Management of Rheumatoid Arthritis By Homoeopathic Medicines
Abstract:- Rheumatoid arthritis (RA) is a chronic, systemic autoimmune disorder primarily affecting the synovial joints, leading to progressive inflammation, pain, swelling, and joint deformity. The disease results from an aberrant immune response that targets the synovial membrane, causing synovial hyperplasia, cartilage destruction, and bone erosion. Genetic factors, such as HLA-DR4 and HLA-DR1 alleles, along with environmental triggers like smoking and infections, contribute to disease susceptibility. Clinically, RA presents with symmetrical polyarthritis, morning stiffness, and systemic manifestations including fatigue, anemia, and, in severe cases, cardiovascular or pulmonary involvement. Diagnosis relies on clinical criteria, serological markers such as rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibodies, and imaging study.
Key word: RA, ANTI CCP , MRI , MCP, PIP
Introduction – Rheumatoid arthritis (RA) is a chronic inflammatory multisystem disease involving articular and extraarticular tissue, the cause of which is still uncertain. It is characterized by persistent bilateral symmetric arthritis (synovitis) involving the peripheral small joints resulting in cartilage destruction and bony erosions with subsequent joint deformities, hence called deforming arthritis.
Epidemiology -The prevalence of RA is 0.8% of the population (range 0.3 to 2.1%) and sex ratio of women vs men is 3:1. The onset is most frequent during 4th and 5th decades of life
▪ Causes-Genetic factors is an associated of HLA –DR4
▪ Family history
▪ Smoking
▪ Infection like Epstein –barr virus, cytomegalovirus, parvovirus, and rubella virus .
Pathology-The clinical onset – infiltration of the synovial membrane with Lymphocytes, Plasma cells, Dendritic cells , Macrophages. – CD4+ T lymphocytes, including Th1 cells and Th17 cells play a central role by interacting with other cells in the synovium. Lymphoid follicles form within the synovial membrane in which T cell-B cell interactions lead T cells to produce cytokines and B cell produce autoantibodies, including RF and ACPA. interacting with other cells in the synovium. Synovial macrophages – activated by immune complexes – produce proinflammatory cytokines, in Proinflammatory cytokines act( TNF, IL1& IL6) on synovial fibroblasts, to promote Proliferate causing synovial hypertrophy and producing matrix metalloproteinase & proteinase damage to soft tissues and cartilage.
The inflammatory granulation tissue (pannus) formed by the above sequence of events spreads over and under the articular cartilage, which is progressively eroded and destroy.
Clinical features
1.Symmetric joints affection, pain, swelling & tenderness.
2.Morning stiffness – > 30 min. improve with activity
3.Most common joints involved include MCP, PIP, wrists, MTP, ankles, elbows, shoulders, hips, and knees.
4.Sacroiliac and vertebral joints are spared except for C1 to C2.
▪ Characteristic deformities in hands with long-standing uncontrolled disease, including
1.‘swan neck’ deformity
2. boutonnière or ‘button hole’ deformity
3. Z deformity of the thumb
4. Ulnar deviation of the fingers
5. Dorsal subluxation of the ulna at the distal radio ulnar joint is common and may contribute to rupture of the fourth and fifth extensor tendons
6. Triggering of fingers may occur because of nodules in the flexor tendon sheaths.
Extra-articular manifestations
A. Soft tissue involvement around the joints
- Rheumatoid nodules. They are subcutaneous and found in 20% cases. They are often palpable on the extensor surface below the elbows, finger joints and achilles tendon . Patients with nodules are usually seropositive (rheumatoid factor positive).
- Bursitis. The olecranon and other bursa may be swollen.
- Tenosynovitis. It particularly affects the flexor tendons in the palm, causes pain and swelling and may contribute to flexion deformities. Swelling of wrist due to tenosynovitis of extensor tendon sheath is common.
- Muscle wasting.
B. The eye
- Secondary Sjogren’s syndrome. It occurs in 15% case, is characterized by dry eyes , a dry mouth and RA.
- Scleritis and episcleritis. Scleritis or episcleritis may occur, causing painful red eyes. Scleromalacia presents as a bluish discoloration of the sclera around the iris; perforation rarely occurs.
C. The nervous system
- Carpal tunnel syndrome (median nerve compression at wrist). It is common neurological abnormality in RA.
- Atlantoaxial subluxation is a common X-ray finding but cervical cord compression is rare.
- Sensory polyneuropathy producing glove and stocking sensory loss or mononeuritis multiplex due to vasculitis of vasa nervosa.
D. The spleen, lymph nodes and blood
- Palpable lymph nodes usually in the distribution of affected joints are common.
- Spleen. It may be enlarged. Splenomegaly and neutropenia in RA constitute Felty’s Syndrome, and is seen in children. Recurrent infections and leg ulceration are common. Skin pigmentation may be seen.
- Anaemia. normocytic and normochromic.
E. The lungs
- Pleural effusion. This is a common lung finding in RA, occurs particularly in middle-aged men but seldom in women. It may precede the development of arthritis. The fluid has high protein and low sugar content.
- Diffuse fibrosing alveolitis or interstitial lung disease is common.
- Caplan’s syndrome ;-caplan’s syndrome is a combination of rheumatoid arthritis and pneumoconiosis that manifests as intrapulmonary nodules.
F. The Heart pericardial rub
G. The Kidneys
The RA is a common cause of amyloidosis affecting the kidneys. It usually presents with proteinuria, nephrotic. The RA is a common cause of amyloidosis affecting the syndrome and may go on to renal failure. It is due in deposition of highly stable serum amyloid.
Investigation
1.Clinical criteria & symptom based
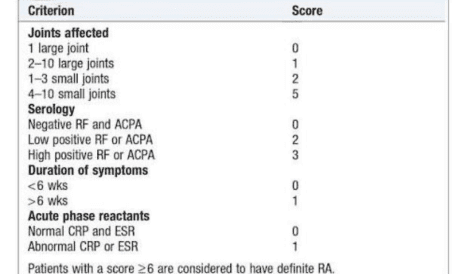
2.Erythrocyte sedimentation rate and C-reactive protein
3.Rheumatoid factor and Anti-cyclic citrulline peptide antibody
4.Ultrasound or MRI
5.X- ray – deformities, decrease bone density .
Miasm -Syphilitic Miasm (Destruction)Most prominent in advanced stages. Associated with joint destruction, deformities, ulcerations, and degenerative changes.
Sycosis (Proliferation and suppression) Seen in the inflammatory phase with swelling, stiffness, overgrowth, and nodules
Homoeopathic Therapeutic
- Bryonia:- Hot swelling of feet. Joints red, swollen, hot, with stitches and tearing; worse on least movement. Every spot is painful on pressure.
- Lithium carb:-Rheumatic pains throughout, the small joints are generally affected. Pain in the hollow of the foot, extending to the knee. Swelling and tenderness of finger and toe joints; better, hot water.
- Actaea spicata:-Rheumatic pains in small joints, wrist , fingers, ankles, toes. Swelling of joints from slight fatigue. Wrist swollen, red, worse any motion. Paralytic weakness in the hands.
- Kalmia latifolia:– A rheumatic remedy. Rheumatism: Pains intense, change places suddenly, going from joint to joint; hot, red, swollen; worse from leást movement.
- Rhododendron:-Acute inflammatory swelling of joints, wandering from one joint to another; severe at night; < in rest and during rough stormy weather. Rheumatic drawing, tearing pains in all the limbs, worse at rest and in wet, cold, windy weather.
- Rhus tox:- Rheumatic pains spread over a large surface at the nape of neck, loin and extremities better motion.
- Stellaria media:-Sharp, shifting, rheumatic pain in all parts very pronounced. Rheumatism; darting pain in almost every part; stiffness of joints; parts sore to touch; worse, motion. Chronic rheumatism. Shifting pains.
- Caulophyllum ;- Severe drawing, erratic pain and stiffness in small joints, fingers, toes, ankles, etc. (rheumatism). Aching in wrists. Cutting pains on closing the hands. Erratic pains, changing place every few minutes.
Co-Author – Dr. Pooja Sharma H.O.D
Dept. of Preventive and Social Medicine
Govt. Homoeopathic Medical College and Hospital Bhopal M.P