

ABSTRACT:
Homeopathy is a great method to opt for when people suffer from diabetes mellitus type 2. The purpose of this article is to promote the use of homeopathy to downsize hyperglycemia and manage its associated complications with homeopathy to achieve the targets of glycemic control formulated. Complications associated with DM Type 2 can be magically handled by preventing the patients from progressing to poor control diabetes; and also managing the patient with poor control diabetes with complications (retinopathy, nephropathy, peripheral neuropathy [diabetic ulcer foot], and others).
INTRODUCTION:
Diabetes mellitus is a clinical syndrome characterized by an increase in plasma blood glucose (hyperglycemia). Diabetes mellitus is of two types 1 or type 2 diabetes. Type 1 diabetes is generally considered to result from the autoimmune destruction of insulin-producing cells (β cells) in the pancreas, leading to marked insulin deficiency, whereas type 2 diabetes is characterized by reduced sensitivity to the action of insulin and an inability to produce sufficient insulin to overcome this ‘insulin resistance’. Hyperglycemia causes both acute and long-term problems. Acutely, high glucose and lack of insulin can result in marked symptoms, metabolic decompensation, and hospitalization. Chronic hyperglycemia is responsible for diabetes-specific ‘microvascular’ complications affecting the eyes (retinopathy), kidneys (nephropathy), and feet (neuropathy). (1)
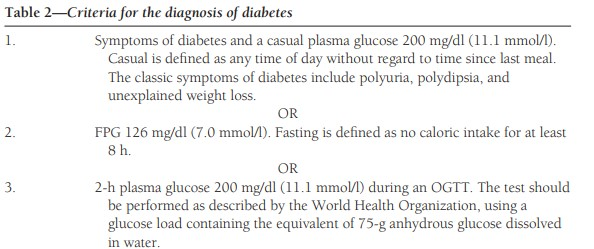
The diagnostic criteria for diabetes –
1. fasting plasma glucose of ≥ 7.0 mmol/L (126 mg/ Dl)
2. Glucose 2 hours after an oral glucose challenge of ≥ 11.1 mmol/L (200 mg/dL) (1).
These values have been selected to identify a degree of hyperglycemia that, if untreated, carries a significant risk of microvascular disease, and in particular diabetic retinopathy (1).
PATHOPHYSIOLOGY OF DIABETES MELLITUS
Insulin resistance and the metabolic syndrome Type 2 diabetes is thought to be caused by resistance to insulin action.
DIABETES MELLITUS INCLUDES CO-MORBIDITIES –
1. HYPERTENSION
2. DYSLIPIDEMIA (Elevated level of LDL cholesterol and triglycerides and low
level of HDL cholesterol)
3. NON-ALCOHOLIC FATTY LIVER DISEASE
4. POLYCYSTIC OVARIAN SYNDROME
This cluster has been termed the ‘insulin resistance syndrome’ or ‘metabolic syndrome’, and is much more common in individuals who are obese.
The primary cause of insulin resistance remains unclear. One theory is centered around the adipocyte; as obesity is a major cause of increased insulin resistance.
Intra-abdominal ‘central’ adipose tissue is metabolically active and releases large quantities of FFAs (free fatty acids), which may induce insulin resistance because they compete with glucose as a fuel supply for oxidation in peripheral tissues such as muscle.
In addition, adipose tissue releases a number of hormones (including a variety of peptides, called ‘adipokines’ because they are structurally similar to immunological ‘cytokines’) that act on specific receptors to influence sensitivity to insulin in other tissues.
Physical activity is another important determinant of insulin sensitivity. Inactivity is associated with the down-regulation of insulin-sensitive kinases and may promote the accumulation of FFAs within skeletal muscle. Sedentary people are therefore more insulin-resistant than active people with the same degree of obesity.
Deposition of fat in the liver is a common association with central obesity and is exacerbated by insulin resistance and/or deficiency. Many people with type 2 diabetes have evidence of fatty infiltration of the liver (non-alcoholic fatty liver disease, NAFLD). This condition may improve with effective treatment of diabetes
In recent years It has been reported that pre-prandial plasma glucose concentrations were related to A1C more strongly than postprandial concentrations (2).
An analysis of a dataset collected in the Diabetes Control and Complications Trial reported that a better correlation with A1C was obtained for post-lunch and mean daily glucose concentrations (2).
However, the research concluded that postprandial glucose levels made the highest contribution (70%) in the lower quintile (A1C <7.3%), i.e., in patients with well-controlled to moderately controlled diabetes (2).
By contrast, fasting hyperglycemia appeared as the main contributor to the overall diurnal hyperglycemia in patients with poorly controlled disease (A1C ≥9.3%) (2)
For all patients who had A1C levels ranging between 7.3 and 9.3%, the contributions of fasting and postprandial hyperglycemia were approximately equivalent (2).
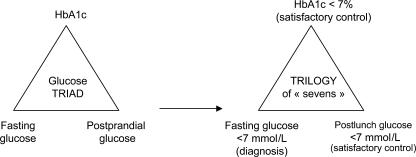
The trilogy of “sevens”
At present, two levels of A1C are usually recognized as threshold values for satisfactory diabetic control: 7% for the American Diabetes Association (3) .
In terms of fasting glucose, recommended goals are set within a 70–130 mg/dl (3.9–7.2 mmol/l) range for American Diabetes (3) .
For postprandial glucose threshold values, large discrepancies are observed. For the American Diabetes Association, the postprandial glycemic threshold value has been set at 180 mg/dl (3).
FACTORS PREDISPOSING DIABETES MELLITUS (3)
- Age 45 years
- Overweight (BMI ≥25 kg/m2)
- Family history of diabetes (i.e., parents or siblings with diabetes)
- Habitual physical inactivity
- Race/Ethnicity
- Previous identified IFG or IGT
- History of GDM or delivery of a baby weighing >9 lbs
- Hypertension (≥140/90 mmHg in adults)
- HDL cholesterol ≤35 mg/dl (0.90 mmol/l) and/or a triglyceride level
≥250 mg/dl (2.82 mmol/l)
- Polycystic ovary syndrome
- History of vascular disease
- History of vascular Disease
GLYCAEMIC GOALS (STANDARDS FOR DIABETIC CARE) (2)
MANAGEMENT OF DIABETES FOR POOR GLYCAEMIC CONTROL
Usually, treatment is done on the basis of an individualized approach but still, there are drugs that can be helpful in managing diabetes.
- There are two Approaches to manage diabetes– (4)
Remedies to manage hyperglycemia
Remedies to manage the complications
# SYZYGIUM JAMBOLANUM- It is the most useful remedy in diabetes mellitus and can be used as a first-line remedy in the treatment of diabetes mellitus. It causes a marked degree of disappearance of glucose in urine. It treats the basic characteristic symptoms of diabetes by polyphagia, polydipsia, and polyuria by normalizing the hyperglycemia. It also treats diabetic ulcers. They are given in mother tincture.
# GYMNEMA SYLVESTRE- After passing urine patient feels very weak. They were burning all over the body. It is given when a patient has diabetic carbuncles.
This is prescribed as a mother tincture.
# URANIUM NITRICUM- It is a great remedy for treating diabetes mellitus and diabetes insipidus. it regulates glycosuria and polyuria and these are the characteristics of this remedy. It is given in females with suppressed menses during diabetes.
# NATRIUM SULPHURICUM- It is given in diabetes mellitus in a person who has a hydrogenoid constitution. There is characteristic burning in the soles and a hot feeling on the top of the head. It is given in patients with polydipsia of cold water.
# PHOSPHORIC ACID- It is a wonderful frug in the management of diabetic mellitus having symptoms of formication over the root of the hair, along the spine, and the limbs. As it is an acid it is definitely indicated in people with marked debility and emaciation with excessive secretion like polyuria at night. Characteristically patients have anxiety before micturition followed by burning and treated with phosphoric acid when a patient has a diabetic ulcer with fetid pus.
# ACETIC ACID- It is a great remedy when the patient has glycosuria when the patient has great debility, polydipsia, and polyuria with pale urine. Given in patients with burning, dry, hot skin with profuse sweat. Characteristic is great thirst with dropsy.
# ARSENICUM BROMATUM- It is a great anti-psoric and anti-syphilitic remedy. It works greatly in diabetes mellitus with diabetic ulcer foot with indurations and also helps in controlling hyperglycemia but is usually thought when the patient is showing syphilitic features of diabetes.
# LYCOPODIUM- It works very efficiently in managing diabetes mellitus with polyuria at night, polyphagia, and debility with uric acid diathesis. Given when a patient has diabetic neuropathy develops numbness. Treats diabetic ulcers with an offensive odor
# PHOSPHORUS- Phosphorus is great in diabetes mellitus in people who have diabetic ulcers which is giving rise to hemorrhages as it is indicated when there are degenerations of skin and mucous membrane. It is also indicated in diabetic neuropathy. Phosphorus is also indicated in diabetic retinopathy causing degeneration of the optic nerve when the vision has flashes and haloes. It also relieves the symptoms of ketoacidosis due to the poor control of diabetes. It is also indicated in burning in different parts of the body.
# HELONIAS DIOICA- It is a wonderful remedy for treating diabetes mellitus and diabetes insipidus. It is a good remedy to be given in diabetes with peripheral neuropathy when a patient has numbness in the lower limb while sitting and a burning sensation on the top of the head.
# ABROMA AUGUSTA- It has wonderful action in diabetes mellitus with polyuria character being a fishy odor of the urine.
Management of complications of diabetes in synthesis repertory- (5)
1. SKIN- ULCERS- diabetic – Secale cornutum, Syzygium jambolanum
2. EYE- INFLAMMATION- Retina- diabetic – Secale cornutum
3. GENERALS- DIABETES MELLITUS- accompanied by- Feet; numbness of- Helonia dioica
4. EXTREMITIES – SWELLING- Ankles- diabetes; in- Argentum metallicum
5. GENERALS- DIABETES MELLITUS- accompanied by- hypertension- Secale cornutum
6. URINE-SUGAR- Helonias dioica, Lycopodium clavatum, Phosphoric acid, Phosphorus, Syzygium jambolanum, Uranium nitricum
7. KIDNEYS- COMPLAINTS Of kidneys- accompanied by- diabetes- sarothamnus scoparius
References
| 1. | Davidson S. Davidson’s Principles and Practice of Medicine. 23rd ed. Stuart H Ralston IDPMWSRPH, editor. New York: Elsevier Ltd; 2018. |
| 2. | Louis Monnier CC. Targets for Glycemic Control. Diabetes Care. 2009 November; 32(2): S199-S204. |
| 3. | ASSOCIATION AD. Standards of Medical Care in Diabetes–2206. Diabetes Care. 2006 JANUARY; 29(1): S4-S42. |
| 4. | Boericke W. Boericke’s New Manual of Homoeopathic MATERIA MEDICA with REPERTORY. third revised edition and Augmented edition based on Ninth edition ed. USA: B. Jain Publisher (P) Ltd; 2016. |
| 5. | Schroyens DF. Repertorium Homeopathicum Syntheticum. 81st ed. London: B. JAIN PUBLISHER (P) LTD; 2001. |



