Abstract
Osteoarthritis of the knee, also known as degenerative joint disease, is typically the result of wear and tear and progressive loss of articular cartilage and is a major cause of pain and disability in older people. It is characterised by focal loss of articular cartilage, subchondral osteosclerosis, osteophyte formation at the joint margin, and remodelling of joint contour with enlargement of affected joints. While conventional medicine explains it mainly through mechanical and age related degeneration, Homoeopathy views knee osteoarthritis as an expression of chronic miasmatic dyscrasia. This article correlates pathological changes in knee osteoarthritis with Hahnemannian miasmatic evolution. Early functional disturbances correspond to Psora, proliferative changes such as synovial thickening and osteophyte formation reflect Sycosis and advanced degeneration with deformity indicates Syphilitic predominance. Understanding this miasmatic-pathological relationship supports a holistic, individualized homoeopathic approach aimed at controlling symptoms and slowing disease progression.
Key Words: Knee osteoarthritis, Pathology, Miasmatic evolution, Psora, Sycosis, Syphilis, Homoeopathy
Introduction
In today’s scenario, osteoarthritis of knees is becoming a common rheumatological problem in India. Its high prevalence, especially in the elderly and its negative impact on physical function make it a leading cause of disability. But nowadays, even in adults between the ages of 40 to 55 years with joint complaints also increasing. So in many cases this affects the personal life of peoples at physical as well as mental level and it creates problems in doing day to day activities.
Osteoarthritis is the second most common rheumatological problem and it is the most frequent joint disease with a prevalence of 22% to 39% in India. More common in women than men, but the prevalence increases dramatically with age. Nearly, 45% of women over the age of 65 years have symptoms while radiological evidence is found in 70% of those over 65 years. Osteoarthritis of the knee is a major cause of mobility impairment, particularly among females. Osteoarthritis was estimated to be the 10th leading cause of nonfatal burden.
This condition is caused by the reasons as mentioned above along with other causes like heredity, repetitive injuries (from sports or accidents), obesity, metabolic diseases like diabetes mellitus, joint deformities like being born with malformed joints or defective cartilages, etc.
In such circumstances, homeopathy can help the patient by improving their symptoms like reducing pain and swelling, by improving motility of affected joints and by improving quality of their life and improving patient’s general feeling of well-being. It is the most Morden system of treatment and the fact is that homeopathic medicines are gentle to treat, safe and cost effective for all socio-economic classes.
Chronic diseases, as described by Samuel Hahnemann, originate from dynamic disturbances in the vital force caused by inherited or acquired miasmatic influences. Hence, knee osteoarthritis is not an only joint pathology but an expression of miasmatic evolution reflected through structural and functional pathological changes. This miasm is inherited in our body, when these chronic diseases are treated with homeopathic medicine it acts on vital force and increases the immunity of patients and decreases the chance of disease going into deeper levels and helps to reduce complications. These homeopathic medicines should not only be selected on the basis of symptoms similarity or disease similarity but miasm are also to be considered. Understanding knee osteoarthritis through pathology and miasmatic evolution allows the homoeopathic physician to treat the patient constitutionally rather than symptomatically.
Etiology And Risk Factor
Knee osteoarthritis is classified as either primary or secondary, depending on its cause. Primary knee osteoarthritis is the result of articular cartilage degeneration without any known reason. This is typically thought of as degeneration due to age as well as wear and tear. Secondary knee osteoarthritis is the result of articular cartilage degeneration due to a known reason.
Cause Of Secondary Osteoarthritis:
- Acute or chronic joint trauma
- Congenital and developmental causes, such as differences in the length of lower extremities, Varus or Valgus deformity of lower extremities, joint hypermobility syndrome, dysplasia of joints, dysplasia of bones.
- Metabolic disorders such as rickets, Alkaptonuria (ochronosis), hemochromatosis, or Wilson disease
- Endocrine disorders: Acromegaly, thyrotoxicosis, diabetes mellitus, obesity, hypothyroidism.
- Diseases caused by deposition of calcium salts: Chondrocalcinosis,
- Inflammatory arthritis: Rheumatoid arthritis, psoriatic arthritis/peripheral spondyloarthritis, gout, and other types of inflammatory arthritis.
- Other bone and joint conditions: Fractures, infections, Paget disease, osteoporosis, osteochondritis dissecans
- Neuropathic osteoarthropathy: Charcot joints
Risk Factors Of Osteoarthritis
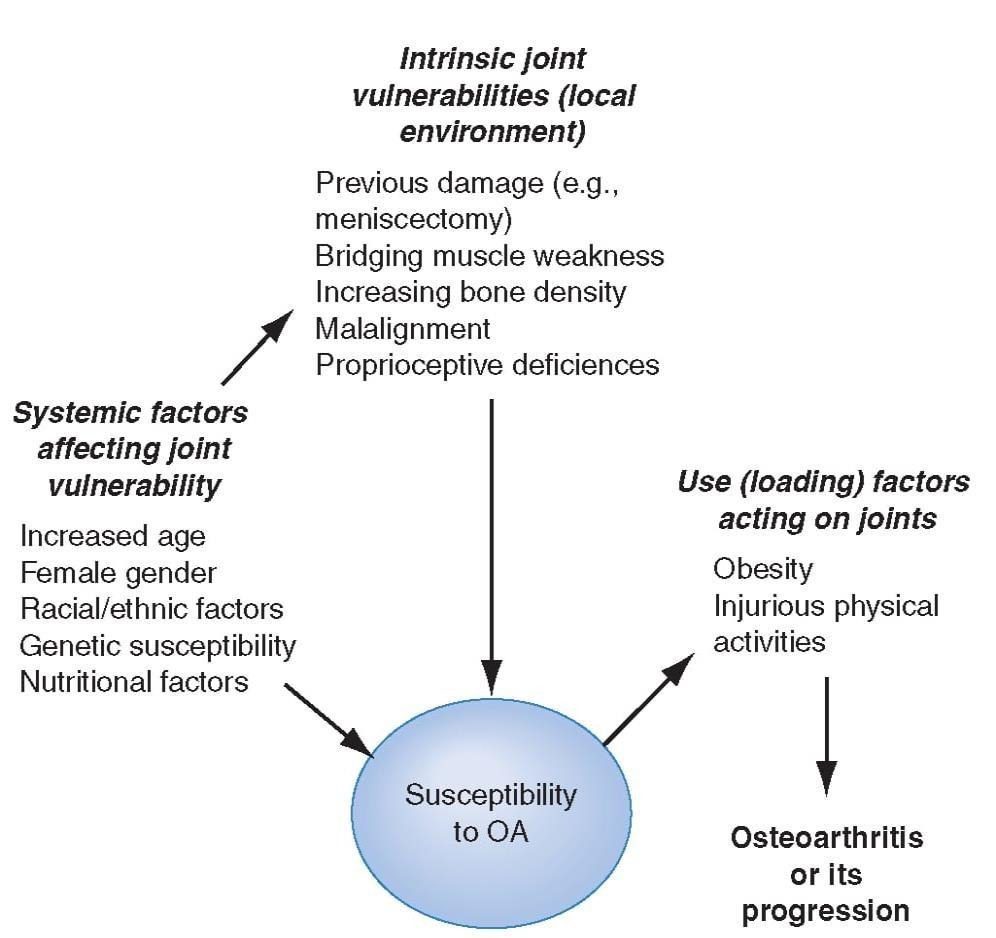
Figure– Risk factors for osteoarthritis (OA) either contribute to the susceptibility of the joint (systemic factors or factors in the local joint environment) or increase risk by the load they put on the joint. Usually a combination of loading and susceptibility factors is required to cause disease or its progression.
Pathophysiology
Articular cartilage is composed primarily of type II collagen, proteoglycans, chondrocytes, and water. Healthy articular cartilage constantly maintains an equilibrium between each of the components so that any degradation of cartilage is matched by synthesis. Healthy articular cartilage is thus maintained. In the process of osteoarthritis, matrix metalloproteases (MMPs), or degradative enzymes, are overexpressed, disrupting the equilibrium and resulting in an overall loss of collagen and proteoglycans. In the early stages of osteoarthritis, chondrocytes secrete tissue inhibitors of MMPs (TIMPs) and attempt to increase the synthesis of proteoglycans to match the degradative process. However, this reparative process is not enough. The loss in equilibrium results in a decreased amount of proteoglycans despite increased synthesis, increased water content, the disorganized pattern of collagen, and ultimately loss of articular cartilage elasticity. Macroscopically these changes result in cracking and fissuring of the cartilage and ultimately erosion of the articular surface.
Although knee osteoarthritis is closely correlated with aging, it is important to note that knee osteoarthritis is not simply a consequence of aging but rather its own disease. This is supported by the differences seen in cartilage with both osteoarthritis and aging. Furthermore, the enzymes responsible for cartilage degradation are expressed in higher amounts in knee osteoarthritis, whereas they are at normal levels in the normal aging cartilage.
Clinical Features
Clinical manifestations usually occur after the age of 45 years and are highly variable in severity. They do not always correlate with the degree of joint damage seen on imaging studies.
Sign And Symptoms
- Joint pain is the dominant symptom. Pain is located in the joint and the upper part of the lower leg and is usually worse with weight-bearing and ambulation. In advanced OA, it may be severe and also occur at rest and at night. Pain can be worse during initial movements following a period of immobility and gradually improve with subsequent movements but then intensify with further use. Pain is usually relieved by rest. Associated peri-articular soft-tissue involvement (e.g. bursitis) can cause pain away from the joint line, whereas pain originating from the joint itself is usually maximal at the joint line.
- Flexion and extension of the joint may produce palpable crepitus. The axis of the limb is almost always abnormal, with Varus deformity being more common than valgus deformity. Joint effusion and popliteal cyst (Baker cyst) are frequently seen. Joint outlines may be widened and deformed in advanced cases. Secondary changes include weakness and atrophy of the quadriceps muscles, enthesitis of the lateral collateral ligaments and knee flexors insertions, and pes anserine bursitis; these also cause pain. In patients with advanced OA of the knee, a flexion contracture of the knee can occur.
- OA can affect any or all compartments of the knee: medial (most common, may be accompanied by Varus knee deformity), lateral (less common, may be accompanied by valgus knee deformity), and patellofemoral. Patients with patellofemoral OA may have more pain going downstairs than upstairs.
- Other features include transient stiffness lasting <30 minutes (early morning or after inactivity), absence of warmth and occasionally joint effusion.
Diagnosis And Investigations
It is not difficult. Clinical features and X-rays confirm the diagnosis.
Laboratory Investigations
- Blood test: No blood tests are routinely indicated for workup of patients with OA. It is usually done to rule out other diseases or comorbidities.
- Imaging: The diagnosis of OA does not routinely require plain radiographs, which are often normal in early stages and also may not correlate with severity of symptoms till late in the disease.
- X ray of involved joint may show a following characteristic features:
- Narrowing of the joint space (due to loss of articular cartilage)
- Sclerosis of the subchondral bony plate
- Subchondral cysts caused by bone destruction
- Osteophytes at the joint margins (the bony excrescence or outgrowth, usually branched in shape)
- Deformities.
- Other imaging studies (computed tomography [CT], magnetic resonance imaging [MRI], Ultrasonography, Scintigraphy) may be useful in differentiating OA from other joint and bone disorders but are often not reveal very early lesions, which precede clinical and radiographic manifestations.
Homoeopathic Perspective
According to the Hahnemannian classification of diseases, Osteoarthritis of knees falls under the category of fully developed chronic miasmatic disease. As per § 5 for the development of any chronic disease, there is always some underlying cause responsible for it and these causes are fundamental. i.e., all the three miasms psora, sycosis and syphilis. Hereditary weakness, suppressed acute disease, prolonged drugging, emotional stress, and faulty lifestyle or many other factors disturb the vital force, allowing miasms to manifest through chronic degenerative pathology. On the basis of its pathology and progression of disease osteoarthritis of knees falls under sycotic miasm, though underlying or fundamental miasm can be psora, sycosis or syphilis.
As per aphorisms 204 to 206 in Organon of Medicine, Dr Hahnemann describes that all chronic affections and diseases properly so-called must be cured only from within, by the homoeopathic medicines appropriate for the miasm that lies at their root and Preliminary investigate that miasm which is lies at their root, it can be the simple miasm or is complications with a second or even with a third.
Pathological Consideration And Miasm
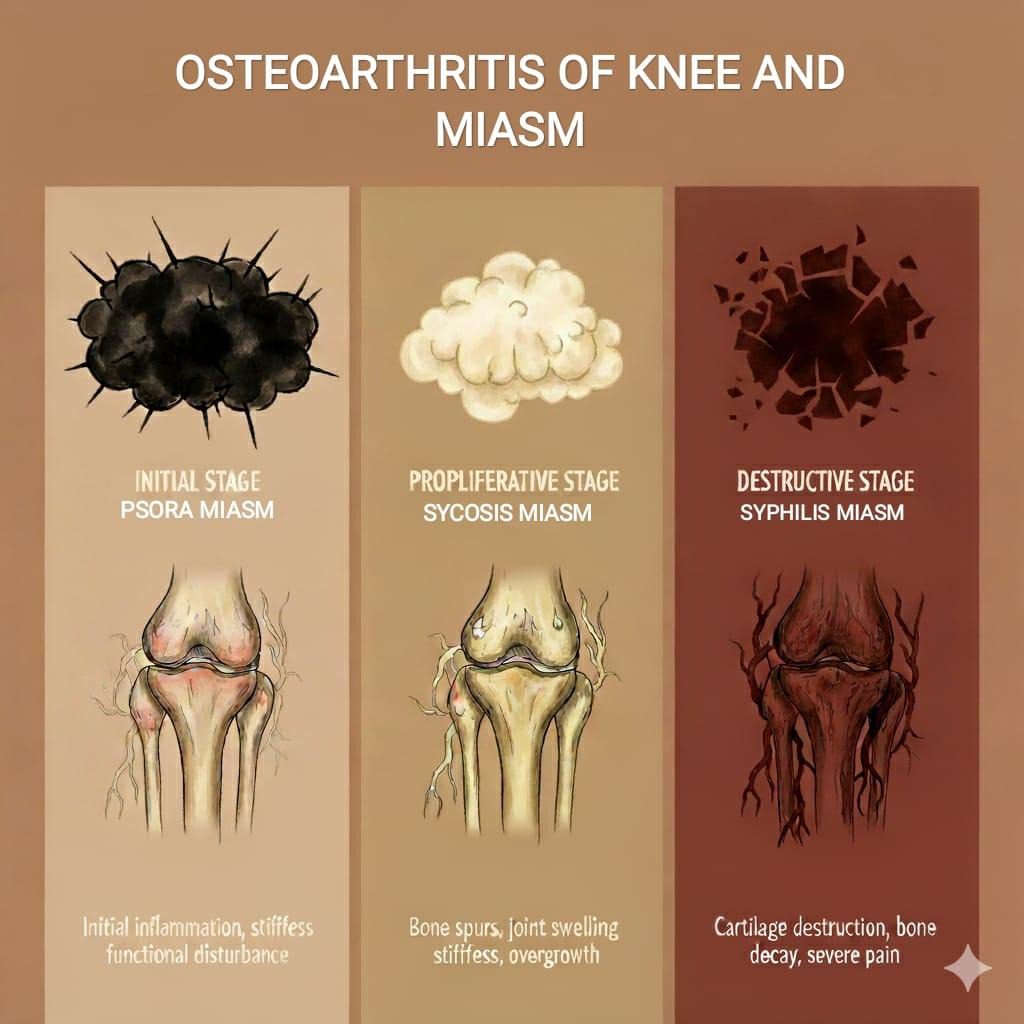
Pathological changes of OA are one of the important aspects in understanding the miasmatic background of disease. Osteoarthritis knee develops slowly over time due to wear and tear of joints, inflammation and the body fails to attempt to repair itself. It appears step by step.
In firstly, cartilage tries to adapt or compensate the stage. In early stages, due to increased stress (due to aging, obesity or injury) or minor damage, for the protection of the joints body tries to thicken the cartilage. In this stage synovial membranes produce more fluid which causes swelling. This early stage is sycotic phase, where the body tries to overgrow or compensate.
If the stress continues, the cartilage loses its ability to regenerate properly. After that Knee joint struggles to maintain balance and starts experiencing occasional pain especially after exertion. This mid stage is the psoric phase.
Here, cartilage loses its ability to repair itself so that the thickened cartilage becomes more- weak, loses its elasticity and starts to break down. Enzymes from inflammatory cells damage collagen and proteoglycans, which reduces cartilage strength. The joint becomes stiff. A small crack or bone spurs and soft spots appear to stabilize the joint but worsen the stiffness and the smooth surface of the cartilage becomes rough which leads to friction between bones.
As cartilage completely wears away, the space between bones becomes narrow. So that bones start rubbing against each other which causes pain and stiffness. The synovial membrane which produces joint fluid for lubrication, becomes inflamed. So that quality and amount of synovial fluid decrease, which leads to less lubrication and more friction. Inflammation releases harmful enzymes that further damage cartilage completely, over time muscle around the knee becomes weak, which makes the joint less stable. The knee undergoes severe destruction, loses its normal shape and becomes misaligned, which lead to bowing or knock-knees and joints becoming deformed. This late stage is the syphilitic phase.
Clinical Presentation And Miasm
Some differentiating points for the comparison of miasms in Osteoarthritis knee are as follows:
| PSORA | SYCOSIS | SYPHILIS | |
| Character | Various type of rheumatism, especially when functional and inflammatory in nature without gross structural changes, twitching of the muscles during sleep, the patient can walk well and finds it difficult to stand still. | Chronic or long-continued inflammations especially in the joints. Easy spraining of the joints while walking; joints and connective tissues which are easily affected. stiffness, soreness and lameness are characteristic of sycosis. osteoarthritis in general sycotic. swelling of joint, tophi and deposits in the joints. Osteophytes formation. slightest physical exertion fatigues the sycotic patient. Proliferative variety of inflammation or growth. | Aching pains in bones and in the joints. Joint is weak and patient is stumbles and fall easily. various deformities(Arthritic deformities) and atrophy or emaciation. |
| Sensations | Neuralgic type of pains. numbness with tingling sensations which occurs when pressure is brought to bear on part, when lying lightly on the part or when sitting cross-legged. | Joints pain Stitching, Pulsating, Shooting, Tearing, and Wandering. Shooting and tearing pain may occur in the muscles as well as the joints. Stiffness, Soreness, Lameness. | Burning , bursting and tearing sensations. |
| Modalities | < In winter—wants warmth externally and internally.< between sunrise to sunset, by cold and from standing, by motion.> by quiet, rest, and warmth.> In summer, from heat, hot application and by natural discharges such as urine, sweat, menstruation etc. | < by rest, damp, rainy, humid atmosphere, cold weather or changes of weather and by approach of a storm or during a thunderstorm, from meat< stooping, bending and beginning to move.> by moving, from slow motion, stretching and rubbing, pressure, by lying on the stomach or with pressure and in dry weather.> by unnatural discharges, and by unnatural elimination through the mucus surface, such as leucorrhoea, nasal discharge etc. | < from sunset to sunrise, at night or at approach of night, the seaside, sea voyages, thunderstorms, during summer and warmth, and extremes of temperature.< stormy weather and changes in the weather< movement, perspiration and the warmth of the bed.>from sunrise to sunset, in lukewarm climates and during the winter cold.> change in position, from any abnormal discharges. |
Conclusion
Osteoarthritis knee is not merely a mechanical wear-tear disease but a chronic constitutional disease reflecting deep-seated miasmatic influences. The pathological changes observed in knee osteoarthritis correspond closely with the miasmatic evolution as decribed by Hahnemann. A Homoeopathic approach, grounded in the understanding of pathology and miasmatic background, enables the physician to treat the patient holistically rather than focusing solely on the affected joint.
A Correct prescription can be made by primarily making the miasmatic diagnosis, secondarily assessing the totality of symptoms which include keynote symptoms and PQRS of the case and prescribe the indicated remedy according to the totality of symptoms. Ensure that this indicated remedy which encompasses miasm as well as totality of symptoms. By addressing the underlying miasm, Homoeopathy offers a rational, scientific, and individualized method of management for knee osteoarthritis, aiming not only at symptomatic relief but at long-term constitutional healing.
“Most of The Time We Fail to Select the True Basic Remedy Because We First Fail to Understand the Miasmatic Phenomena and The Relation They Bear to Each Other and to The Life Force.” – Dr. J H Allen
References
- Jameson, Fauci , Kasper , Hauser , Longo , Loscalzo. HARRISON’S
PRINCIPLE OF INTERNAL MEDICINE. 20th ed. Jameson JL, Kasper DL, Longo DL, Fauci AS, Hauser SL, Loscalzo J, editors.: Mc Graw Hill; 2018.p.2624-2631.
- Pal CP, Singh P, Chaturvedi S, Pruthi KK, Vij A. Epidemiology of Knee Osteoarthritis in India and Related Factors. Indian Journal of Orthopedics. 2016 september; volume 50(5): 518-522.
- Stanley D, Illustrations by Robert Britton. DAVIDSON’S principles and practice of Medicine. 23rd ed. Ralston SH, Penman ID, Strachan MW, Hobson RP, editors. EDINBURGH: ELSEVIER; 2018.p.1007-1012.
- Hsu H, Siwiec RM. www.ncbi.nlm.nih.gov/books/NBK507884/. [Online].; 2023 [cited 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507884/.
- Shenoy R. Essentials of orthopedics. 2nd ed. shetty fbMS, editor. new delhi: Jaypee brothers Medical Publishers(P)Ltd; 2014.p.242-244.
- Jaeschke R, Gajewski P, O’Byrne Pm. MC MASTER Textbook of internal medicine 2022. South Asian ed. Jaeschke R, editor. krakow: Medycyna Praktyczna; 2022.p.1506-1512.
- Sarkar BK. Hahnemann’s Organon of medicine. Sixteenth ed. Delhi: Birla PUBLICATIONS PVT.LTD.; 2016-2017.
- Samuel H. The Chronic Diseases their peculiar nature & their homoeopathic cure. reprint ed. new delhi: Indian books & Periodicals Publishers; 2016.
- Samuel H. Organon of medicine. sixth ed. new delhi: Indian Books & Periodicals Publishers; 2018.
- Banerjea DSK. MIASMATIC PRESCRIBING its philosophy, diagnostic classifications,clinical tips, miasmatic repertory miasmatic weightage of medicine and case illustrations. Second Extended Edition ed. NOIDA, New delhi: B. Jain Publishers (P) Ltd; 2024.