ABSTRACT: This article discusses a case of septic gangrene of the foot in an elderly man whose prognosis was poor given that amputation of the leg below the knee was advised. Patient was completely cured with the help of remedy, Gun powder and Insulinum, without amputation.
A male patient of 53 years belonging to Ilkal, Karnataka has presented with the complaint of pain and numbness in lower extremities on 18-4-2020. Patient cannot walk without support of walker. All the complaints started 4 months back. Patient is diabetic since 12years and is on allopathic prescription. Based on the presenting complaint of the patient, the homoeopathic medicine Gun powder and Insulinum were prescribed, which proved to be effective in treating the diabetic wet gangrene without foot amputation. In this case, a patient of diabetic wet gangrene was completely cured with homoeopathic medicines, Gun Powder and Insulinum without the foot amputation.
KEY WORDS: homoeopathy, diabetic wet gangrene, Gun powder, Insulinum, NECROSIS.
ABBREVIATIONS: peripheral arterial disease (PAD), diabetes mellitus (DM), ankle brachial index (ABI), computed tomographic (CT) scan, magnetic resonance imaging (MRI), bilateral (B/L)
INTRODUCTION: Diabetes occurs due to impairment in either pancreatic production of insulin or utilisation of the produced insulin. It is one of the leading causes of deaths worldwide. It is associated with various complications and reduced quality of life. Among these, foot complications remain an important concern. The major foot complications include foot ulceration, cellulitis, abscess, wet gangrene, dry gangrene, and necrotising fasciitis, with different pathophysiological concepts behind each of them. As per the World Health Organisation, there are always higher chances of limb amputation among diabetic patients as compared to non-diabetics1.
Gangrene usually represents a late manifestation of peripheral limb ischaemia in patients with diabetes mellitus, often requires amputationand may result in death. Gangrene caused by peripheral arterial disease (PAD) is commonly aseptic or non infected and has a ‘dry’ appearance, whereas gangrene caused by bacterial infections or sepsis has a ‘wet’ appearance. Dry gangrene is usually less severe than wet gangrene and may result in auto amputation (i.e. spontaneous detachment from the body and elimination of a gangrenous part), whereas wet gangrene may lead to cellulitis, loss of the extremity, septicaemia and death. Diabetic ischaemic peripheral gangrene most commonly affects the toes/digits, feet and in some cases the entire leg2.
Foot gangrene, defined as dead tissue in the foot resulting from inadequate blood flow supply, is one of the manifestations of critical limb ischemia. It can be caused by obstructed peripheral circulation or bacterial infections. Foot ulcers in patients with diabetes are at an increased risk of foot gangrene, mainly due to peripheral arterial disease (PAD) and foot infections.
Foot gangrene can be classified into two types: (1) dry gangrene with ischemic tissue but no infection, and (2) wet gangrene with both infectious and necrotic tissue. Infectious foot gangrene (wet gangrene) is both a limb- and life-threatening disease
Diabetic foot ulcers are an injury to all layers of skin, necrosis or gangrene that usually occur on the soles of the feet, as a result of peripheral neuropathy or peripheral arterial disease in diabetes mellitus (DM) patients.
Understanding diabetic foot ulcers include necrosis or gangrene. Diabetic gangrene is a tissue death caused by a blockage of blood vessels (ischaemic necrosis) due to micro emboli atherothrombosis which is caused by occlusive peripheral vascular disease that accompanies diabetics as a chronic complication of diabetes itself. Diabetic foot ulcers can be followed by bacterial invasion resulting in infection and decay, can occur in any part of the body especially in the distal part of the lower leg.
Aetiology of diabetic foot ulcers:
- Causative factor, peripheral neuropathy (sensory, motor, autonomic), the main and most important causative factors. Sensory neuropathy is usually fairly deep (>50%) before experiencing a loss of protective sensation which results in susceptibility to physical and thermal trauma, thus increasing the risk of foot ulcers. Not only the sensation of pain and pressure are lost, but also the proprioception of the sensation of foot position also disappeared. Motor neuropathy affects all the muscles in the legs, resulting in protrusion of abnormal bones, normal architecture of the foot changed, distinctive deformity such as hammer toe and hallux rigidus.
- Autonomic neuropathy is characterised by dry skin, no sweating and increased secondary capillary refill due to arteriovenous shorts in the skin, triggering fissures, skin crust, all make the foot vulnerable to minimal trauma. High foot plantar pressure The second most important causative factor.
- Trauma, especially recurring trauma, 21% trauma from friction from footwear, 11% due to foot injuries (mostly due to fall), 4% cellulitis due to tinea pedis complications and 4% due to fingernail cut errors.
- Contributive factor: Atherosclerosis due to peripheral vascular disease, especially regarding the blood vessels of femoropopliteal and small blood vessels below the knee, is the most important contributing factor. The risk of ulcers, twice as high in diabetic patients as compared to non-diabetic patients.
- Diabetes leads to intrinsic wound healing, including collagen cross-linking disorders, metricoproteinase matrix functional disorders and immunologic disorders. In addition, diabetics have higher rates of onychomycosis and tinea infections, so the skin is easy to peel and infections. In DM, characterised by sustained hyperglycaemia as well as increased inflammatory mediators, triggering an inflammatory response, leading to chronic inflammation, but this is considered to be low-grade inflammation,
Clinical diagnosis of diabetic foot ulcers and management of diabetic ulcers consists of:
- Determining and repairing the underlying cause of ulcer disease, good wound care, and prevention of ulcer recurrence. The cause of diabetic ulcers can be determined precisely through deep anamnesis and physical examination.
- History: Symptoms of peripheral neuropathy include hyperaesthesia, paraesthesia, dysesthesia, radicular pain and anhidrosis.
- Most people with atherosclerotic disease in the lower extremity are asymptomatic, patients who show symptoms are found claudication, ischemic pain at rest, non-cured wounds and obvious leg pain. Cramps, weakness and discomfort in the legs are often felt by diabetics because of their tendency to suffer from occlusion of tibioperoneal atherosclerosis. Ulcers can arise in malleolus because in this area it often gets traumatized.
- Other abnormalities found in the physical examiner include: hypertrophic callus, brittle or broken nail, hammer toes and fissure. Assessment of possible vascular insufficiency. Physical examination shows the disappearance or decrease of the peripheral pulse below a certain level.
- Other findings associated with atherosclerotic disease include bruits on the iliac and femoral arteries, skin atrophy, hair loss in the legs, cyanosis of the toes, ulceration and ischemic necrosis, both pale feet when the foot is raised as high as the heart for 1-2 minute.
- Non-invasive vascular examinations include measurements of transcutaneous oxygen, ankle brachial index (ABI), systolic pressure of the toes. Ankle brachial index is a non-invasive examination that is easily performed using the Doppler tool.
- Peripheral neuropathy signs include loss of sensation of vibration and position, loss of deep tendon reflex, tropical ulceration, foot drop, muscle atrophy and hypertrophic callus formation especially in the pressure areas.
- Neurologic status can be examined using the Semmes-Weinsten monofilament to determine if the patient still has a “protective sensation”.
- Blood tests: leucocytosis may indicate an abscess or other infection of the foot. Wound healing is inhibited by the presence of anaemia.
- Metabolic profile: measurement of blood glucose, glycohaemoglobin and serum creatinine helps to determine the adequacy of glucose regulation and renal function.Radiological examination.
- A plain examination of the diabetic foot may show demineralisation and the charcot joint and the presence of osteomyelitis.
- Computed tomographic (CT) scan and magnetic resonance Imaging (MRI): although an experienced examiner can diagnose an abscess with a physical examination, a CT scan or MRI may be used to help diagnose an abscess if the physical examination is unclear.3
CASE REPORT: Initially, patient experienced numbness in the bilateral limbs for a month. Later, there was pain and blackish discolouration of bilateral legs and feet. Later after a month eruptions started on bilateral legs with oozing of foul smelling discharge. Then the eruptions turned into necrosis with the exposure of underlying femur. Patient was advised for bilateral feet amputation.
FAMILY HISTORY: No family history of any major illness.
PERSONAL HSITORY: Diet- mixed, appetite: 3meals /day, increased since 1 month, sleep: refreshing, bowels: regular, micturition: increased frequency.
General physical examination: patient is well oriented will time, place and person.
Weight: 67 kg
On Examination: offensive discharge from the necrosed bilateral legs and feet.
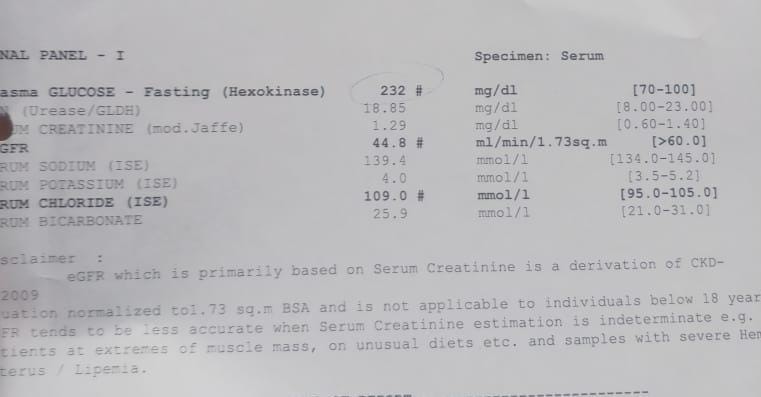
INVESTIGATION: 16-3-2020
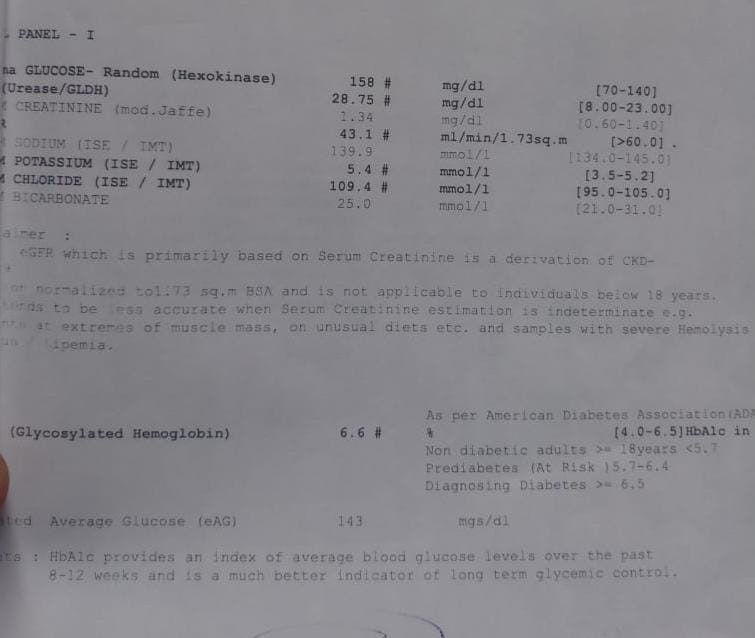
INVESTIGATION : 17-4-2020
DIAGNOSIS: DIABETIC WET GANGRENE3
ANALYSIS OF THE CASE
| COMMON SYMPTOMS: Numbness with tingling sensation in bilateral legs and toes. Pain and blackish discolouration of bilateral legs and feet. Eruptions on bilateral legs with oozing of foul-smelling discharge. Necrosis with the exposure of underlying femur. Foul smelling discharge from the necrosed lower limbs | UNCOMMON SYMPTOMS Diet: mixed.Appetite: increased since a month.Sleep: slightly disturbed. Bowels: regular. Micturition: frequency increased.Irritability, restlessness, depressed that he cannot walk, fear of losing lower limbs. |
EVALUATION OF THE CASE:
| MENTAL GENERALS: Irritability. Restlessness. Depressed that he cannot walk.Fear of losing lower limbs. | PHYSICAL GENERALS: Diet: mixed.Appetite: increased since a month. Sleep: slightly disturbed. Bowels: regular. Micturition: frequency increased. | CHARACTERSTIC PARTICULARS: Numbness with tingling sensation in bilateral legs and toes. Pain and blackish discolouration of bilateral legs and feet. Eruptions on bilateral legs with oozing of foul smelling discharge. Necrosis with the exposure of underlying femur. Foul smelling discharge from the necrosed lower limbs |
TOTALITY:
- Numbness with tingling sensation in bilateral legs and toes.
- Pain and blackish discolouration of bilateral legs and feet.
- Eruptions on bilateral legs with oozing of foul smelling discharge.
- Necrosis with the exposure of underlying femur.
- Foul smelling discharge from the necrosed lower limbs.
- Irritability, restlessness, depressed that he cannot walk, fear of losing lower limbs.
- Diet: mixed, appetite: increased since a month, sleep: slightly disturbed, bowels: regular, micturition: frequency increased.
DISCUSSION:
GUNPOWDER4: CLINICALS: Abscesses. Acne. Bites. Blood-poisoning. Boils. Carbuncles. Cuts, poisoned. Ivy (Hedera) poisoning. Osteo-myelitis. Tonsillitis, septic. Vaccinosis. Worms. Black Gunpowder is a mixture and not a chemical compound. But for all that, it is a unit, and can be used as such in medicine. As it contains three potent remedies, two of them polychrests, there is little wonder at its medicinal powers. “Blood-poisoning.” Gunp. corresponds to suppuration in a great number of forms, many of them septic.
Gun powder was first published in Homoeopathic world, London 1914 by Clarke, Av combination remedy of carbon, sulphur, and potassium nitrate. Useful for all kinds of blood poisoning, for septic wounds and ptomaine poisoning. Strong history of use in war time, particularly world war 1 and 2. Gunshot wounds, surgical septicaemia, boils, methane poisoning. Wartime ailments.4
Blood disorders, blood poisoning from pyorrhoea alveolaris. Septic suppurations. Infected wounds. Wounds that refuse to heal, abscessed bites, infections and wounds, antiseptic. Swollen and abscessed glands.
Poisoning from bad food or water. Poisoning from meats that have been unsuccessfully tinned. Acute infections, boils, abscesses, carbuncles, and bites.
Antidoting the ill effects of vaccination. Preventive for various kinds of inoculations. Gonorrhoea and syphilis. Shingles of face and eyes.
Dr. Clarke referred to the old-fashioned gun powder that was in use before the era of high explosives and smokeless powder. black gunpowder is a mixture and not a chemical compound . it contains three remedies , two of the polychrests Nitre with Sulphur and charcoal forms gunpowder. In lower trituration , gunpowder has cured ascarides in adults .
The London police Force also knew it as boil remedy.
Canon Roland Upcher noted that Norfolk shepherds rubbed gunpowder on to sheep’s wounds made during sheep-shearing , and took it to cure or prevent ill effects from handling sheep who suffered from ‘foot-rot’.
Upcher published cases of skin eruptions caused by handling ivy, cured with Gunpowder3x.
Clarke experimented with Gun powder 2x and developed severe herpes facialis involving the right eyebrow and right side of the nose.
Clarke confirmed the proving by curing Shingles. He heard of a case of lumbrici cured with an infusion of Gun powder by the patient.
A woman who had very sensitive skin was bitten by a gnat on the foot, resulting in swelling inflammation and suppuration .There was a ring of inflammation around the bite, constantly spreading and detaching the epidermis as it spread , after the failure of several medicines, Gun powder 3x rapidly cured.
A man had a bad cut with a knife on the left index finger . The wound refused to heal . An inflammatory ring striped off the epidermis and spread more and more . Lachesis mutus and other remedies failed to make any impression , Gun powder rapidly cured.
Another women was very severely poisoned by sewer gas . There followed swelling of the right arm and axillary glands of the right side. 3 months after the accident the right arm was almost fixed at the elbow above and below. The axillary glands were as large as hen’s egg. Gun powder 3x gradually resolved the trouble and motility of arm was fully restored4.
INSULINUM5: An active principle from the pancreas which affects sugar metabolism.
Besides the use of Insulin in the treatment of diabetes, restoring the lost ability to oxidise carbohydrate and again storing glycogen in the liver, some use of it homoeopathically has been made by Dr Wm. F. Baker, showing its applicability in acne, carbuncles, erythema with itching eczema. In the gouty, transitory glycosuria when skin manifestations are persistent give three times daily after eating. Given a persistent case of skin irritation, boils or varicose ulceration with polyuria, it is indicated.
CLINICALS: Abscesses, acidosis, Acne, bed sores, boils, cancer, dermatitis, diabetes, diarrhoea, carbuncles, gout, glycosuria, hepatitis, enlarged liver, varicose ulcers, marasmus, otitis, pneumonia, polyuria.
The pancreatic hormone plays an important part in the process of sugar metabolism in the body . its capacity to burn the sugar into carbon di oxide and water , thereby helping the body with combustion. If insulin is administered at suitable intervals , the blood sugar is maintained at normal level and the urine remains free of sugar . restores the ability to restore carbohydrates, and to store glycogen in the liver.
It was proved by Dr William F Baker, and Dr S. K . Josh of Calcutta . some sue of insulin homoeopathically has been made by Baker, showing its applicability in acne, carbuncles, erythema, with itching eczema.
Insulin is indicated for persistent cases of skin irritation, boils, varicose ulcers with polyuria,
For gouty patients with glycosuria when skin manifestations are persistent it is indicated.
Dr Ghose used it in potency for overdoses of insulin, followed by weakness, fatigue and tremulousness with profuse sweating . patient is debilitated , Asthenia, Emaciation with loose bowels, craving for sweets.
Abdomen:– duodenal ulcers, chronic intestinal troubles with diarrhoea and enlarged liver.
Blood: hypoglycaemia, septicaemia.
Food: desires sugar and sweets, but aggravated by them.
Liver: hepatitis, chronic functional derangement of liver.
Skin: acute dermatitis with chronic diarrhoea and liver trouble eczema, acne, erythema, suppurative ailments with enlarged liver5.
PRESCRIPTION :1)Gun powder 3x
3-3-3 /7 days
2) Insulinum 30
4-0-4/7days
FOLLOW UP after 7days.
FOLLOW UP:
| DATE 6-5-2020 15-5-2020 4-6-2020 25-6-2020 11-7-2020 26-7-2020 | FOLLOW UP Numbness with tingling sensation in bilateral legs and toes > Pain and blackish discolouration of bilateral legs and feet. Persists Eruptions on bilateral legs with oozing of foul smelling discharge,> Necrosis with the exposure of underlying femur, persists. Foul smelling discharge from the necrosed lower limbs, slightly > Irritability, restlessness, depressed that he cannot walk, fear of losing lower limbs,> All generals are good Foul smelling discharge from the necrosed lower limbs, > Numbness with tingling sensation in bilateral legs and toes> All generals are good. Patient is able to walker without the walker. Foul smelling discharge from the necrosed lower limbs > Pain and blackish discolouration of bilateral legs and feet,> All generals are good. Eruptions on bilaterak legs and feet ,> Pain and blackish discolouration of bilateral legs and feet,> Patient is able to walker without the walker.Patient feels confident.All generals are good. Necrosis with the exposure of underlying femur>.Revascularisation in B/L lower limbs is established. Patient is completely better.Can walk without the support of walker.All the generals are good |
REMEDY
Gunpowder
3x
3-3-3 /7 days
Insulinum
30
4-0-4/7days
Gunpowder
3x
3-3-3 /15 days
Insulinum
30
4-0-4/15days
Placebo
3-3-3/15days
Gunpowder
3x
3-3-3 /15 days
Insulinum
30
4-0-4/15days
Gunpowder 3x 3-3-3 /15 days Insulinum 30 4-0-4/15days Placebo 3-0-3 /7 days |
BEFORE THE HOMOEOPATHIC TREATMENT : THE CASE WAS ADVISED FOR AMPUTATION

CONCLUSION: Patient has completely recovered by homoeopathic treatment within a span of 3months without the lower limb amputation. This proves that homoeopathic medicines can do wonders in such complicated cases. As the patient belonged to the low- socio economic status and was the only bread winner of the family, he was quite depressed of his condition. In such cases, omoeopathic treatment helps in providing a better quality of life to the patients.
REFERENCES:
- Alzahrani H, Bedir Y, Al-Hayani A. Efficacy of shellac, a natural product, for the prevention of wet gangrene. Journal of international medical research, 2013 June 4th.
- Haimovici H, Gangrene of the extremities of venous origin: review of the literature with case reports. Circulation, 1950 Feb 1st.
- Rosyid FN, Etiology, pathophysiology, diagnosis and management of diabetics foot ulcer. International Journal of Research in Medical Sciences, 2017 Oct 5th .
- Clarke JH, A practical dictionary of Materia Medica, B Jain publishers
- Murphy R, Lotus Materia Medica, B Jain Publishers.
ABOUT THE AUTHOR:
DR AMALA.A(MD-1)
DEPARTMENT OF PAEDIATRICS
FATHER MULLER HOMOEOPATHIC MEDICAL COLLEGE