ABSTRACT: Homoeopathy is a system of medicine based on individualization and symptom similarity of the patient. It treats every person as a whole and individualised entity. The homoeopathic literature is caring various examples of thyroid diseases and their treatment aspects with homoeopathy. There are numerous examples of clinical and therapeutic studies done on thyroid disorders but there are few peer reviewed controlled design studies in Homoeopathy. Homoepathic medicines play an important role in immuno modulation at the cellular level and can manage cases of hypothyroidism.
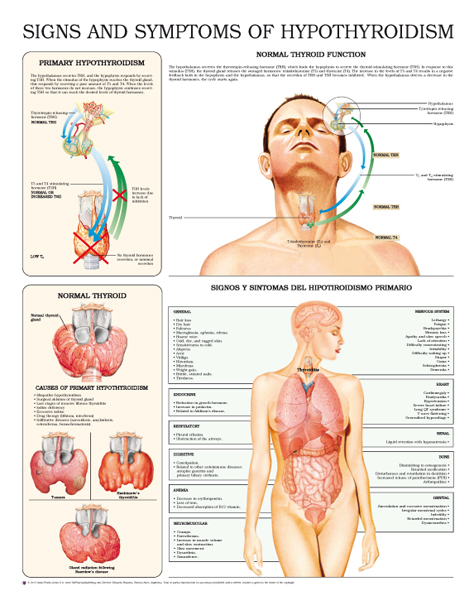
INTRODUCTION: Hypothyroidism is a condition in which the thyroid gland is underactive, resulting in a deficiency of the thyroid hormones triiodothyronine (T3) and thyroxine (T4). In rare cases, hormone production may be sufficient, but thyroid hormones may have insufficient peripheral effects. Hypothyroidism may be congenital or acquired.
ETIOLOGY:
| CONGENITAL HYPOTHYROIDISM | AQUIRED HYPOTHYROIDISM |
| Sporadic (∼ 85% of cases) [3]Thyroid hypoplasia, dysplasia, or ectopyThyroid aplasia (athyroidism)Transplacental transmission of maternal antithyroid antibodiesIodine deficiencyHereditary (∼ 15% of cases)Dyshormonogenetic goiter: Defects in thyroid hormone synthesis (most commonly in thyroid peroxidase) lead to thyroid hyperplasia and goiter.Peripheral resistance to thyroid hormones | Primary hypothyroidism: insufficient thyroid hormone productionHashimoto thyroiditisThe most common cause of hypothyroidism in iodine-sufficient regions Associated with other autoimmune diseases (e.g., vitiligo, pernicious anemia, type 1 diabetes mellitus, and systemic lupus erythematosus)Postpartum thyroiditis (subacute lymphocytic thyroiditis) De Quervain thyroiditis (subacute granulomatous thyroiditis): often subsequent to a flu-like illness Iatrogenic: e.g., post thyroidectomy, radioiodine therapy, antithyroid medication (e.g., amiodarone, lithium)Nutritional (insufficient intake of iodine): the most common cause of hypothyroidism worldwide, particularly in iodine-deficient regionsRiedel thyroiditis: occurs in IgG4-related systemic diseaseWolff-Chaikoff effect Secondary hypothyroidism: pituitary disorders (e.g., pituitary adenoma) → TSH deficiencyTertiary hypothyroidism: hypothalamic disorders → TRH deficiency |
PATHOPHYSIOLOGY:
Hypothalamic-pituitary-thyroid axis
The hypothalamus, anterior pituitary gland, and thyroid gland, together with their respective hormones, comprise a self-regulatory circuit referred to as the “Hypothalamic-pituitary-thyroid axis.
- Primary hypothyroidism: peripheral (thyroid) disorders → T3/T4 are not produced (↓ levels) → compensatory ↑ TSH
- Secondary hypothyroidism: pituitary disorders → ↓ TSH levels → ↓ T3/T4 levels
- Tertiary hypothyroidism: hypothalamic disorders → ↓ TRH levels → ↓ TSH levels → ↓ T3/T4 levels
CLINICAL FEATURES: General signs and symptoms
| Symptoms related to decreased metabolic rate | Symptoms related to generalized myxedema | Symptoms of hyperprolactinemia | Future symptoms |
| Fatigue, decreased physical activity Cold intolerance Decreased sweating Hair loss, brittle nails , and cold, dry skin Weight gain (despite poor appetite) Constipation Bradycardia Hypothyroid myopathy; , myalgia, stiffness, cramps Woltman sign: a delayed relaxation of the deep tendon reflexes, which is commonly seen in patients with hypothyroidism, but can also be associated with advanced age, pregnancy, and diabetes tunnel mellitus. Entrapment syndromes (e.g., carpal syndrome) | Doughy skin texture, puffy appearance Myxedematous heart disease (dilated cardiomyopathy, bradycardia,dyspnea) Hoarse voice, difficulty articulating words Pretibial and periorbital edema Myxedema coma | Abnormal menstrual cycle (esp. secondary amenorrhea; or menorrhagia) Galactorrhea Decreased libido, erectile dysfunction , delayed ejaculation, and infertility in men | Impaired cognition (concentration, memory), somnolence, depression Hypertension Goiter (in Hashimoto thyroiditis) or atrophic thyroid (in atrophic thyroiditis) |
DIAGNOSTICS:
- TSH Levels
| CONGINITAL | AQUIRED |
| Neonatal screening to measure TSH levels 24–48 hours after birth is required by law. Increased TSH levels indicate congenital hypothyroidism. | The initial step is to determine TSH levels, which may be followed by measurement of FT4 levels to confirm or rule out the suspected diagnosis. |
- Antibody testing
- Tg Ab (thyroglobulin) and TPO Ab (thyroid peroxidase): detectable in most patients with autoimmune hypothyroidism
- TRAb(TSH receptors)
- Radioactive iodine uptake test
- Ultrasound of thyroid gland
- Associated conditions
- Hypercholesterolemia (increased LDL), hyperlipidemia, hypoglycemia
- Increased creatine kinase
- Mild anemia
- Possibly hyponatremia
DIFFERENTIAL DIAGNOSIS:
- Euthyroid sick syndrome
- Hashimoto thyroiditis
- Postpartum thyroiditis
- Subacute granulomatous thyroiditis (De Quervain)
- Postpartum thyroiditis
- Congenital hypothyroidism
- Riedel thyroiditis
COMPLICATIONS:
- Myxedema coma
- Primary thyroid lymphoma
- Increased cardiovascular risk
- Carpal tunnel syndrome
HOMOEOPATHIC MEDICINE FOR HYPOTHYROIDISM:
THYROIDINUM: Dry, congested, raw, burning; worse left side Goitre. Excessive obesity. Thyroid produces anemia, emaciation, muscular weakness, sweating, headache, nervous tremor of face and limbs, tingling sensations, paralysis. Heart rate increased, exophthalmus and dilation of pupils. In myoedema and cretinism its effects are striking. Thyroid exercises a general regulating influence over the mechanism of the organs of nutrition, growth and development. Thyroid weakness causes decided craving for large amount of sweets.,
IODIUM: Larynx feels constricted. Eustachian deafness. Thyroid enlarged. Goitre, with sensation of constriction. Swollen submaxillary glands. Uvula swollen.
SPONGIA TOSTA: Thyroid gland swollen. Stitches and dryness. Burning and stinging. Sore throat; worse after eating sweet things. Tickling causes cough. Clears throat constantly.
CALCAREA CARBONICA: Swelling of tonsils and submaxillary glands; stitches on swallowing. Hawking-up of mucus. Difficult swallowing. Goitre. Parotid fistula.
KALIUM IODATUM: It acts prominently on fibrous and connective tissues, producing infiltration, edema, etc. Glandular swellings. Purpura and hemorrhagic diathesis. Syphilis may be indicated in all stages: . Diffused sensitiveness –(glands, scalp, etc).
GRAPHITES: Like all the carbons, this remedy is an anti-psoric of great power, but especially active in patients who are rather stout, of fair complexion, with tendency to skin affections and constipation, fat, chilly, and costive, with delayed menstrual history, take cold easily. -Ophthalmia, with intolerance of artificial light. Eyelids red and swollen. Blepharitis. Dryness of the lids. Eczema of lids; fissured.
DISCUSSION AND CONCLUSION:
Homoeopathy is a system of medicine in which treatment is based on similarity of symptoms. There are many more remedies for hypothyroidism in homoeopathy. With the selection of similar remedy based on totality of symptoms can successfully manage the cases.
About Author:
Dr. Ashok yadav,
HOD Dept. of Practice of Medicine (Hom.) Dr. M.P.K. Homoeopathic Medical College, Hospital and Research Center. Homoeopathy University, Jaipur.
Dr. Navneet Kaur ,,Dr. Mansi Mishra , Dr. Dharmendra Saini , Dr. Sonu Mahiya
REFERENCES
- Harrison T, Kasper D, Hauser S, Jameson J, Fauci A, Longo D et al. Harrison’s principles of internal medicine. 20th ed. New York: McGraw-Hill Education; 2018.
- Robbins, S., Cotran, R., Kumar, V., Abbas, A. and Aster, J., 2015. Pathologic Basis Of Disease. 9th ed. Philadelphia, PA: Saunders Elsevier.
- Ralston, S., Strachan, M., Britton, R., Penman, I. and Hobson, R., 2018. Davidson’s Principles & Practice Of Medicine. 23rd ed. Edinburgh: Elsevier.
- Boericke W., 9th Edition, New Manual of Homoeopathic Materia Medica and Repertory; Augmented, B. Jain Publisher (P) Ltd., New Delhi, (2000).
- Rastogi MV, LaFranchi SH. Congenital hypothyroidism. Orphanet J Rare Dis. 2010; 5 (1). doi: 10.1186/1750-1172-5-17 . | Open in Read by QxMD
- Vanderpump MP. The epidemiology of thyroid disease. Br Med Bull. 2011; 99 (1): p.39-51. doi: 10.1093/bmb/ldr030 . | Open in Read by QxMD
- LaFranchi S. Clinical features and detection of congenital hypothyroidism. In: Post TW, ed. UpToDate. Waltham, MA: UpToDate. https://www.uptodate.com/contents/clinical-features-and-detection-of-congenital-hypothyroidism.Last updated: November 18, 2015. Accessed: January 21, 2017.
- Caturegli P et al.. Hashimoto thyroiditis: Clinical and diagnostic criteria. Autoimmun Rev. 2014; 13 (4-5): p.391-397. doi: 10.1016/j.autrev.2014.01.007 . | Open in Read by QxMD
- Yamada M, Mori M. Mechanisms related to the pathophysiology and management of central hypothyroidism. Nat Clin Pract Endocrinol Metab. 2008; 4 (12): p.683-694. doi: 10.1038/ncpendmet0995 . | Open in Read by QxMD
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease. Elsevier Saunders ; 2015
- Stabouli S, Papakatsika S, Kotsis V. Hypothyroidism and hypertension. Expert Rev of Cardiovasc Ther. 2010; 8 (11): p.1559-1565. doi: 10.1586/erc.10.141 . | Open in Read by QxMD
- Chen Z-P, Hetzel BS. Cretinism revisited. Best Pract Res Clin Endocrinol Metab. 2010; 24 (1): p.39-50. doi: 10.1016/j.beem.2009.08.014 . | Open in Read by QxMD
- Garber JR, Cobin RH, Gharib H, et al. Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Endocr Pract. 2012; 18 (6): p.988-1028. doi: 10.4158/EP12280.GL . | Open in Read by QxMD
- Szczepanek-Parulska E, Hernik A, Ruchała M. Anemia in thyroid diseases. Polish Archives of Internal Medicine. 2017 . doi: 10.20452/pamw.3985 . | Open in Read by QxMD
- Liamis G, Filippatos TD, Liontos A, Elisaf MS. MANAGEMENT OF ENDOCRINE DISEASE: Hypothyroidism-associated hyponatremia: mechanisms, implications and treatment. Eur J Endocrinol. 2016; 176 (1): p.R15-R20. doi: 10.1530/eje-16-0493 . | Open in Read by QxMD
- Refetoff S, Dumitrescu AM, Weiss RE. Impaired sensitivity to thyroid hormone. In: Post TW, ed. UpToDate. Waltham, MA: UpToDate. https://www.uptodate.com/contents/impaired-sensitivity-to-thyroid-hormone?source=search_result&search=thyroid+hormone+resistance&selectedTitle=1~18#H39028860.Last updated: November 29, 2016. Accessed: February 9, 2017.
- Stagnaro-Green A. Postpartum thyroiditis. Best Practice & Research Clinical Endocrinology & Metabolism. 2004; 18 (2): p.303-316. doi: 10.1016/j.beem.2004.03.008 . | Open in Read by QxMD
- Alfadda AA et al.. Subacute Thyroiditis: Clinical Presentation and Long Term Outcome. International Journal of Endocrinology. 2014; 2014 : p.1-7. doi: 10.1155/2014/794943 . | Open in Read by QxMD
- James V. Hennessey. Riedel’s Thyroiditis: A Clinical Review. The Journal of Clinical Endocrinology & Metabolism. 2011; 96 (10): p.3031-3041. doi: 10.1210/jc.2011-0617 . | Open in Read by QxMD
- LaFranchi S. Treatment and prognosis of congenital hypothyroidism. In: Post TW, ed. UpToDate. Waltham, MA: UpToDate. https://www.uptodate.com/contents/treatment-and-prognosis-of-congenital-hypothyroidism?source=search_result&search=congenital+hypothyroidism&selectedTitle=2~88#H2.Last updated: September 20, 2016. Accessed: February 9, 2017.
- Ross DS. Myxedema coma. In: Post TW, ed. UpToDate. Waltham, MA: UpToDate. http://www.uptodate.com/contents/myxedema-coma?source=machineLearning&search=myxedema+coma&selectedTitle=1~22§ionRank=2&anchor=H3#H3.Last updated: June 3, 2015. Accessed: February 9, 2017.
- Beynon J, Akhtar S, Kearney T. Predictors of outcome in myxoedema coma.. Critical Care. 2008 .
- Markus Luster, Leonidas H. Duntas, Leonard Wartofsky. The Thyroid and Its Diseases: A Comprehensive Guide for the Clinician. Springer ; 2019
- Iwasaki Y, Oiso Y, Yamauchi K, Takatsuki K, Kondo K, Hasegawa H, Tomita A. Osmoregulation of plasma vasopressin in myxedema.. The Journal of Clinical Endocrinology and Metabolism. 1990 .
- Piédrola G, Casado JL, López E, Moreno A, Perez-Elías MJ, García-Robles R. Clinical features of adrenal insufficiency in patients with acquired immunodeficiency syndrome.. The Journal of Clinical Endocrinology and Metabolism. 1996 .
- Jacqueline Jonklaas et al.. Guidelines for the Treatment of Hypothyroidism: Prepared by the American Thyroid Association Task Force on Thyroid Hormone Replacement. Thyroid. 2014 .
- R K Pedersen, N T Pedersen. Primary non-Hodgkin’s lymphoma of the thyroid gland: a population based study.. Histopathology. 1996 .
- Shiri R. Hypothyroidism and carpal tunnel syndrome: a meta-analysis. Muscle Nerve. 2014; 50 (6): p.879-883. doi: 10.1002/mus.24453 . | Open in Read by QxMD
- Kothari MJ. Carpal tunnel syndrome: Etiology and epidemiology. In: Post TW, ed. UpToDate. Waltham, MA: UpToDate. http://www.uptodate.com/contents/carpal-tunnel-syndrome-etiology-and-epidemiology?source=search_result&search=carpal+tunnel+syndrome&selectedTitle=3~135#H8.Last updated: February 9, 2016. Accessed: February 9, 2017.
- Braun MM, Barstow CH, Pyzocha NJ. Diagnosis and management of sodium disorders: hyponatremia and hypernatremia. Am Fam Physician. 2015; 91 (5): p.299-307.
- Jameson JL, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J. Harrison’s Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2). McGraw-Hill Education / Medical ; 2018
- Giovanella L, Avram AM, Iakovou I, et al. EANM practice guideline/SNMMI procedure standard for RAIU and thyroid scintigraphy. Eur J Nucl Med Mol Imaging. 2019; 46 (12): p.2514-2525. doi: 10.1007/s00259-019-04472-8 . | Open in Read by QxMD
- Gaitonde DY, Rowley KD, Sweeney LB. Hypothyroidism: an update.. American Family Physician. 2012; 86 (3): p.244-51.
- Sinclair D. Clinical and laboratory aspects of thyroid autoantibodies. Annals of Clinical Biochemistry. 2006; 43 (3): p.173-183. doi: 10.1258/000456306776865043 . | Open in Read by QxMD
- Surks MI, Ortiz E, Daniels GH, et al. Subclinical Thyroid Disease. Journal of the American Medical Association. 2004; 291 (2): p.228. doi: 10.1001/jama.291.2.228 . | Open in Read by QxMD
- Vaidya B, Pearce SHS. Management of hypothyroidism in adults. BMJ. 2008; 337 : p.284-289. doi: 10.1136/bmj.a801 . | Open in Read by QxMD
- Rose SR, Brown RS. Update of Newborn Screening and Therapy for Congenital Hypothyroidism. Pediatrics. 2006; 117 (6): p.2290-2303. doi: 10.1542/peds.2006-0915 . | Open in Read by QxMD
- Kalra S, Sahay R, Unnikrishnan A. The hypoglycemic side of hypothyroidism. Indian Journal of Endocrinology and Metabolism. 2014; 18 (1): p.1-3. doi: 10.4103/2230-8210.126517 . | Open in Read by QxMD
- Hennessey JV, Espaillat R. Diagnosis and Management of Subclinical Hypothyroidism in Elderly Adults: A Review of the Literature. Journal of American Geriatrics Society. 2015; 63 (8): p.1663-1673. doi: 10.1111/jgs.13532 . | Open in Read by QxMD
- Colucci P, Yue CS, Ducharme M, Benvenga S. A Review of the Pharmacokinetics of Levothyroxine for the Treatment of Hypothyroidism.. European endocrinology. 2013; 9 (1): p.40-47. doi: 10.17925/EE.2013.09.01.40 . | Open in Read by QxMD
- Hart JL, Lloyd C, Harvey CJ. Ultrasound of the thyroid. British Journal of Hospital Medicine. 2008; 69 (5): p.68-71. doi: 10.12968/hmed.2008.69.sup5.29373 . | Open in Read by QxMD: