with REHBaR guidelines for homoeopathic research reporting [6].
Materials and Methods
Study Design: Prospective observational clinical study.
Study Setting: Dr. B.D. Jatti Homoeopathic Medical College and Hospital, Dharwad. Sample Size: 30 OCD patients.
Sampling Method: Purposive sampling.
Diagnostic Criteria: ICD-10 criteria [4].
Symptom severity was assessed using the Yale–Brown Obsessive Compulsive Scale (Y BOCS), a validated clinical rating instrument for OCD [3].
The study was conducted and reported in accordance with REHBaR guidelines for homoeopathic research reporting [6].
Inclusion Criteria: Diagnosed OCD patients of both genders and all age groups with informed consent.
Exclusion Criteria: Other psychiatric disorders and those on conventional treatment. Intervention: Individualised homoeopathic prescriptions based on symptom totality. Outcome Measure: Y-BOCS score.
Follow-up: Weekly, fortnightly, and monthly.
Statistical Analysis: Paired t-test, p < 0.05 considered significant.
Ethical Consideration: Written informed consent obtained.
Results
Out of 30 patients, 17 were males and 13 females. Majority belonged to 21–30 years age group. Twenty-four patients improved, two had no change, and four showed no improvement. Paired t-
test showed significant reduction in Y-BOCS score (t = −5.84, p = 0.00001). Arsenicum album and Lycopodium were most frequently prescribed remedies.
Statistical Analysis
Data were analysed using Statistical Package for Social Sciences (SPSS) version 25.0. Descriptive statistics were used to calculate mean and standard deviation. Paired t-test was applied to compare baseline and post-treatment Y-BOCS scores. The level of statistical significance was set at p < 0.05.
Discussion
Obsessive–compulsive disorder is considered one of the leading causes of psychiatric disability worldwide because of its chronic course, high relapse tendency, and impact on quality of life [1,2]. The disorder affects emotional wellbeing, interpersonal relationships, occupational functioning, and social participation. Many patients experience persistent anxiety and distress due to repetitive intrusive thoughts and compulsive rituals, which consume significant time and interfere with routine activities.
The present observational study evaluated the effectiveness of individualized homoeopathic treatment in OCD patients using the Yale–Brown Obsessive Compulsive Scale (Y-BOCS), which is considered a reliable and validated instrument for measuring symptom severity and treatment response [3]. The findings demonstrated statistically significant reduction in mean Y-BOCS scores following treatment, suggesting improvement in obsessive and compulsive symptoms among the majority of patients included in the study.
In the present study, the majority of patients belonged to the 21–30 years age group, which is consistent with previous epidemiological studies reporting that OCD commonly manifests during adolescence and early adulthood [2,8]. Male predominance observed in this study may reflect healthcare-seeking patterns or sociocultural factors influencing psychiatric consultation in the study population.
Individualised homoeopathic treatment was prescribed based on the totality of symptoms, considering mental, emotional, and physical characteristics unique to each patient. Remedies such as Arsenicum album and Lycopodium were frequently prescribed due to the predominance of symptoms like anxiety, fear, insecurity, perfectionism, anticipatory anxiety, excessive concern regarding cleanliness, and compulsive behaviours. The individualized approach of homoeopathy emphasizes patient-specific symptom expression rather than disease-label-based prescribing.
The statistically significant reduction in post-treatment Y-BOCS scores indicates possible therapeutic benefit associated with individualized homoeopathic intervention. Similar observations have been reported in integrative and complementary medicine research, where individualized approaches were associated with improvement in psychological wellbeing and
symptom burden [9]. However, it must be emphasized that the observational design of the study does not establish causality.
The findings should also be interpreted in the context of certain methodological limitations. The absence of a control group limits comparison with placebo effects or natural symptom fluctuations. The sample size was relatively small, reducing generalizability of results. In addition, observer bias and patient expectation bias cannot be completely excluded. The duration of follow-up was limited, making long-term assessment of relapse prevention difficult.
Nevertheless, the study has several strengths. Standardized diagnostic criteria (ICD-10) and a validated psychiatric assessment scale (Y-BOCS) were used for evaluating clinical outcomes. The study also contributes preliminary clinical evidence regarding homoeopathic management of OCD in an Indian tertiary care setting, an area where published observational data remain limited.
Limitations
1. Small sample size.
2. No control group.
3. Short follow-up period.
4. Observer biases possible.
Conclusion
The study findings indicate that individualized homoeopathic treatment may have a supportive role in reducing symptom severity among patients with obsessive–compulsive disorder when assessed using the Y-BOCS scale. Although encouraging clinical improvement was observed in a majority of cases, further rigorous scientific investigations with robust methodology are essential before definitive conclusions regarding efficacy can be established.
Novelty Statement
This study provides preliminary evidence on homoeopathic management of OCD using an objective psychiatric rating scale (Y-BOCS) in an Indian clinical setting.
Declarations
Funding: None.
Conflict of Interest: None declared.
Ethical Approval: The study protocol was reviewed and approved by the Institutional Ethics Committee (IEC) of Dr. B. D. Jatti Homoeopathic Medical College & Hospital, Dharwad. Written informed consent was obtained from all participants.
Acknowledgment
The author sincerely acknowledges Dr. B. D. Jatti Homoeopathic Medical College & Hospital and PG Research Centre, Dharwad, for providing necessary facilities to conduct this study. The author also expresses gratitude to the guide, Dr. Monika S Katti, for her valuable support and guidance throughout the course of the study.
Table 1. Clinical Outcome Based on Y-BOCS Score
| Outcome | Number of Cases | Percentage |
| Improved | 24 | 80% |
| No Change | 2 | 6.7% |
| Not Improved | 4 | 13.3% |
Table 2. Distribution of Homoeopathic Remedies Prescribed
| Remedy | Number of Cases |
| Arsenicum album | 6 |
| Lycopodium | 5 |
| Sulphur | 3 |
| Silicea | 3 |
| Staphysagria | 2 |
Figures
Figure 1. Bar graph showing clinical outcome based on Y-BOCS score after homoeopathic treatment.
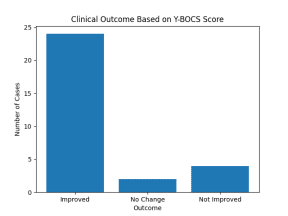
Figure 2. Bar graph showing distribution of frequently prescribed homoeopathic remedies in OCD patients.
Table 3. Pre- and Post-Treatment Y-BOCS Scores (Mean ± SD)
| Assessment | Mean Y-BOCS Score | Standard Deviation (SD) |
| Baseline | 24.6 | 6.2 |
| Post-Treatment | 12.3 | 5.1 |
REFERENCES
1. Reddy YJ, Rao NP, Khanna S. An overview of Indian research in obsessive compulsive disorder. Indian J Psychiatry. 2010;52:200–204.
2. Fineberg NA, et al. Obsessive-compulsive disorder. Lancet Psychiatry. 2019;6(8):720–736.
3. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: Development, use, and reliability. Arch Gen Psychiatry. 1989;46(11):1006–1011.
4. World Health Organization. ICD-10 Classification of Mental and Behavioural Disorders. Geneva: WHO; 2007.
5. Veale D, Roberts A. Obsessive-compulsive disorder. BMJ. 2014;348:g2183. 6. Mathie RT, et al. Reporting research in homeopathy: REHBaR guidelines. Homeopathy. 2015;104(4):238–246.
7. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 5th ed. Washington DC: APA; 2013.
8. Stein DJ, et al. Obsessive–compulsive disorder. Nat Rev Dis Primers. 2019;5:52. 9. Witt CM, et al. The role of complementary and integrative medicine in mental health. J Affect Disord. 2015;175:72–81.
10. Mathie RT, et al. Randomised placebo-controlled trials of individualised homeopathy: systematic review. Systematic Reviews. 2014;3:142.