Abstract
Enuresis is a common pediatric condition that can significantly impact a child’s psychological well-being and quality of life . The prevalence in India is 7.61%–16.3%. The prevalence is highest in children aged 5–8 years and lowest in children aged 11–12 years. The worldwide prevalence of enuresis among children aged 6–12 years is 1.4%–28%. In general, prevalence of nocturnal enuresis is higher among male children than female children. This case report presents successful management of nocturnal enuresis using individualized homeopathic treatment with Lycopodium.
Keywords : Bed wetting , incontinence , homeopathy
Introduction
The International Children’s Continence Society (ICCS) defines intermittent incontinence as urine leakage in discrete amounts, occurring during the day and/or at night in children aged ≥5 years. Primary enuresis is -enuresis in a child who has never established continence for over 6 months , is the more common form occurring in 80% of cases. It is nocturnal wetting in a child who has never been dry on consecutive nights for longer than 6 months. Secondary enuresis is the reemergence of enuresis after continence has been established for at least 6 months. Nocturnal enuresis can cause a feeling of failure and result in chronic stress. It impacts the emotional state, self-esteem, as well as the social development of a child. Children may feel unable to participate in activities and may feel that they are missing out on important aspects of their life.[5,6] Children with nocturnal enuresis have lower self-esteem, mental health, skills, and poorer relation to their parents and others.
The etiology of nocturnal enuresis is multifactorial, involving delayed maturation of bladder function, reduced nocturnal secretion of antidiuretic hormone, increased nighttime urine production, reduced functional bladder capacity, deep sleep patterns, and psychological stressors. Genetic factors also play a significant role, with higher incidence observed in children with a positive family history.
Case presentation
Chief complain
A 8 years old male boy , 3rd std. A student came with a complaint of involuntary urination at mid-night around 1 PM for 2 yrs, 4-5 episodes in a week . There was no history of daytime incontinence.
Agg. –Mid night ,around 1 PM
Past history
Getting cold easily in childhood
Family history
Father : Hemorrhoids and constipation
Physical general
Appetite : Intolerable , hurried while eating , even eat after stomach full
Thirst : 4- 5 glass/ day
Desire : sweets like chocolates , ice cream , Gulab jamun
Aversion : Brinjal
Urine : 5-6 Time / day , occasionally 1 time/night
Stool : 1 Motion /day
Sleep : Disturb
Dreams : Not remember
Perspiration : profuse on face and head after playing
Thermal : Chilly
Mental general :
His father and mother told me about his complaint. His mother said that he is very obstinate and annoying at home and always fights with sister. He dominates the whole house and wants things his way, when things aren’t exactly as he wants he becomes very angry. He is totally opposite at home and very different here. He can not stay alone , always wants someone. Fear of darkness, ghosts, being alone.
In the initial case he avoided eye contact. During conversation he kept silent, looking very innocent, smiley, calm and timid. He speaks softly and looks at parent before answering.
Physical examination
Built – lean, thin body, brownish complexion
Height – 132 cm
Weight – 23 kg
No sign of pallor, cyanosis, clubbing, jaundice, edema, lymphadenopathy
Systemic examination
Respiratory system: BLAE clear
Cardiovascular system: S1, S2 heard, no murmur
GIT: Bowel sounds heard, per abdomen soft and non tender
Central nervous system: Conscious and oriented with time, place and person.
Totality of symptoms
Obstinate
Fear of being alone
Fear of darkness
Desire for sweets
Intolerable hunger even eat after full stomach
Involuntary urination at night time
Repertorization
Repertorization was carried out using Synthesis.
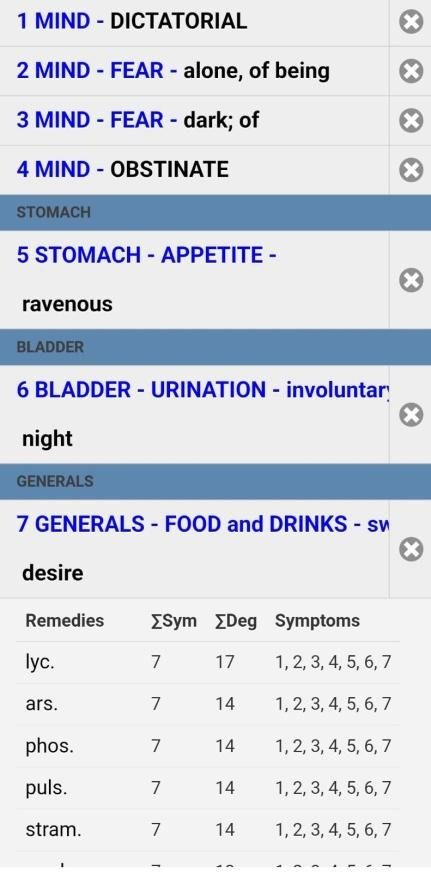
Selection of final remedy with justification
Lycopodium was selected as a most appropriate based on:
Strong correspondence with mental generals , desire for sweet and urinary complain . 4 dose of lycopodium 200 was prescribed followed by placebo twice daily for 15 days in accordance with homeopathic principle of minimum dose and individualized prescription.
Prescription
Lycopodium 200C – BD for 2 days, followed by placebo for 15 days.
Auxiliary management : avoid drinking water 1 hour before going to sleep and empty bladder before going to bed .
Follow up and results
| Follow up | Duration | Complain | prescription |
| Baseline | Day 0 | 4-5 times/week | Lyco 200 BD for 2 days |
| 1st Follow up | 15 days | Reduced to 2-3 times / week | Sac lac BD |
| 2ndFollow up | 1 months | 1-2 episode in last 15 days | Sac lac BD |
| 3rd Follow up | 1 months | 1 episode in last 1 month | Lyco 200 1 dose |
| 4th Follow up | 2 months | No episode | Sac lac |
Conclusion
This case highlights the management of nocturnal enuresis in an 8 year old child using individualized homeopathic medicine lycopodium . The patient showed significant improvement in the frequency of bedwetting episodes along with overall enhancement in confidence and emotional wellbeing during the course of treatment . Through detailed case taking and reportorial analysis , lycopodium was selected based on prominent mental characteristics such as bossy at home & timid outside , fearful & lack of confidence but intellectually capable and obstinate , along with physical symptoms like urinary symptoms . The observed clinical improvement suggests a possible therapeutic role of individualized homeopathic treatment in pediatric nocturnal enuresis .
References
1. Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM. Nelson Textbook of Pediatrics. 21st ed. Philadelphia: Elsevier.
2. Reddy NM, Malve H, Nerli R, Venkatesh P, Agarwal I, Rege V. Nocturnal enuresis in india: Are we diagnosing and managing correctly. Indian journal of nephrology. 2017 Nov;27(6):417. accessed on 20-2-2020, available from https://pmc.ncbi.nlm.nih.gov/articles/PMC5704404/
3. Hahnemann S. Organon of Medicine. 6th ed. New Delhi: B Jain Publishers; 2002.
4. Kent JT. Lectures on Homoeopathic Philosophy. New Delhi: B Jain Publishers
5. Boericke W. Pocket manual of homoeopathic materia medica and repertory. Reprint ed. New Delhi: B Jain Publishers.