

Abstract: Stroke occurs when blood supply to the part of brain is interrupted or reduced and brain tissues are unable to get oxygen and nutrients. It is the most prevalent cause of morbidity and mortality from neurological disease. Sudden loss of vision, sudden weakness of face and arm and slurred speech are its common presentation. Following article will simplifies the various etiology, types, clinical presentations and homoeopathic medicines along with appropriate rubric of stroke given in repertory.
Keywords: Stroke, homoeopathy, hypertension, thrombosis, atherosclerosis, apoplexy.
Abbreviations: Transient Ischemic Attack (TIA), ATP (adenosine tri phosphate), O2 (oxygen), Na (sodium). CT (computed tomography), ECG (electrocardiography), MRI (magnetic resonance imaging), FAST (face, arm, speech, time).
Introduction
Stroke can be defined as a sudden onset of focal neurological dysfunction due to vascular cause. Transient Ischemic Attack (TIA) usually lasts for minutes with complete recovery under <24 hrs. Stroke is a medical emergency which increases with the increasing age ( > 60 yrs ). Haemorrhagic stroke accounts for 15% of cases and occupy second position while ischaemic stroke on the other hand are responsible for 85% of cases and holds fourth spot in death all over globe. In India, cerebrovascular disease are placed on second position after ischaemic heart disease[1].
Table 1. showing risk factor and etiology of stroke
| Risk factors | Aetiology |
| Age: >60 | Thrombosis |
| Hypertension | Embolism |
| Diabetes | Hypertension |
| Hyperlipidaemia | Aneurysm |
| Alcohol | Vascular malformations |
| Obesity | Coagulopathy |
| Smoking | Vasculitis |
Pathology
Any decrease in level of O2 concentration below the threshold in cerebral circualation disposes brain to tissue damage. If homoeostatic mechanism kicks in time it result in a TIA. Any failure to do so causes ATP (adenosine tri phosphate) shortage which paves way for loss of membrane potential and increase influx of sodium (Na) and water into cells(cytotoxic oedema). Release of glutamate neurotransmitter further allow influx of calcium(activate intracellular enzymes) and more sodium into the neurons. Inflammatory mediators released by microglia and astrocytes causes death of all cell types in the area of maximum ischaemia. Fever and high blood glucose contribute in development of deficit. A structurally intact swollen ischemic tissue that surrounds the infarcted zone is called ischemic penumbra. A generalised reduction in blood flow to brain due to hypotension, cardiac arrest and shock causes global cerebral ischemia while decrease supply at a local level due to thrombosis or embolism results in focal cerebral ischaemia.[2]
Fig 1.Brain vascular anatomy[3]:
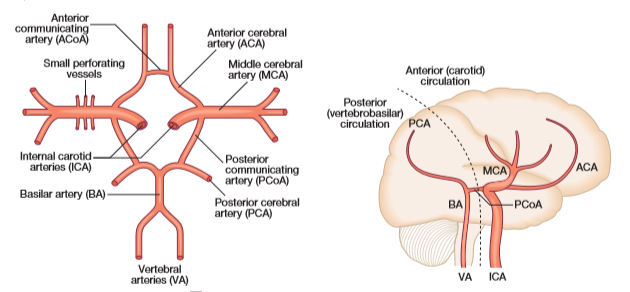
Blood supply to different regions of brain:[A] Horizontal view [B] Lateral view
Clinical features:
- TIA (Transient Ischemic Attack) is sudden loss of function with complete recovery and no evidence of infarction on imaging. Symptoms remain for very short span of time including amaurosis fugax, aphasia, hemiparesis, hemisensory loss and hemianopic visual loss.
- Cerebral infarction(85%): The clinical presentation of stroke depends on site
- Anterior circulation infarcts occur in territories of internal carotid, middle cerebral, anterior cerebral and opthalmic arteries. Symptoms are contralateral hemiplegia and facial weakness hemisensory loss and neglect syndromes, aphasia and hemianopia.
- Posterior circulation infarct affect brainstem, thalamus, hippocampus resulting in diplopia, vertigo, vomiting, choking and dysarthria, ataxia, hemisensory loss, hemianopic and bilateral visual loss, tetraparesis, loss of consciousness and transient global amnesia.
- Lacunar infarction are often asymptomatic but may present without cortical features, such as pure motor stroke, pure sensory stroke, sudden unilateral ataxia and sudden dysarthria with a clumsy hand.
- Watershed infarction due to cerebral hypoperfusion affect border zones and may cause loss of memory, vision and slight impairment in intellect.
- Haemorrhagic stroke(15%) are present with severe occipital headache accompanying vomiting and if timely intervention is not done followed by coma. They include intracerebral and cerebellar haemorrhage and subarachnoid haemorrhage[4].
Investigations:
Table.2 Investigations for determination of stroke
| Immediate | Within 24 hours | Additional |
| MRI Brain | Routine blood | CT or MR angiography |
| CT Brain | Lipids | CT Brain |
| Blood count | ECG | Echocardiogram |
| Glucose | Carotid Doppler | Antiphospholipid antibodies |
Differential diagnosis:
- Migraine
- Encephalitis
- Subdural or extradural haematoma
- Brain Tumor
Management: Strokeis a medical emergency. To educate general public, acronym FAST is used
- Face – sudden weakness of the face
- Arm – sudden weakness of one or both arms
- Speech – difficulty speaking, slurred speech
- Time – the sooner treatment can be started, the better.[4]
A. General management include airway patency, giving oxygen and maintaing blood pressure.
B. Medical management require thrombolytic, antiplatelet and anticoagulative therapy and decompressive craniectomy,
Secondary intervention:Anti hypertensive, lipid lowering, life style modification, exercise and physiotherapy, surgery and stenting for carotid stenosis.[4]
Homoeopathic management in stroke
In homoeopathic literature, apoplexy is the corresponding term for stroke. In this type of cases where evolution of disease from TIA to stroke needs to be arrested and acuteness of condition in haemorrhagic stroke demands a therapeutic selection, characteristic symptoms of patient can be crucial for medicinal differentiation. While the concept of thorough case taking and individualisation should be saved for chronic condition remaining thereafter.
Miasmtic evolution:
Atherosclerosis is a result of sycotic miasm. Structural changes underlie hypertension and aneurysm which is central to syphilitic miasm. Haemorrhagic tendencies do come under tubercular miasm[5].
Rubrics related to stroke are well placed in various repertories:
1. Rubrics of stroke from Repertory of The Homoeopathic Materia Medica by Dr J.T. Kent[6]–
- HEAD – CEREBRAL HAEMORRHAGE
- HEAD – CONGESTION
- HEAD – ANAEMIA
- EXTREMITIES – PARALYSIS – apoplexy, after
- EXTREMITIES – Upper Limbs – apoplexy
- EXTREMITIES – Lower Limbs – apoplexy
- EXTREMITIES – PARALYSIS – hemiplgia
- GENERALITIES – APOPLEXY
2. Rubrics of stroke from Synthesis Repertory[7]–
- HEAD – APOPLEXY
- HEAD – CEREBRAL HEMORRHAGE
- GENERALS – APOPLEXY
- GENERALS – APOPLEXY THREATENED
- GENERALS – PARALYSIS – oneside – apoplexy after
- EXTREMITIES – PARALYSIS – apoplexy after
- EXTREMITIES – PARALYSIS – hemiplegia
3. Rubrics of stroke from Homoeopathic Medical Repertory by Dr Robin Murphy[8]
- BRAIN – STROKE , apoplexy
- DISEASE – STROKE, apoplexy- paralysis from
- DISEASE – HYPERTENSION, high blood pressure
4. Rubrics of stroke from New Manual of Homeopathic Materia Medica & Repertory by Dr Boericke [9]–
- CIRCULATORY SYSTEM – RUPTURE OF ARTERY
- HEAD – BRAIN – Anaemia
- HEAD – BRAIN – Congestion
- HEAD – BRAIN – Paralysis
- NERVOUS SYSTEM – PARALYSIS
- NERVOUS SYSTEM – HEMIPLEGIA
- NERVOUS SYSTEM – PARAPLEGIA
Medicines having high therapeutic value in cases of stroke are [9]
Coffea cruda:. It is a remedy for threatened apoplexy. Pain as if nail driven in head with rapid high tension pulse and urinary suppression
Belladonna: It is suitable for confusion and cerebral irritation with hot head and cold feet. Congestive headache with throbbing of carotids. Acuteness of pain which resolve suddenly accompanied by vomiting.
Opium: Complete loss of consciousness in apoplectic state and dark red flushed face with paralysis. Pulse is low and full and there is dropping of lower jaw. Vertigo with head feels lights in old people.
Lachesis mutus: Left sided paralysis remaining after stroke. Hemorrhage of dark, profuse and non coagulable blood. Rush of blood to head causing pressure on vertex and headache with flickering dimness of vision.
Phosphorus: It causes fatty degeneration, congestion of blood vessels. Arms and hands become numb. Pulse rapid ,small and soft.
Baryta muriaticum: It is suitable for arteriosclerosis, aneurysm and cerebral affection with a high systolic pressure and a comparative low diastolic tension. Vertigo due to cerebral anaemia with noises in ears.
Causticum: Paralysis of right side of face. Gradually appearing local paralysis of vocal cords, muscles of deglutition, tongue, eyelids, face, bladder and extremities.
Aconitum napellus: Sudden, active cerebral congestion characterized by fear of death, restlessness, thirst. Pulse is full, hard and bounding. It used for congestive stage before localization take place[10].
Crotalus horridus[11] : Vertigo with weakness and trembling. Dull heavy occipital pain on right side and eye with dipolpia. Right sided paralysis
Arnica montana[11,12]: A remedy to prevent threatened apoplexy with red full face. Arnica is disposed to cerebral congestion, tendency to hemorrhage, to promote absorption of clots and helps in restoration of blood circulation where head and face feel hot while whole body is cold.
Discussion and conclusion
Homoeopathy is a system of medicine in which treatment is based on similarity of symptoms. Patient with stroke shows various symptoms on general and particular level. For homoeopathic prescription each symptoms narrated by patient is not equally important, but characteristic, rare, uncommon symptoms are key for prescription. However, the constitutional approach is most suitable way to find out similimum but at times patients are not in condition of giving case taking because of unconsciousness, dysarthria, hence a prescription based on acute totality is needed to give relief to the patient. Such type of prescribing helps the physician to deal with the acute severity of the case when symptoms agree.
References:
- Harrison T, Kasper D, Hauser S, Jameson J, Fauci A, Longo D et al. Harrison’s principles of internal medicine. 20th ed. New York: McGraw-Hill Education; 2018.
- Robbins, S., Cotran, R., Kumar, V., Abbas, A. and Aster, J., 2015. Pathologic Basis Of Disease. 9th ed. Philadelphia, PA: Saunders Elsevier.
- Ralston, S., Strachan, M., Britton, R., Penman, I. and Hobson, R., 2018. Davidson’s Principles & Practice Of Medicine. 23rd ed. Edinburgh: Elsevier.
- Kumar, P. and Clark, M., 2017. Kumar And Clark’s Clinical Medicine. 9th ed. Edinburgh: Elsevier.
- Robert HA. The principal and Art of Cure by Homoeopathy. New Delhi: B. Jain Publishers (P) Ltd.; 2002.
- Kent J. Repertory of the Homoeopathic Materia Medica. 6th ed. New Delhi: B. Jain Publishers (P) Ltd.; 2013.
- Schroyens F. Synthesis Repertorium Homoeopathicum Syntheticum. (9.1st ed). New Delhi: B. Jain Publishers Private Ltd.; 2008.
- Murphy Robin. Homoeopathic Clinical Repertory. 2nd ed. New Delhi: B.Jain Publishers (P) Ltd; 2003.
- Boericke W., 9th Edition, New Manual of Homoeopathic Materia Medica and Repertory; Augmented, B. Jain Publisher (P) Ltd., New Delhi, (2000).
- Allen HC. Keynotes rearranged and classified with leading remedies of the materia medica and bowel nosodes. New Delhi: B. Jain Publishers (P) Ltd.; 2012.
- Khuwaja Gulrana, Ishrat Tauheed, Khan M Badruzzaman, Raza
Syed Shadab, Ahmad Khan M Moshahid, Ahmad Ajmal, Vaibhav Kumar, Khurana Anil,
Islam Fakhrul
Protective role of homoeopathic medicines on cerebral ischaemia in animals
Year : 2014 | Volume: 8 | Issue Number: 4 | Page: 209-217 - Mueller, Manfred. Homeopathic Treatment of Brain Hemorrhage: Several Cases. American Homeopath. 19. 15, 2013.
About Author: Dr Ashok Yadav1 Dr Virendra Chauhan2 Dr Nipun Singh Dabi3
1 Professor, HOD, Dept. of Practice of Medicine, Dr. M.P.K. Homoeopathic Medical College, Hospital & Research Centre , Homoeopathy University, Jaipur, Rajasthan.
2 Professor, Dept. of Practice of Medicine, Dr. M.P.K. Homoeopathic Medical College, Hospital & Research Centre , Homoeopathy University, Jaipur, Rajasthan.
3 MD Scholar, Dr. M.P.K Homoeopathic Medical College, Hospital & Research Centre, Homoeopathy University, Jaipur, Rajasthan.



