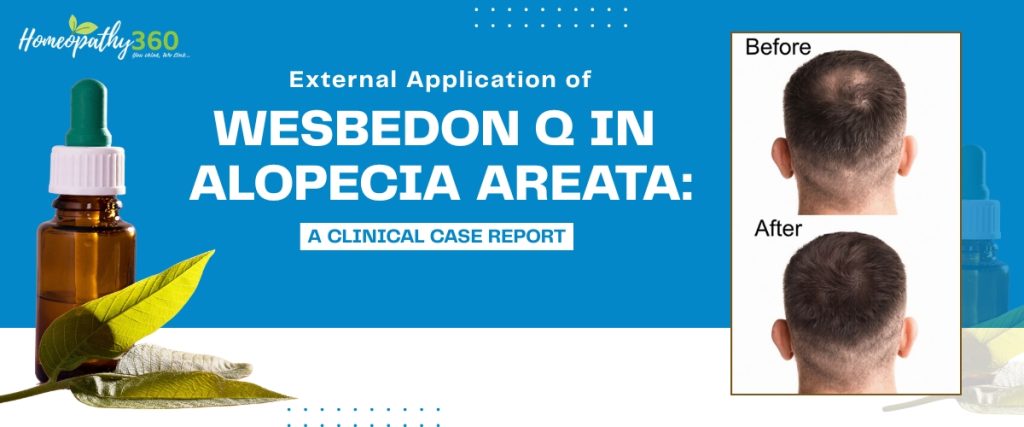
Abstract
Alopecia areata is a non-scarring autoimmune disorder characterized by sudden patchy hair loss. Conventional management includes corticosteroids and immunotherapy; however, recurrence and side effects remain concerns. This case report describes a 28-year-old male with localized alopecia areata managed exclusively with external application of Wesbedon mother tincture (Q). Significant hair regrowth was observed within four months without internal medication. This case suggests a possible role of topical homoeopathic mother tincture in localized alopecia areata and warrants further clinical investigation.
Keywords
Alopecia areata, Wesbedon Q, Mother tincture, Homoeopathy, Hair regrowth, Case report
Introduction
Alopecia areata (AA) is an autoimmune disorder characterized by T-cell mediated attack on hair follicles, leading to non-scarring hair loss. The lifetime risk is approximately 1–2% worldwide. It commonly presents as well-defined, round bald patches over the scalp.
Current conventional treatments include:
∙ Topical or intralesional corticosteroids
∙ Topical immunotherapy
∙ Minoxidil
Despite these therapies, relapse rates are high.
Homoeopathy approaches disease holistically, typically using internal constitutional remedies. However, certain mother tinctures are known to act locally on tissues. Literature regarding exclusive external use in alopecia areata remains limited. According to Organon (Aphorism 186–187), local diseases represent internal disturbance. However, in recent, localized conditions without systemic involvement, cautious local application that is non-suppressive may aid recovery. In this case, Wesbedon Q was used externally without suppressive intent and resulted in progressive hair regrowth.
Patient Information
∙ Age: 28 years
∙ Gender: Male
∙ Occupation: Labour worker in dyeing and printing mill
∙ Residence: Heavy industrial pollution area
∙ Socioeconomic Status: Middle class
Chief Complaint
Sudden onset of a localized bald patch over the scalp for 1 month. Hair falling particular occipital area of head.
History of Present Illness
∙ The patient developed a round, well-demarcated bald patch 1 month prior to consultation.
∙ The lesion: Appeared suddenly
∙ Gradually increased in visibility
∙ No itching
∙ No scaling
∙ No discharge
∙ No redness
∙ No pain
∙ No previous similar episodes
Past History
∙ No major illness
∙ No autoimmune disease
∙ No chronic skin disorders
Family History
∙ Parents alive and healthy
∙ No family history of alopecia or autoimmune disorder
Personal History
∙ Appetite: Normal
∙ Thirst: Normal
∙ Sleep: Normal
∙ Bowel & bladder: Regular
Mental Generals
∙ Suspicious nature
∙ Anger when work is not done according to his expectations
∙ Otherwise polite
Clinical Examination
∙ Single well-defined circular bald patch
∙ Smooth surface
∙ Non-scarring
∙ No inflammation
∙ No scaling
Case Analysis
∙ Acute onset
∙ Localized pathology
∙ Occupational exposure to chemicals
∙ Absence of systemicFeb 1 2025 involvement
Prescription
∙ Medicine: Wesbedon Q
∙ Potency: Mother tincture
∙ Mode: External application only
∙ Method: Applied locally over affected area with cotton
∙ Frequency: Twice daily
Follow-Up Timeline
| Date | Follow up |
| Jan 15 2025 | Clear bald patch, no regrowth |
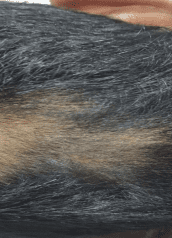
| Feb 1 2025 | Fine vellus hair growth visible |
| Feb 18 2025 | Progressive thickening of hair |
| Mar 5 2025 | Significant hair regrowth |
Outcome
Marked improvement with visible hair regrowth over the affected area after 4 months of exclusive topical therapy.
Discussion
Alopecia areata is considered an autoimmune condition mediated by CD8+ T lymphocytes targeting hair follicles. Environmental triggers, including occupational chemical exposure, may play a contributory role.
In this case:
∙ The patient was exposed to industrial pollutants.
∙ No systemic autoimmune association was found.
∙ Local stimulation via mother tincture application appeared to promote follicular recovery.
Dr. Hahnemann emphasized that local diseases are manifestations of internal dynamic disturbance (Aphorism 186–187). He cautioned against suppressive external treatments that merely remove symptoms without curing the internal cause (Aphorism 196). However, he acknowledged that local applications may assist cure when used judiciously and without suppressive intent (Aphorism 194). In the present case, the pathology was recent and localized, with no systemic involvement. The external use of Wesbedon Q was employed as a non suppressive local stimulus, and progressive improvement was observed.
Conclusion
This case demonstrates significant hair regrowth in localized alopecia areata following exclusive external application of Wesbedon Q. While promising, further controlled studies are required to validate its therapeutic role.
Treatment Image

REFERENCES
1. Pratt CH, King LE Jr, Messenger AG, Christiano AM, Sundberg JP. Alopecia areata. Nat Rev Dis Primers. 2017;3:17011.
2. Gilhar A, Etzioni A, Paus R. Alopecia areata. N Engl J Med. 2012;366(16):1515–25.
3. Messenger AG, McKillop J, Farrant P, McDonagh AJ, Sladden M. British Association of Dermatologists’ guidelines for alopecia areata. Br J Dermatol. 2012;166(5):916–26.
4. Hahnemann S. Organon of Medicine. 6th ed. Translated by Boericke W. New Delhi: B Jain Publishers; 2002.
5. Boericke W. Pocket Manual of Homoeopathic Materia Medica. New Delhi: B Jain Publishers; 2010.
6. Allen HC. Keynotes and Characteristics with Comparisons. New Delhi: B Jain Publishers; 2002.