Abstract
Persistent Depressive Disorder is a chronic mood disorder characterized by a persistently depressed mood for most of the day, for more days than not, lasting for at least two years, and associated with additional depressive symptoms causing significant distress or impairment in functioning. Homeopathy emphasizes individualized treatment based on the totality of mental, emotional, and physical symptoms. This case report presents a patient with long-standing depressive symptoms managed through an individualized homeopathic approach. Gradual improvement was observed in mood, sleep, emotional stability, and overall quality of life. The case highlights the potential supportive role of individualized homeopathic management in chronic depressive disorders.
Keywords: Persistent Depressive Disorder, kali-carb, individualisation, similia, Homeopathy, stress.
Introduction
Depression is a mood disorder in which disturbances of mood form the core pathology. It is one of the most common mental disorders and is characterized by persistent sadness, loss of interest or pleasure in previously rewarding activities, guilt, low self esteem, disturbances in circadian rhythm, appetite changes, fatigue, and impaired concentration. These symptoms significantly affect personal, social, and occupational functioning.
According to the National Mental Health Survey of India (2015–2016), nearly 15% of Indian adults require active intervention for one or more mental health conditions, and approximately one in twenty individuals suffers from depression. Persistent Depressive Disorder represents a chronic form of depression requiring long-term and individualized management strategies.
Clinical Features of Depression
The clinical features of depressive disorders include persistent sadness, loss of interest in pleasurable activities, feelings of guilt, worthlessness and hopelessness, fatigue or loss of energy, impaired concentration, appetite and weight changes, psychomotor agitation or retardation, sleep disturbances, and suicidal ideation.
Aetiology
Biological Factors
Genetic predisposition, abnormalities in monoamine neurotransmitter systems (norepinephrine, dopamine, and serotonin), endocrine dysfunction, and association with other medical disorders.
Psychosocial Factors
Loss of significant emotional objects, introjection of loss, fixation at early psychosexual stages, prolonged stress, interpersonal conflicts, and socioeconomic instability.
Case Report
Chief Complaints
A 38 years old Female patient presented with complaints since he past four years, a persistent depressed mood with constant sadness, aggravated in the morning, along with a marked lack of pleasure in previously enjoyable activities. increased irritability over trifles and has poor concentration, which interferes with daily activities and work. Emotionally, she is unable to bear being alone and seeks company, with frequent crying spells even while narrating her complaints. There is also a diminished appetite. Overall, the symptoms show a morning aggravation and have followed a chronic course for the last four years.
Associated Complaints
∙ Breathlessness on slight exertion
∙ Stitching pain in various parts of the body, aggravated at night and relieved after midnight
Past History
∙ Dengue fever six years ago, treated with allopathic medicines
∙ Tubectomy performed eight years ago
Past Psychiatric Treatment
The patient had received psychiatric treatment two years prior for six months (Sertraline 50 mg, Escitalopram 5 mg, and Melatonin 10 mg). Partial improvement was noted, but treatment was discontinued due to financial constraints.
Family History
No family history of depression or other psychiatric disorders.
Father- Hypertension, on Tab. Rosuvastatin 10
Mother- Healthy, Alive
Child- Healthy, Alive
Physical Generals
∙ Appetite: Diminished
∙ Desire: Sweet ++
∙ Thirst: 7–8 glasses/day
∙ Urine: 4–6 times/day
∙ Stool: Once daily, morning
∙ Sleep: Disturbed, non-refreshing
∙ Dreams: Of ghosts
∙ Perspiration: Profuse on covered parts
∙ Diet: Vegetarian
∙ Addiction: Tea
∙ Thermal reaction: Chilly
Menstrual and Obstetric History
∙ Cycle: 30–32 days
∙ Duration: 3–4 days
∙ character: Dark red
∙ Concomitants: Mild nausea before menses; pelvic pain with nausea during menses
∙ Obstetric history: G1P1A0, full-term normal delivery
Mental and Life Space Assessment
Personal and occupational: nurse, wants routine and structured environment conflict: after marriage, difficulty in managing personal and professional life
Mental fatigue with stressed related to household work and college work and unable to manage it all
Sadness without any reason, most of the day
Irritability+++ on trifles and quarrelsome with family members. Guilty after quarrel with anyone.
Does not like to talk but wants company
Excessive anxious thoughts related to her health and hopeless about recovery Fear of death, no suicidal thoughts and attempts.
Weeping when telling her symptoms.
Discontented with everything, feels no one support and understand her emotionally.
Physical Examination
General Examination
Moderately nourished; vitals stable.
Systemic Examination
∙ Respiratory system: Air entry bilaterally equal
∙ Cardiovascular system: Normal heart sounds
∙ Gastrointestinal system: Abdomen soft
∙ Central nervous system: Conscious and oriented
Psychiatric Evaluation
Mental Status Examination
∙ Appearance and behaviour: Well dressed, cooperative, help-seeking ∙ Mood: Depressed and irritable
∙ Affect: Flat
∙ Attention and concentration: Impaired
∙ Memory: Mild impairment of recent memory
∙ Thought process: Relevant with racing ideas
∙ Impulse control: Intact
∙ Judgment and insight: Fair
Psychometric Assessment
Hamilton Depression Rating Scale (HAM-D): Score 12 (mild depression)
Investigations
Complete blood count, Vitamin B12, and thyroid function tests were within normal limits.
Case Evaluation and Totality of Symptoms
Causeless sadness+ >morning+3
Discontented with everything++
Quarrelsome with family members+
Fear of death+
Irritability on trifles++
Weeping when telling her symptoms
Desire for company, aggravated when alone
Diminished Appetite
Dreams of ghost
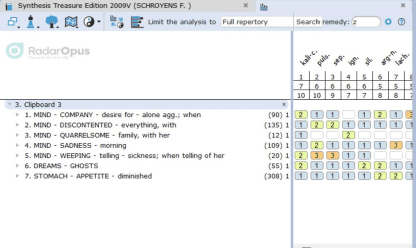
Prescription:
∙ Kali carbonicum 1M – single dose
∙ Sac lac – three times daily for 15 days
Follow-Up and Outcome
Gradual improvement was observed during follow-up visits, including reduction in sadness and irritability, improved sleep and appetite, restoration of interest and motivation, and better emotional stability. medicine repeated for 2 times in 3 months according to symptoms, similarity and outcome. HAM-D score reduced from 12 to 8, indicating clinical improvement.
Conclusion
Persistent Depressive Disorder is a long-standing condition requiring individualized and sustained management. This case report suggests that individualized homeopathic treatment may play a supportive role in improving emotional stability, functional capacity, and quality of life in chronic depressive disorders. Further systematic research is warranted to explore the scope of homeopathy in mental health care. Homeopathic medicine is prescribed as per the similimum, determined through individualization. By administering homeopathic potentized medicines in conjunction with a healthy lifestyle, it is possible to minimize the complaints of patients with Depressive Disorders and help prevent further progression and relapse of the condition.
References
1. Kaplan HI, Sadock BJ, Sadock VA. Synopsis of Psychiatry. 12th ed. Wolters Kluwer.
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 5th ed.
3. National Institute of Mental Health and Neurosciences. National Mental Health Survey of India 2015–2016.
4. Boericke W. Pocket Manual of Homeopathic Materia Medica. 5. Kent JT. Lectures on Homeopathic Materia Medica.