Dr. Trapti Goel
(MD scholar, Department of Repertory, Bakson Homoeopathic Medical College & Hospital, Greater Noida, UP)
(BHMS, Nehru Homoeopathic Medical College & Hospital, University of Delhi, Defence Colony, New Delhi)
Abstract:
Rheumatoid Arthritis (RA) is an autoimmune disease causing a symmetrical polyarthritis with systemic involvement. It has extremely variable course and it is also associated with non-articular features. Rheumatoid arthritis is remitted and exacerbated specially in winter and rainy season. In this article we will discuss epidemiology, risk factors, pathogenesis, clinical presentation, differential diagnosis, general and conventional management. We will also discuss the role of Homoeopathy in management of rheumatoid arthritis whether it’s a chronic arthritis or sudden exacerbation of arthritis.
Introduction:
Rheumatoid arthritis is symmetric polyarthritis with predilection for small joints of the hands and feet, deformities are common with progressive disease. Major manifestation of Rheumatoid arthritis is synovitis of multiple joints. RA is a significant cause of disability and mortality and carries a high socio-economic cost. The condition can present itself in any age, but the probability increases with age. It is a heterogenous disease with variable severity, unpredictable course, and a variable response to drug treatment.
Epidemiology:
The disease prevalence worldwide is approximately 0.8% (0.3% to 2.1%) of the population. In India, the prevalence of RA is 0.5% to 0.75%. The peak age of onset is in the fourth and fifth decade of life with more than 75% patients developing disease between 30 and 50 years of age.
Risk Factors:
Exact cause of RA is Unknown.
However, cause is thought to be multifactorial along with genetic and environmental factors.
- Gender: Women before the menopause are affected three times more often than men (3:1).
After the menopause the frequency of onset is similar between the sexes, suggesting an etiological role for sex hormones.
- Familial: Increased incidence in first degree relatives.
- Genetic factors are estimated to account for upto 60% of disease susceptibility. There is a string association between susceptibility to RA and certain HLA halo types. HLA -DR4, which occurs in 50-75% of patients, correlates with a poor prognosis.
- Climate: Temperate zones with cold and damp climate.
- Psychological factors: Excessive and continuous stress.
- Nutrition: Malnourished are more affected.
- Cigarette smoking is a strong risk factor for developing RA and also associates with greater severity.
Pathogenesis:
RA is characterized by infiltration of the synovial membrane with lymphocytes, plasma cells and macrophages. CD4+ T cells play a central role by interacting with other cells in the synovium. Activated T cells stimulate B cells to produce immunoglobulins including RF, and macrophages to produce pro-inflammatory cytokines.
These act on the endothelium, synovial fibroblasts, bone cells and chondrocytes to promote swelling and congestion of synovial membrane and destruction of bone, cartilage and soft tissues. The B-cells release immunoglobins, including RF, which can form immune complexes within the joint and in extra-articular tissues, leading to vasculitis.
Lymphoid follicles form within the synovial membrane. Inflammatory granulation tissue (pannus) spreads over and under the cartilage, which is progressively eroded and destroyed. Later, fibrous or bony ankylosis may occur. Muscles adjacent to inflamed joints atrophy and may get infiltrated with lymphocytes.
Rheumatoid nodules consist of a central area of fibrinoid material surrounded by a palisade of proliferating mononuclear cells. Similar granulomatous lesions may occur in pleura, lung, pericardium and sclera.
Clinical features:
Presentations of Rheumatoid arthritis:
- Palindromic: Monoarticular attacks lasting 24-48hours; 50% progress to other types of RA.
- Transient: A self- limiting disease, lasting less than 12months and leaving no permanent joint damage.
- Remitting: There is a period of several years during which the arthritis is active but then remits, leaving minimal damage.
- Chronic, persistent: Most typical form, it may be seropositive or seronegative for IgM rheumatoid factor. Follows a relapsing and remitting course for years. Seropositive (plus anti- CCP) patients tend to develop greater joint damage and long-term disability.
- Rapidly progressive: The disease progress rapidly to severe joint damage and disability. It is usually seropositive (plus anti- CCP), has a high incidence of systemic complications and is difficult to treat.
Symptoms:
- Initially tiredness, general weakness, numbness and tingling in hands and feet.
- Loss of weight and generally debility.
- Vasomotor disturbances.
- Morning stiffness.
- Painful sensation in walking on soles.
- The most frequently affected joints are proximal interphalangeal and metacarpophalangeal joints of fingers, toes and knee, wrist, ankles.
Signs:
Joint Involvement
- Small joints of fingers and toes are involved first.
- Warmth over affected joints.
- Later-on big joints like knees, shoulders may be involved. Muscular stiffness worse in morning. Swelling of proximal interphalangeal joints; gives a spindle shaped swelling.
Muscular wasting
Constitutional symptoms: Fever, lymphadenopathy, splenomegaly.
Specially in children where it is called ‘ Still’s disease’.
Deformities: Swan neck deformity, ulnar deviation of fingers, ‘Z’ deformity of thumb, the boutonniere or ‘button hole’ deformation, subluxation of the ulna at the distal radio-ulnar joint, triggering of fingers, ‘cock-up’ toe deformities. Loss of the longitudinal arch (flat foot), Popliteal (Baker’s) cysts.


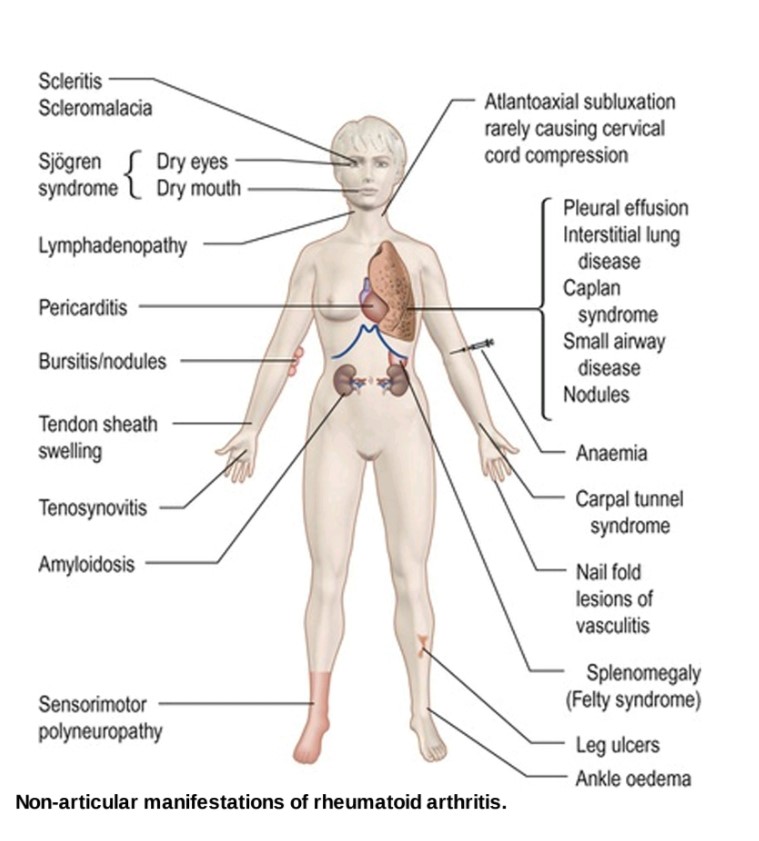
Extra – articular manifestations
- Rheumatoid nodules
- Rheumatoid vasculitis
- Felty’s syndrome
- Pleuro – pulmonary involvement
Investigation:
- Blood
- ESR Raised
- CRP Raised
- PMN Leucocytosis
- Altered plasma protein pattern
- Anemia: Hypochromic or normochromic, normocytic.
- Serology
- Anti – CCP is positive in earlier disease and in early inflammatory arthritis indicates the likelihood of progressing to RA.
- Rheumatoid factor is present in approximately 70% of cases.
- ANA at low titre in 30%.
- X – ray
- Joints will show de-mineralisation of bony ends.
- Narrowing of the joint space.
- Marginal erosion, cysts.
- Sub – cutaneous nodules.
- Arthroscopy
- Synovial biopsy
- MRI
Diagnosis Criteria:
According to American Rheumatism Association 1988 revision, Diagnosis of RA is made with four or more of the following:
- Morning stiffness (>1hr)
- Arthritis of three or more joint areas.
- Arthritis of hand joints.
- Symmetrical arthritis.
- Rheumatoid nodules.
- Rheumatoid factor.
- Radiological changes.
- Duration more than or equivalent to 6weeks.
Differential diagnosis:
- Rheumatic fever: Big joints are involved, arthritis is fleeting type, cardiac involvement present. Anti – streptolysin O titre in the blood is increased.
- Osteoarthritis: Weight bearing joints like hips and knees are involved. Herberden’s nodes are present. Early morning difficulty in movement and osteophytes in X-ray and normal ESR.
- Tuberculous Arthritis: History of trauma and single joint Involvement.
- Gouty Arthritis: History of acute gouty attack with involvement of big toe first, gouty tophy may be present and increased uric acid in blood.
- Psoriatic Arthritis: Terminal inter-phalangeal joints.
- Reiter’s syndrome: More common in males. Polyarthritis, non-gonococcal urethritis and conjunctivitis.
- SLE (Systemic Lupus Erythematous): Malar rash, Discoid rash, Photosensitivity, Oral ulcers, Serositis etc. Anti – DNA antibody & Anti -Sm usually present.
Management:
Patients with RA need constant advice and support from physiotherapist. A combination of rest for active arthritis and exercises to maintain joint range and muscle power is essential. Exercise in a hydrotherapy pool is popular and effective. Good posture, firm mattress, a firm back rest and minimum number of pillows should be used. Weight bearing on affected joint should be avoided. Hot bags, warm tub baths to decrease inflammation.
Diet: High Calorie, high protein, well balanced diet, including milk, eggs and fruits.
Conventional Treatment:
NSAIDs, coxibs, Corticosteroids, DMARDs like sulfasalazine, methotrexate, leflunomide and TNF -alpha blockers are used.
Homoeopathic Management:
Homoeopathic medicines can be used on the basis of the similarity of drug symptoms with totality of symptoms of patient. Few of the Homoeopathic medicines along with their symptoms, which can be used in the management of rheumatoid arthritis are:
- Abrotanum: For the Excessive pain before the swelling commences; from suddenly checked diarrhea or other secretions; alternates with hemorrhoids, with dysentery. Very lame and sore all over.
- Actea Spicata: Rheumatic remedy especially of the small joints; tearing, tingling pains characterize it. Wrist Rheumatism. Pains worse from touch and motion.
- Bryonia: Hot feeling of feet. Joints red, swollen, hot, with stitches and tearing; worse least movement. Every spot is painful to pressure.
- Causticum: Rheumatic tearing in joint, warmth and moving about relieves.
- Caulophyllum: Severe drawing, erratic pains and stiffness in small joints, fingers, toes etc. Aching in wrist joints, cutting pain on closing fist. Erratic pains, changing place every few minutes
- Colchicum: It has a special affinity for fibrous tissues, tendons, ligaments and periosteum. It has shifting arthritis; pains are worse in evening. Joints are swollen and dark red; suitable for weak, debilitated persons, specially a remedy for smaller joints of hands and feet.
- Guaicum: Rheumatism pains in shoulders, arms and hands; joint swollen, painful and intolerant of pressure; can bear no heat, contracture of joints.
- Kalmia: Arthritis of upper parts of the arms, and the lower parts of leg, worse from going to sleep; shifting or migrating pain; great weakness.
- Ledum Pal: Tearing pains, in smaller joints, travel upwards; very little effusion; symptoms worse from warmth of bed.
- Pulsatilla: When knee, ankle and the tarsal joints are involved; pains are so severe that the patient is compelled to move; migrating pains relieved by slow motion; joints swollen and a feeling of ulceration under the surface.
- Stelleria Media: Chronic Rheumatoid arthritis, shifting pains. Synovitis, worse in morning, enlarged and contracted joints.
- Viola odorata: Pressing pain in right carpal and metacarpal joints.
Conclusion:
Rheumatoid arthritis being a joint disorder, can be treated with Homoeopathy, after proper case taking and prescription of simillimum on the basis of totality of symptoms. Early intervention with Homoeopathy in cases of RA has shown remarkable scope. In cases where deformities and extra articular manifestations are present, we can stop the progress of symptoms with similimum, proper diet, stress and sleep management, although deformities can’t be reversed. Sudden exacerbation of arthritis can be managed with acute Homoeopathic Medicines like Belladona, Rhustox, Bryonia etc.
References:
- Kumar Praveen, Clark Michael. Kumar & Clark’s Clinical Medicine. Saunder’s Elsevier publication. Ninth Edition. 2017
- Munjal Y.P. API textbook of Published by The Association of Physicians of India. 10th Edition. 2014
- Papadakis A Maxine, McPhee J Stephen. Current Medical Diagnosis & Treatment 2020. McGraw hill publications. Fifty ninth Edition. 2020
- Kansal Kamal, Kaushal Rakesh. Textbook of Practice of Medicine with Homoeopathic therapeutics. B.Jain publishers (P) Ltd. Revised and enlarged edition. 2006
- College R. Nicki, Walker R. Brian, Ralston H. Stuart. Davidson’s Principles and practice of Medicine. Churchill Livingstone Elsevier. 21st edition. 2010
- Boericke William. Boericke’s new manual of Homoeopathic Materia Medica with Repertory. Third revised and augmented edition based on ninth edition. B. Jain publishers (p) ltd. 2007
- Allen C. H. Keynotes rearranged and classified with leading remedies of the materia medica and bowel nodes. B. Jain publishers (P) ltd. Tenth Edition.2007