ABSTRACT: Impetigo is the most common bacterial skin infection in children two to five years of age and it is a highly contagious infection of the epidermal layer of skin, most commonly seen especially among children, and transmitted through direct contact. Most common bacteria are Staphylococcus aurens and streptococcus pyogens. The disease is generally mild and felt to be self-limited; however, In conventional medicine therapy antimicrobial treatment is often initiated to reduce spread. Here is a case of impetigo which could be effectively managed by using individualized homoeopathic medicine with proper assessment.
Keywords: Impetigo, Staphylococcus, streptococcus, Cicuta virosa.
Abbreviations: O.P.D. – Outpatient department
INTRODUCTION:
Impetigo is a common and highly contagious superficial bacterial skin infection. The infection is generally classified as bullous and non-bullous based on clinical presentation. Bullous impetigo caused by staphylococcal epidermolytic toxin and non-bullous impetigo which can be caused by either staphylococcus aureus or streptococcus or both together. All ages can contract the infection but non-bullous disease particularly affects young children. Impetigo is most common during hot, humid weather, which facilitates microbial colonization of the skin. It is highly communicable and readily spreads in overcrowding and poor hygiene or through close contact. A widespread form can occur in neonates [1].
EPIDEMIOLOGY:
In the world, impetigo affects more than 162 million children in low to middle income countries. In India, impetigo incidence is 5.96%. Impetigo is more common in developing countries and in poor areas of industrial countries [4].
CLASSIFICATION: There are two ways an initial infection can occur
Primary impetigo – When the bacteria invades the skin through a cut, insect bite or other injury
Secondary impetigo – When the bacteria invades the skin because the skin barrier has been disrupted by another skin infection, such as scabies or eczema. [4]
TYPES:
There are two types of impetigo – Impetigo contagiosa which is also called non-bullous impetigo and bullous impetigo
In non-bullous impetigo, multiple thin walled bullae with erythematous halo, rupture rapidly to form exudative plaques covered with honey-colored (golden) crusts. Spread peripherally, without central healing, removal of crusts reveals erosion. Most frequent site of involvement on face especially periorificial (mouth and nose).
In Bullous impetigo containing turbid fluid and minimal perilesional halo, rupture in few days to form thin, varnish-like crusts. Centre heals to form annular plaques. Face, sometimes extensive lesions, often favoring sites of existing skin diseases. [2]
Investigation done by Gram stains of exudates shows polymorphs with intracellular and extracellular gram-positive cocci in chains (streptococci) or clusters (staphylococci) or both. And Culture of pus to identify etiological agents (Staph. aureus or/ and Strep. Pyogenes) and also for antibiotic sensitivity. [2]
Triggering factors: Varicella infections, herpes zoster infection, scratching, lice, burns, trauma, insect bite
Management: [4]
- Keeping skin clean is the best way to keep it healthy.
- Gently wash the affected areas with mild soap and running water.
- Wash an infected person’s clothes, linen and towels every day and don’t share them with anyone else in the family.
- Cut an infected child’s nail short to prevent damage from scratching.
- It’s important to wash cuts, scrapes, insect bites and other wounds right away.
CASE REPORT
A 3-years-old female child with her mother came with the complaints of eruption on face in OPD with eruption all over face, especially on chin and nose, which are dark brownish honey colored with crust. Sometimes discharge of pus in very little amount. Aggravated by touch and ameliorated by lying on bed. According to the mother, child eats dirt which is indigestible. Patient also complains of worms.
PAST HISTORY – Nothing significant
FAMILY HISTORY – There was no family history
VACCINATION HISTORY – Properly scheduled
PHYSICAL GENERAL: Her appetite was less. She has a desire for indigestible things, thirst was moderate. Bowel movements were regular. Thermal reaction of child was chilly.
General modality: < by touch, > lying on bed
MENTAL GENERAL: Frightened easily and startled at bed time. Act like a foolish behavior.
Physical examination: Small eruptions with dark brown like crust on face especially on chin, nose and eyebrows. Slightly exudates with no itching.
DIAGNOSIS: The diagnosis of the case was made based on symptomatology (ICD-11-1B72) and
physical examination.
Analysis and evaluation of the symptoms with miasmatic analysis [5]
| S. NO. | Symptoms | Analysis | Evaluation | Miasmatic analysis |
| 1. | Frightened easily | Mental general | + | Psora |
| 2. | Foolish behavior | Mental general | +++ | Psora-sycotic |
| 3. | Startled at bed time | Mental general | ++ | Psora |
| 4. | Pus discharge from eruption | Particular | + | sycosis |
| 5. | Honey colored like eruption | Particular | +++ | Sycosis |
| 6. | Impetigo | Particular | +++ | Psora |
| 7. | Crust like eruption | Particular | + | Psora |
| 8. | Worm manifestation | Particular | ++ | Psora tubercular |
| 9. | Dirts desire | Physical general | +++ | Tubercular |
| 10. | > by lying on bed | Physical general | ++ | Psora |
It is mixed-miasmatic case, but psora was the dominant miasm.
Repertorisation: The repertorisation was done using radar opus (synthesis repertory). Cicuta virosa covered maximum rubrics with highest scoring medicine. [6]
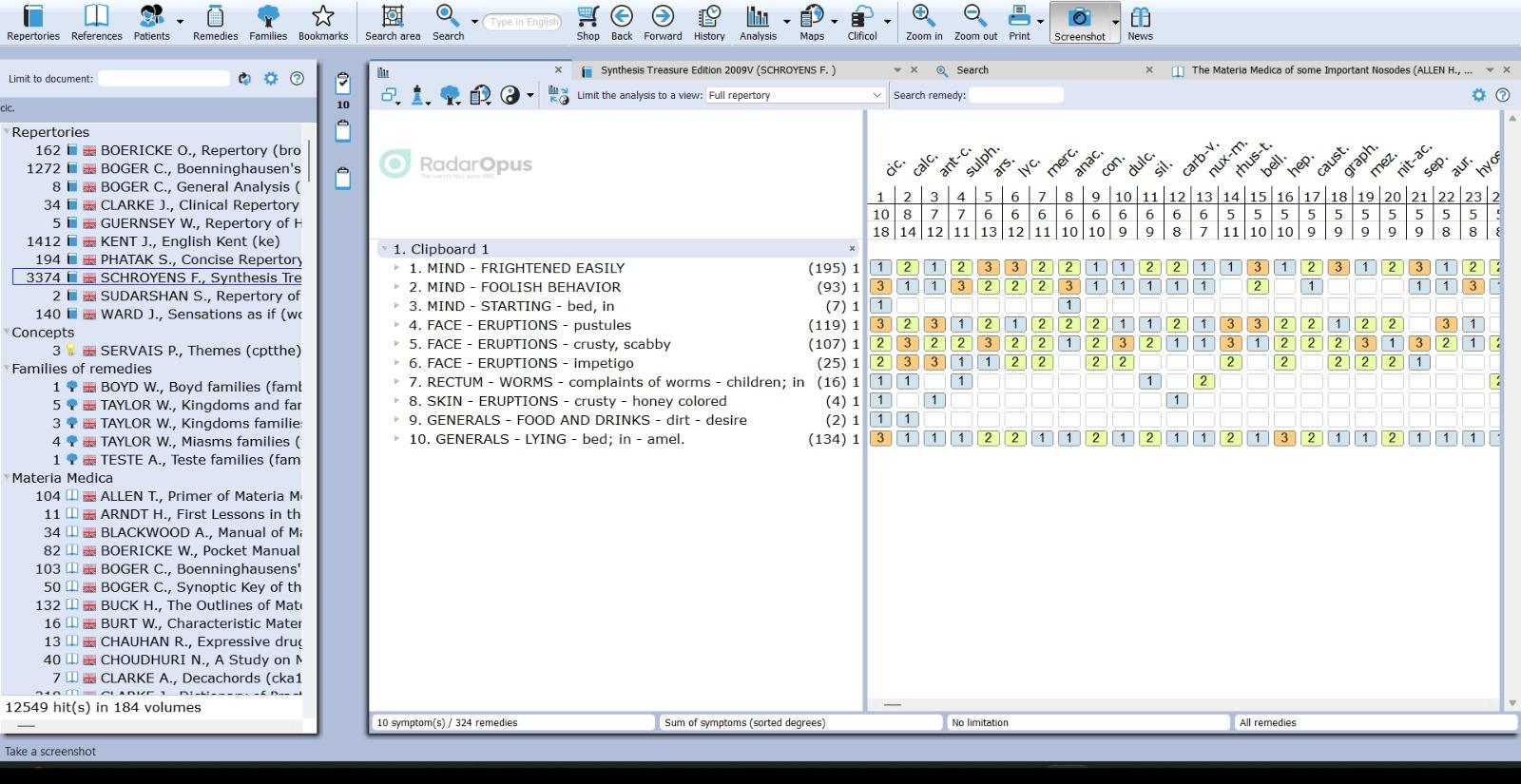
Prescription: After case taking, the Repertorisation was done using Radar opus (synthesis repertory). Here cicuta virosa is selected. So, final selection is done with the help of materia medica [3]. Cicuta virosa 30/4 dose, 4 globules, B.D was prescribed on date 19/07/2023.
FOLLOW UP:
| DATE OF VISIT | CHANGE IN SYMPTOMS | PRESCRIBED MEDICINE/POTENCY |
| 24/07/2023 | Improvement in eruption and no discharge | Rubrum 30/8 dose TDS |
| 28/07/2023 | Improvement continue in eruptions and had no worm manifestation. | Rubrum 30/6 dose BD |
| 05/07/2023 | Better and normal skin appeared | Rubrum 30/6 dose BD |



Before treatment During treatment After treatment
Conclusion: This case report shows the positive role of individualised homoeopathic medicine in the treatment of impetigo within a short span of time. Although this single case report cannot draw any certain conclusion, more cases and scientific research could help to generate evidences on the usefulness of homoeopathic medicine in managing impetigo. Homoeopathic medicines help treat impetigo very effectively by boosting the immune system to fight the infection. Homoeopathy helps bring about natural treatment for impetigo. Homoeopathic system of treatment treats the patient in a holistic way without any side effects.
REFERENCES:
- Walker BR, Colledge NR, Ralston SH, Penman ID, Davidson’s principles and practice of medicine, 22nd edition, Elsevier science limited 2014
- Khanna Neena, Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases. 6th edition, New Delhi, Relix India Pvt. Ltd. 2020.
- Boericke, W. Pocket Manual of Homoeopathic Materia Medica with Repertory (9th edition). B.Jain Publishers (P) LTD; (2015)
- https://www.slideshare.net
- Banerjea Subrata Kumar, Miasmatic Prescribing – Its Philosophy, Diagnostic Classification, Clinical Tips, Miasmatic Repertory, Miasmatic Weightage of Medicines And Case Illustrations. 2nd Extended Indian Ed.8th Impression , New Delhi: B. Jain Publishers (P) Ltd. 2019
- Schroyens F. Radar opus software (synthesis repertory) version 3.2