The Homeopathic Journey to Get Rid of Tinea Cruris
Abstract
Diseases caused by fungi can be divided into three broad groups: superficial mycosis, subcutaneous mycosis, and systemic mycosis. The superficial infection caused by the dermatophytes is called dermatophytosis and the term dermatomycosis refers to the infection from any of the fungi. Superficial fungal infections are some of the most common dermatologic diseases seen worldwide. Among superficial mycosis, dermatophytosis is the most common contagious infection. Dermatophytosis is a term used to describe mycotic infections caused by a group of fungi that usually remain localized to the superficial layers of the skin, hair, or nails. These fungi are classified in the anamorphic genera Epidermophyton, Microsporum, and Trichophyton. While T. Rubrum is the most common agent. As T. Ajelloi is an unusual isolate of superficial dermatophytosis, so the case is presented. The prevalence of an individual species in a given geographic location, and hence the disease it causes, is dependent on a number of factors including population migration patterns, lifestyle practices, primary host range, secondary host susceptibility, standard of living, and climatic preference.
Keywords: Tinea cruris Dermatophytes, Skin infection, Keratinophilic fungi
Introduction Superficial mycosis refers to fungal infections of skin and its appendages, hair and nail. It has been estimated that superficial mycoses are seen in 20-25% of the world’s population . Dermatomycoses is by far the most common fungal disease in human beings. Even though worldwide in distribution, they are mostly prevalent in tropical and sub-tropical countries like India. The hot and humid climate is supposed to aggravate the infection . The principal causative agents are dermatophytes, and their geographic distribution is variable. This is reflected in the differing patterns of dermatophytosis seen in different parts of the world. The epidemiology of dermatophyte infection has changed as a result of migration, lifestyle, drug therapy, and socioeconomic conditions.
Case :- A male 35 year old come on 30/02/2025 Presenting complaint
visited A male patient, aged 35years, the complaint of itching reoccurring with black discoloration . over the inguinal region since 2 years. The itching was very much aggravated at night which causes burning sensation after scratching. Sometimes there was slight watery discharge after scratching.



History of presenting complaints
The patient had previously suffered from skin complaints with lesions at the same locations two years ago for which she consulted a dermatologist and was diagnosed as Tinea Corporis. She took allopathic treatment including tablets , capsules and ointment for a long duration which subsided the skin complaint. After a few months, the same complaint arose diffusely over some parts of body for which she again took allopathic treatment. She remained free of complaint for sometime after which it recurred but this time over the areas of inguinal with great severity in itching and discomfort. Being on allopathic treatment for a long time, the patient was very much reluctant to use it anymore. On the advice of her relative, for a permanent solution to the problem, she finally visited our OPD.
Treatment adopted – allopathic
Result – No relief
Past History:- No history of serious and autoimmune disease.
Physical generals:- Diet : both (Vegetarian diet & non vegetarian)
Desire : Sweets & Cold things
Disagrees : gourd and pumpkin.
Thirst : 2-3 litters/ day.
Tongue : white coating
Taste : No altered taste as mentioned by the patient. Salivation : Moderate as per patient.
Perspiration : profuse.
Stool : irregularly but no complaint.
Urine : frequent (watery 8-9 times in 24 hrs.)
Bathing : Regularly.
Dwelling place : Well ventilated house with proper sunlight Appetite : constipation
Thermal : Chilly
Skin : Dry
Sleep:- Disturbed due to itching at night (4hrs/day )
Mental generals:-
Loquacity . extrovert ,Love his family.
religious person ,Hopeful .
Examination :-
BP-130/90mmhg
Pulse: 80beats/min
Temperature: 99°F
Respiration: 16 beats/ min
Abdomen – blotting for constipation
Local examination (Skin)
Inspection: – Border: Irregular, raised Colour: Hyperpigmented with erythematous at border
Weeping: Present after scratching
Crusting: Not present
Palpation: –
Tenderness: Not present
Surface texture: Rough
Associated signs: Nothing significant
Oedema: Mild oedema of the affected site
Elevation: At borders with reddish eruptions in circular fashion
Clinical Diagnosis: Tinea Cruris
Analysis of the Case
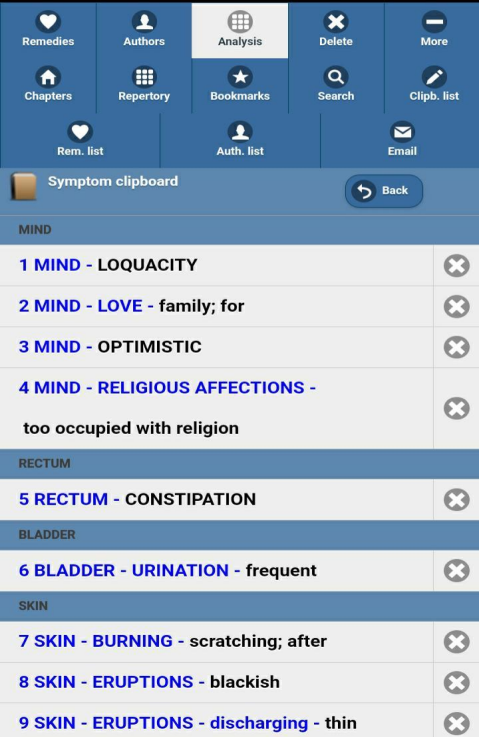
After detailed case taking, symptoms were analyzed and evaluated to construct the totality. The following characteristic mental general symptoms, as well as physical general and particular symptoms were considered for repertorization:
Personal History:-
The patient is a housewife belonging to a middle class Hindu family. All her children are unmarried. She lives with her husband and mother in law. There are no specific worries except her skin complaint which is of a recurring nature.
Family History:-
Father has been suffering from hypertension, mother has a history of hypertension and diabetes. The patient is married and has 2 children. Her relations with her husband are satisfactory. There are no financial issues as such in the family.
Miasmatic Result:- Psoric miasm
Differential Diagnosis:-
Seborrheic dermatitis, Candidal intertrigo ,Erythrasma Inverse psoriasis, Tinea cruris
Repertorial analysis:-
After the totality of symptoms was formed, repertorization was done by Synthesis repertory software.
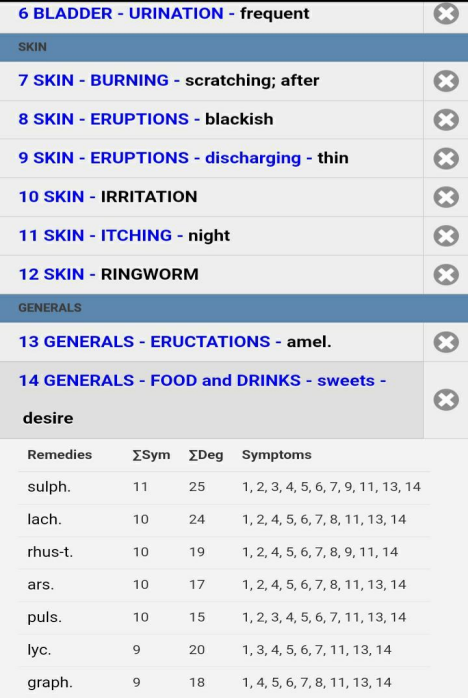
Prescription :- 30/02/25 Sulphur 30 BD for 1 day Rubrum met 30 BD for 10 days
Follow up:- 1. Itching decreased, no new eruptions, 10/03/25 Rubrum met 30 BD for 10 days 2. No new eruptions, no increase in itching.
Constipation relief, relax beforehand in frequent urination 20/03/25 Rubrum met 30 BD for 10 day
3. Itching reduced, eruptions reduced , mild discoloration are present
Common Homeopathic Remedies for Tinea Cruris:
1. Graphites
Useful when there is intense itching with oozing of a sticky, honey-like discharge.
Skin is often rough and dry.
2. Sulphur
Helpful when there is burning, redness, and itching, especially worse from warmth and bathing.
Suitable for people with a history of skin complaints.
3. Tellurium
Effective for ringworm-like eruptions that are itchy, red, and scaly.
Fungal infections that have a circular appearance and may spread rapidly.
4. Sepia
For itchy skin that gets worse from sweating, particularly in the groin.
Often useful in women with hormonal imbalance or chronic skin issues.
5. Thuja Occidentalis
Indicated in fungal infections and wart-like growths.
Can be useful if the skin symptoms are accompanied by suppressed discharges or vaccinations in the past.
References:-
1. Pariser RJ, Pariser DM. Primary care physicians‟ errors in handling cutaneous disorders. A prospective survey. J Am Acad Dermatol. 1987;17(2 pt 1):239-245.
2. Hay RJ, Clayton YM, De Silva N et al. Tinea capitis in south east London- a new pattern of infection with public health implications. Br J Dermatol. 1996;135:95595.
3. Weitzman I, Summerbell RC. The dermatophytes. Clinical microbiology reviews. Clin Microbiol Rev.1995;8:240.
4. Kelly BP. Superficial fungal infections. Pediatr Rev. 2012;33(4):22-37.
5. Blaithin Moriarty, Roderick Hay, Rachael Morris-Jones. The diagnosis and management of tinea. BMJ. 2012;345:4380.
6. Hay RJ, Jones RM. New molecular tools in the diagnosis of superficial fungal infections. Clin Dermatol. 2010;28:190-6.
7. John W. Ely, Sandra Rosenfeld, Mary Seabury Stone.
Diagnosis and Management
1. Pariser RJ, Pariser DM. Primary care physicians‟ errors in handling cutaneous disorders. A prospective survey. J Am Acad Dermatol. 1987;17(2 pt 1):239-245.
2. Hay RJ, Clayton YM, De Silva N et al. Tinea capitis in south east London- a new pattern of infection with public health implications. Br J Dermatol. 1996;135:95595.
3. Weitzman I, Summerbell RC. The dermatophytes. Clinical microbiology reviews. Clin Microbiol Rev.1995;8:240.
4. Kelly BP. Superficial fungal infections. Pediatr Rev. 2012;33(4):22-37.
5. Blaithin Moriarty, Roderick Hay, Rachael Morris-Jones. The diagnosis and management of tinea. BMJ. 2012;345:4380.
6. Hay RJ, Jones RM. New molecular tools in the diagnosis of superficial fungal infections. Clin Dermatol. 2010;28:190-6.
7. John W. Ely, Sandra Rosenfeld, Mary Seabury Stone. Diagnosis and Management of Tinea Infections. American Family Physician. 2014; 90(10).
8. Speight P. A Comparison of the Chronic Miasms, Psora, Pseudopsora, Syphilis, Sycosis. Reprint Edition. New Delhi: B. Jain Publishers (P) Ltd.; 1998. P. 1-87.
9. RADAR 10. Archibel Homoeopathic Software. Belgium. 2009.
10. Kent JT. Lectures on Homoeopathic Materia Medica. Second rearranged Edition. New Delhi: B Jain Publishers (P) Ltd.; 2009.p. 951-976.
11. Chitkara H.L. Best of Burnett. Reprint Edition. New Delhi: B. Jain Publishers (P) Ltd.; 2007.p.114.
12. Paterson C, Britten N. In pursuit of patientcentred outcomes: a qualitative evaluation of the “Measure Yourself Medical Outcome Profile.” J Health Serv Res Pol 2000;5(1):27- 36.
13. Reilly D, Mercer Stewart W, Bikker Annemieke P, Harrison Tansy. Outcome related to impact on daily living: preliminary validation of the ORIDL instrument. BMC Health Serv Res. 2007; 7: 139.
14. Van Haselen RA. Development of a supplement (HOM‑CASE) to the CARE clinical case reporting guideline. Complement Ther Med. 2016;25:78‑85.
15. Burnett J. Compton. Ringworm, its constitutional nature and cure. Boericke & Tafel; 1892.p.89-90.
16. Henny Heudens Mast. The foundation of the chronic miasms in the practice of Homoeopathy. First edition. Florida: Lutea Press; 2005.p.11.
17. Banerjee, SK. Miasmatic prescribing, its philosophy, diagnostic clinical tips, classifications, Miasmatic repertory, Miasmatic weightage of medicines and case illustrations. Second enlarged edition. New Delhi: B. Jain Publishers (P) Ltd.;p.3-6.
18. Pubmed [Internet]. Bethesda: US National Library of Medicine, National Institutes of Health 1988- [cited 2019 October 28].
Authors
Guided by :- Dr. Umesh masram { M.D. ( Hom.)
Department of Practice of Medicine, Government Homoeopathic Medical College & Hospital Bhopal, Madhya Pradesh, India
About the Author :-
Dr. Arvind kumar verma
Fellowship in dermatology , Department of Practice of Medicine, Government Homoeopathic Medical College and Hospital Bhopal, Madhya Pradesh, India.