“From Flare to Clear: Homeopathic Resolution of Guttate Psoriasis with Lycopodium”
ABSTRACT
Guttate psoriasis is an acute eruptive form of psoriasis commonly triggered by infections or stress. Conventional treatment often provides only temporary relief, with frequent relapses. This case report presents a 48-year-old patient diagnosed with guttate psoriasis who was treated successfully with an Individualized Homeopathic prescription of Lycopodium clavatum 200C. Within four weeks, marked improvement was noted in scaling, erythema, and itching, with complete remission by eight weeks. The case highlights the efficacy of Individualized Homeopathic prescribing in managing chronic dermatological conditions.
AIM:
To report a case of guttate psoriasis successfully managed with Individualized Homeopathic treatment using Lycopodium clavatum.
RESULT:
The patient experienced a short phase of Homeopathic aggravation before showing significant improvement within five weeks, with continued progress and no relapse on follow-up.
CONCLUSION:
Individualized Homeopathic treatment with Lycopodium can be effective in managing guttate psoriasis, supporting the principles of constitutional prescribing and holistic care in dermatological disorders.
KEYWORDS:
Guttate Psoriasis, Homeopathy, Lycopodium, Case Report, Individualized Treatment.
INTRODUCTION
Definition
Guttate psoriasis is an acute, eruptive variant of psoriasis characterized by the sudden appearance of numerous small, drop-shaped (guttate) erythematous papules covered with fine, silvery scales, typically following a streptococcal throat infection or other triggering factors. It commonly affects the trunk and proximal extremities and is more frequent in children and young adults, though it can occur at any age.
Etiology and Pathogenesis
Guttate Psoriasis is an acute eruptive variant of psoriasis, commonly triggered by streptococcal infection, particularly of the upper respiratory tract. Other contributing factors include emotional stress, genetic predisposition, trauma, and certain medications.
The condition is immune-mediated, characterized by abnormal T-cell activation and accelerated keratinocyte proliferation, leading to excessive epidermal turnover and inflammatory infiltration in the dermis. Elevated cytokines, especially TNF-α, IL-17, and IL-23, play key roles in the inflammatory cascade.
In Homeopathic understanding, guttate psoriasis represents an imbalance of vital force manifesting through the skin as a psoric expression. The disease may surface following emotional suppression or after infections that disturb the internal harmony of the organism. Individual susceptibility and the patient’s constitutional makeup determine both the form and recurrence of the eruption.
Clinical Features
Onset:
- Sudden appearance of multiple small lesions, often 1–3 weeks after streptococcal throat infection or other triggering factors.
Lesion morphology:
- Small, drop-shaped (guttate) papules or plaques, typically 0.5–1.5 cm in diameter.
- Erythematous base with fine, silvery-white scales on the surface.
Distribution:
- Predominantly on the trunk, upper arms, thighs, and sometimes scalp.
- Face and palms/soles usually spared.
Symptoms:
- Mild to moderate itching and dryness of the skin.
- Occasionally, burning or tightness of the affected area.
Koebner phenomenon:
- New lesions may appear at sites of trauma or scratching.
Course:
- Lesions may coalesce if untreated but typically resolve within weeks to months.
- Recurrences are common after infections, stress, or abrupt corticosteroid withdrawal.
Nail and joint involvement:
- Uncommon in guttate psoriasis (more typical of chronic plaque type).
Systemic features:
- Usually absent, but some patients may report sore throat, malaise, or low-grade fever preceding eruption
DIAGNOSIS
Diagnosis of Guttate Psoriasis is primarily clinical, based on history and the characteristic appearance of lesions.
Diagnostic points:
- Sudden onset of multiple, small, drop-shaped erythematous papules.
- Fine, silvery scales easily detached on gentle scraping.
- Lesions predominantly on trunk and proximal limbs.
- History of recent streptococcal infection (e.g., sore throat or tonsillitis).
- Positive Auspitz sign: pinpoint bleeding spots after scale removal (may be present).
- Koebner phenomenon: new lesions appearing at sites of trauma.
- Supportive lab findings: raised ASO titre or positive throat culture for Streptococcus pyogenes.
- Skin biopsy (if needed) shows parakeratosis, elongation of rete ridges, and Munro microabscesses.
Differential Diagnosis
| Condition | Distinguishing Features |
| Pityriasis rosea | Herald patch followed by oval lesions along cleavage lines; less scaling; self-limiting within 6–8 weeks. |
| Tinea corporis | Annular, ring-shaped lesions with central clearing; positive KOH test for fungal hyphae. |
| Seborrheic dermatitis | Greasy, yellowish scales over scalp, nasolabial folds, and chest; less discrete lesions. |
| Secondary syphilis | Coppery maculopapular rash involving palms and soles; positive VDRL test. |
Investigations
Diagnosis is primarily Clinical, supported by history and appearance of the lesions. However, certain investigations may help confirm or rule out underlying causes:
- Throat swab culture – to detect Streptococcus pyogenes infection.
- Antistreptolysin O (ASO) titre – may be elevated following streptococcal infection.
- Skin biopsy – rarely required but can show parakeratosis, elongated rete ridges, and Munro microabscesses.
- Routine blood tests – to assess inflammatory markers or systemic involvement.
- KOH test (if fungal infection is suspected) – to rule out dermatophytosis.
General Management: Diet and Ancillary Measures
- Dietary Measures
- Eat a balanced diet with plenty of fruits, vegetables, and whole grains.
- Avoid spicy, oily, and processed foods.
- Limit refined sugar, alcohol, and red meat.
- Maintain adequate hydration throughout the day.
- Ancillary Measures
- Engage in regular exercise and get moderate sunlight exposure.
- Practice stress management (yoga, meditation, relaxation).
- Use mild soaps and moisturizers; avoid scratching or friction.
- Ensure adequate rest and emotional stability to aid recovery.
Prognosis
Guttate psoriasis generally has a favorable prognosis. Lesions often resolve within weeks to months, especially after treating the underlying infection or trigger. However, recurrences may occur following stress, infections, or seasonal changes. In some cases, guttate psoriasis may evolve into chronic plaque psoriasis if not properly managed.
Homeopathic Approach
According to Hahnemann’s Organon of Medicine (§7, §17, §26), disease is a dynamic disturbance of the vital force, and cure can be achieved only by a medicine capable of producing a similar derangement in a healthy individual, which is the law of similars.
In this case, the manifestations of guttate psoriasis were viewed as an outward reflection of internal disorder. The totality of characteristic symptoms, physical, mental, and emotional, was evaluated as per §83–§104 (case-taking guidelines), leading to the selection of Lycopodium clavatum as the Similimum.
Following §246, a single dose of Lycopodium 200C was administered, with placebo thereafter, allowing the vital force to react without interference. The gradual, sustained improvement observed aligns with §253, which describes gentle, permanent restoration of health as the hallmark of true cure.
CASE PRESENTATION
PRELIMINARY DATA:
Name: Mr HPC; Age: 48 years; Sex: Male; Religion: Christian; Education: MBA; Occupation: Businessman; Marital status: Married; Address: Deribail, Mangalore; Date of Case: 30/07/25.
CHIEF COMPLAINT:
The patient came with complaints of Skin itching and reddish papular eruptions for two months, which had increased from two weeks. The complaint is aggravated after eating (wheat, eggs, peanuts, curd), Evening and better with a cold-water bath and scratching.
| No. | LOCATION | SENSATION & PATHOLOGY | MODALITIES | CONCOMITANTS |
| 1) | INTEGUMENTARY SYSTEMWHOLE BODYFrom 2 monthsIncreased since 2weeksSudden onset and Gradual progression.Rx>Allopathy (Aprezo 30) | Itching2+ Reddish Papular Eruptions++ (Drop-like) | < Eating: Gluten (wheat)2+,Eggs+, Peanuts+, Curd+.< Evening 2+>Scratching 2+>Cold-water bath+ | _________ |
HISTORY OF CHIEF COMPLAINT:
The patient presented with reddish, papular, drop-like eruptions distributed over the whole body for the past two months, which had increased in intensity during the last two weeks. The onset was sudden, followed by a gradual progression. The lesions were associated with itching of moderate intensity (2+), more pronounced in the evening (2+). The eruptions were aggravated after consumption of gluten (wheat) (2+), eggs (+), peanuts (+), and curd (+), and were ameliorated by scratching (2+) and cold-water bathing (+). The patient had previously taken allopathic medication (Aprezo 30 mg).
PAST HISTORY:
- PAST MEDICAL HISTORY: chickenpox.
- PAST SURGICAL HISTORY: Nothing Significant
- TREATMENT HISTORY: Treatment for the presenting complaint.
- FAMILY HISTORY: Nothing Significant.
- ALLERGIC HISTORY: Not Allergic to Dust or Drugs. Allergic to Eggs, Curd & Peanuts.
PERSONAL HISTORY:
- Diet: Mixed
- Appetite: Good, 3 meals/day
- Thirst: Drinks 1-2 litres/Day.
- Craving: Chicken
- Aversion: Nil
- Bladder habits: 4-5/D. No Difficulty, No Pain while passing
- Bowel habits: Regular once daily; Satisfactory
- Perspiration: Generalized, whole body
- Sleep: Good.
- Dreams: Unremembered
- Addictions: N/S
- Thermal state: Likes monsoon/winter season, wants fan/AC in all seasons, cover in any season till neck, likes open air, bathing in warm water, prefers loose clothing- HOT Patient
LIFE SPACE INVESTIGATION:
The patient was born and raised in Mangalore in a middle-class, nuclear family of three. His father worked abroad in the Gulf, while his mother was a teacher. He is the only child.
Childhood:
His upbringing was described as average. He exhibited an introverted nature and disliked math, feeling that his teacher favored the richer students. He shared a love–hate relationship with his parents. His father was strict and demanding, while his mother, being preoccupied with family issues, was often emotionally distant. The patient recalled feelings of loneliness and, at times, a desire to run away from home.
Education:
During college, the patient’s personality evolved—he excelled academically and in sports, gradually becoming more sociable and balanced. Later, he pursued higher education in Bangalore, where life was stable and satisfying.
Adulthood:
He married at the age of 29. The relationship with his wife was initially strained due to frequent misunderstandings and differing opinions. A miscarriage at five months further affected their emotional bond. After a period of separation, the couple reconciled and had two children, a 17-year-old son and a 12-year-old daughter. Currently, the patient reports feeling disappointed and indifferent toward his wife, describing her as “constantly nagging over trivial matters.” Despite this, he manages household responsibilities, as his wife remains occupied with her own commitments.
Personality:
The patient is philosophical, happy-go-lucky, strong-willed, and prefers solitude. He admits to work-related stress and a tendency to avoid responsibilities. He displays a sense of self-importance and self-love, yet is sympathetic and generally positive in outlook. Intellectually inclined, he reflects deeply on life and maintains a calm demeanor.
Observation: During case taking, the patient was cooperative and communicative. He answered questions thoughtfully and used hand gestures to emphasize points. His responses were concise, relevant, and expressed in a clear, composed tone. At times, he became reflective and philosophical during the discussion.
GENERAL PHYSICAL EXAMINATION:
Appearance: Well-built & Nourished, Brown complexion. Stocky individual.
Orientation: Well-oriented with Time, Place, and Person.
No signs of Pallor, Cyanosis, Clubbing, Icterus, Oedema and Lymphadenopathy.
VITAL SIGNS:
Temperature- Afebrile at the time of examination; Pulse: 82 bpm, Respiratory Rate: 18 bpm, Weight: 97 kgs, Height: 176cm
LOCAL EXAMINATION- Skin
Inspection:
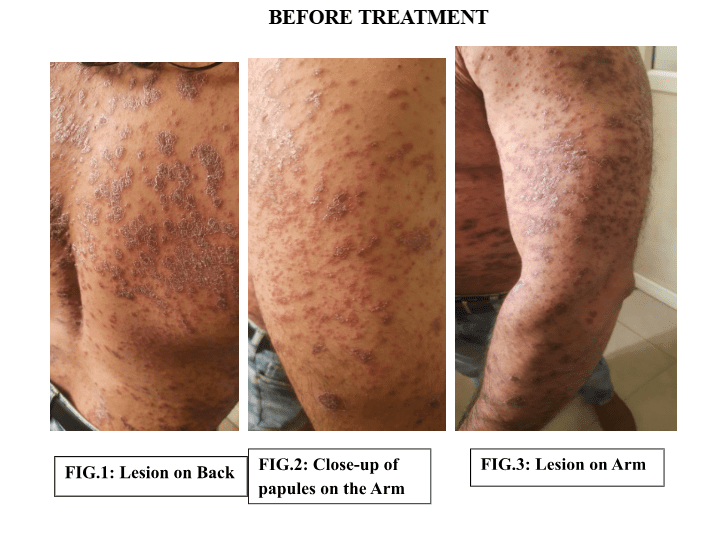
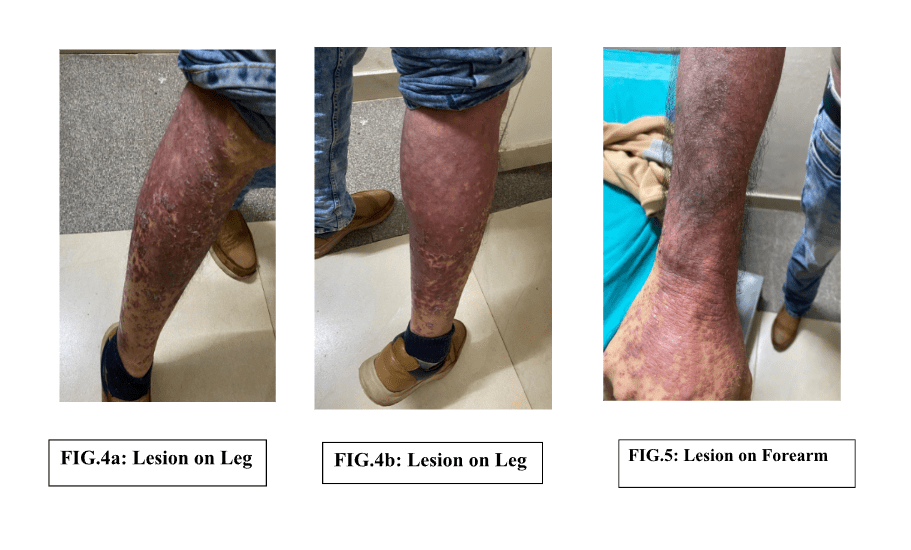
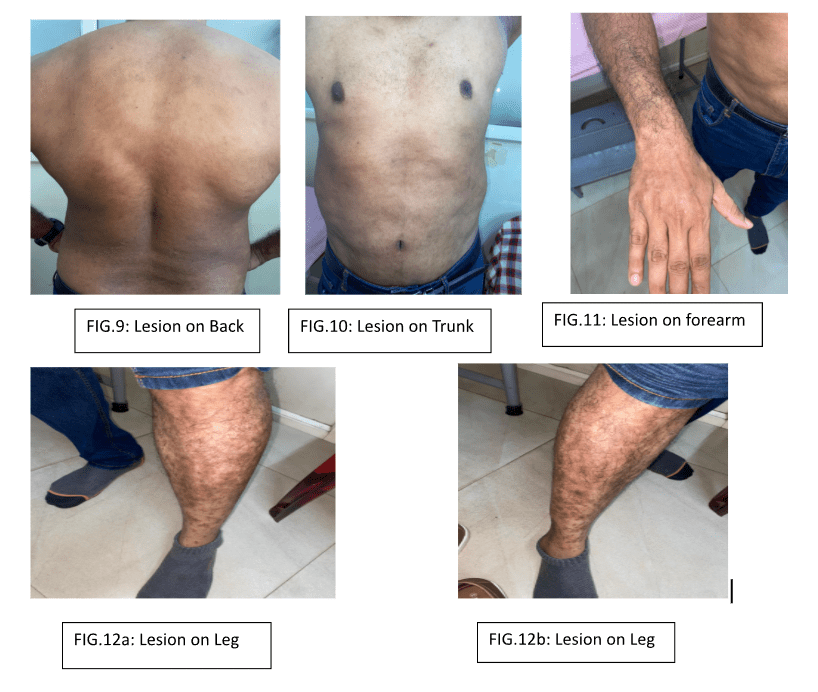
- Multiple discrete, erythematous papules seen over the trunk and proximal limbs.
- Lesions are round to oval, like drops, measuring approximately 0.5–1 cm in diameter.
- Surface covered with fine, silvery-white scales.
- Distribution is symmetrical, predominantly involving the chest, back, arms and legs.
- No oozing, crusting, or ulceration noted.
- No evidence of secondary infection.
Palpation:
- Lesions are dry, rough, and slightly raised.
- Margins are well-defined.
- Non-tender; no local rise of temperature.
- Scales are easily detachable on gentle scraping.
- Auspitz’s sign: Negative.
- No induration or thickening of the underlying skin.
SYSTEMIC EXAMINATION:
Respiratory System: Normal Vesicular Breath Sounds heard, No Added Sounds.
Cardiovascular System–S1 & S2 heard; no murmurs.
DIAGNOSIS:
| Provisional Diagnosis | Differentia Diagnosis |
| Guttate Psoriasis Itching, Reddish, papular eruptions. Evening aggravations.Better by scratching, a cold-water bathScaly, red, small patches like drops | Pityriasis rosea – ruled out due to absence of herald patch and shorter disease course. Nummular eczema – excluded due to absence of oozing, crusting, or marked exudation. Tinea corporis – ruled out by absence of central clearing and negative KOH findings. |
MANAGEMENT- GENERAL
| Diet & Regimen | Ancillary Measure | Education & Orientation |
| Choose oatmeal, brown rice, and whole-grain bread.Limit spicy, fried, and processed foods, along with refined sugar and alcohol.Ensure adequate hydration to maintain healthy skinLimit Trigger Foods: Identify and reduce intake of foods that exacerbate symptoms. | Regular, moderate exercise and early morning sunlight exposure to promote overall health.Gentle skin care with mild soaps and emollients; avoid scratching or friction.Maintain adequate sleep and a structured daily routine to support immunity and mental well-being. | To educate the patient that symptoms are manageable.To set realistic expectations for symptom management- avoid scratching or friction.To be regular for follow-up visits. |
MANAGEMENT- SPECIFIC
| Provisional Remedy | Differential Remedy |
| LYCOPODIUM Does not like to face Responsibilities++Company- Prefers to be alone++Intellectually keen++Keeps a good image of himself++ Desires: Chicken+Thermal: HOT pt++Evening aggravations Itching of the skin. | SULPHURSelfish nature+++Company- desires to be alone++Philosophical ++Thermal: Hot patientSkin: papular eruptions, burning sensation++< heat in general++R/OThe mental symptoms of the patient are more inclined with Lycopodium, be it: intellectual concerns, concern of self-image, better by cold bath, thermally Hot patient is favourable to Lycopodium. Hence, Sulphuris was ruled out. |
Investigations:
No specific laboratory or imaging investigations were undertaken in this case. The diagnosis was made clinically.
Case Analysis- Constitutional Totality
| Mental Generals | Physical Generals | Characteristic Particulars |
-Intellectual++-Prefers to be alone++-Does not like to take up Responsibilities++-Self-love, Self-image ++ | -Craving: Chicken++-Thermally: Hot patient++ | -Itching, reddish papular eruptions on the Trunk and bilateral limbs++-Itching: <curd, <eggs, <peanuts.< evenings++Better by: >cold water bath++ and >scratching++ |
Repertorial Analysis
Repertory used: Synthesis Repertory

Remedy Selection:
Based on the totality of symptoms and individual characteristics, Lycopodium clavatum was selected as the similimum. The prescription was confirmed through repertorial analysis and verified with the Homoeopathic Materia Medica.
FIRST PRESCRIPTION
DATE: 30/07/2025
Rx
- LYCO 200 (1P) H.S. TONIGHT
- 2 GRAIN TABLET (2-2-2) x 2 weeks
- Dose: Single dose, followed by a Placebo
- Basis of selection: Totality and Constitutional Similarity.
FOLLOW-UPS
| DATE | FOLLOW-UP | PRESCIPTION |
| 13/08/2025 | C/ O itching of the whole body- IncreasedC/o scaling of skin- presentC/o reddish papular eruptions- IncreasedC/o new reddish eruptions behind the ear and forehead- from 3-4 daysC/o dryness of the backBowel habit: hard stools for 4 daysAll other generals are good.O/E: reddish eruptions present trunk, bilateral limbs with discolouration.BP: 110/80; Weight: 97.5 kg | RxLYCO (0) 1P EMES2 GRAIN TABLET (2-2-2)5 GRAIN TABLET (1-0-0) EMES x3 WEEKS |
| 03/09/2025 | C/O itching of the whole body- ReducedC/o scaling of skin- presentC/o reddish papular eruptions- presentC/o new reddish eruptions behind the ear and forehead- from 3-4 daysC/o dryness of back- presentBowel habit: didn’t pass todayAll other generals are good.O/E: reddish eruptions present trunk, bilateral limbs with discolouration.BP: 110/80; Weight: 96 kg | RxLYCO (0) 1P EMES2 GRAIN TABLET (2-2-2)5 GRAIN TABLET (1-0-0) EMES X2 WEEKS |
| 17/09/2025 | C/O itching and dryness of the whole body-Better C/o scaling of skin- reduced C/o reddish papular eruptions- betterC/o new reddish eruptions behind the ear and forehead- betterC/o dryness of back- betterBowel habit: betterAll other generals are good.O/E: reddish eruptions present on the trunk, bilateral limbs with discolouration.BP: 110/80; Weight: 95 kg | RxLYCO (0) 1P EMES2 GRAIN TABLET (2-2-2)5 GRAIN TABLET (1-0-0) EMES x3 WEEKS |
| 15/10/2025 | C/O itching and dryness of the whole body-Better C/o scaling of skin- reduced C/o reddish papular eruptions- betterC/o reddish eruptions behind the ear and forehead- Absent C/o dryness- betterSleep is disturbedAll other generals are good.O/E: reddish eruptions present trunk, bilateral limbs with blackish discolouration.BP: 140/90; Weight: 95 kg | RxLYCO (0) 1P EMES2 GRAIN TABLET (2-2-2)5 GRAIN TABLET (1-0-0) EMES x3 WEEKS |
| 05/11/2025 | C/o itching- reducedc/o dryness- reduceddiscolouration of limbs- reduced (80%)No new complaintAll other generals are good.O/E: no new eruptions, discolouration is improvingBP: 130/90; Weight: 95 kg | RxLYCO (0) 1P EMES2 GRAIN TABLET (2-2-2)5 GRAIN TABLET (1-0-0) EMES x2WEEKS |
| 12/12/25 | C/o itching- reducedc/o dryness- reduceddiscolouration of limbs- BetterNo new complaintAll other generals are good.O/E: no new eruptions, discolouration is improvingBP: 120/90; Weight: 95 kg | RxLYCO (0) 1P EMES2 GRAIN TABLET (2-2-2)5 GRAIN TABLET (1-0-0) EMES x2WEEKS |
| 24/12/2025 | C/o eruptions are improving c/o itching slightly present Discolouration of limbs-better No new complaints All generals are goodO/E: no new eruptions, discolouration is improvingBP: 130/90; Weight: 100kg | RxLYCO (0) 1P EMES2 GRAIN TABLET (2-2-2)5 GRAIN TABLET (1-0-0) EMES x2WEEKS |
| 07/01/2026 | C/o eruptions are improving c/o itching slightly present Discolouration of limbs-better No new complaints All generals are good(Reported Case) | RxLYCO (0) 1P EMES2 GRAIN TABLET (2-2-2)5 GRAIN TABLET (1-0-0) EMES x2WEEKS |
DISCUSSION
Despite its Repertorial prominence, Sulphur could not be selected because the patient’s mental profile and modalities conflicted with its Classical picture. The absence of heat aggravation, the presence of cold amelioration, and a reserved, orderly personality clearly ruled out Sulphur.
Thus, Sulphur was not the Similimum in this case.
Justification for Lycopodium clavatum:
The patient demonstrated several hallmark Lycopodium characteristics:
- Intellectual yet introverted personality
Lycopodium types are described as intellectually strong, analytical, yet inwardly insecure and introverted. Clarke notes their “high intellectual activity with aversion to responsibility” (Clarke, Dictionary of Practical Materia Medica). - Aversion to responsibilities and anticipatory anxiety
Lycopodium individuals typically avoid responsibilities, feel overwhelmed, and fear failure. Hering mentions “lack of confidence with fear of undertaking new responsibilities” (Hering’s Guiding Symptoms). - Desire for solitude
Lycopodium often prefers being alone despite its social capability. Boericke describes Lycopodium patients as “preferring solitude, yet not intolerant of company.” - Gastro-intestinal & dietary modalities
Lycopodium exhibits a strong aggravation reaction to certain foods, particularly eggs and fermented substances.
- In Allen’s Encyclopedia: “Eggs aggravate markedly.”
- Lycopodium is also a meat-desiring remedy.
- Skin expression: papular eruptions with evening aggravation
Hering notes “papular eruptions with itching, worse evening, ameliorated by cold.”
This exactly mirrors the patient’s modalities:
- Itching worse in the evening
- Better by scratching and cold bathing
- Papular, red, scattered lesions consistent with guttate psoriasis
The remedy also aligns with the patient’s strong-willed, philosophical nature, which is common in Lycopodium constitutions that hide deep insecurities under an appearance of confidence.
Differential Remedies (Ruling Out)
1. Calcarea carbonica
Ruled-out
- No typical obesity, perspiration on head, cold-damp constitution.
- Patient lacks Calcarea’s characteristic anxiety about health, insecurity, and sluggishness.
- Skin eruptions did not match the typical thick, white, scaly Calcarea type.
- Patient prefers solitude, not Calcarea’s dependence on reassurance.
References: Phatak MM; Boericke; Kent.
2. Sepia
Ruled-out
- Though indifference to family exists, Sepia shows marked irritability, aversion to loved ones, sadness, bearing-down sensations are absent here.
- Sepia has strong hormonal/genital sphere symptoms, not relevant in this case.
- Skin symptoms of Sepia are more ringed, circinate, herpetic, unlike guttate lesions.
References: Kent, Boericke, Clarke.
3. Mercurius solubilis
Ruled-out
- No offensive sweat, salivation, mouth ulcers, or sensitivity to heat & cold, Merc characteristics.
- Merc eruptions are typically moist, suppurative, with burning pains, not dry papular guttate lesions.
- Mental picture (suspicious, hurried, impulsive) not present.
References: Allen, Boericke, Hahnemann Materia Medica Pura.
4. Phosphorus
Ruled-out
- Phosphorus is open, affectionate, extroverted, emotionally expressive, unlike this patient’s introverted, solitary and intellectual nature.
- Marked thirst for cold water, craving for salty/icy foods not seen.
- Skin eruptions of Phos are drier, scaly, and bleed easily, not guttate.
References: Kent, Phatak, Boericke.
5. Pulsatilla
Ruled-out
- Patient is not mild, yielding, emotional, or weepy.
- No desire for open air or aggravation from fatty food.
- Pulsatilla eruptions respond to warmth, but here symptoms improve from cold.
References: Kent, Boericke, Clarke.
6. Rhus toxicodendron
Ruled-out
- Rhus tox eruptions are intensely itchy vesicles, better from warmth and hot bathing, opposite to this case.
- Characteristic restlessness, stiffness < rest, > motion not seen.
- Lesions are not the typical erythematous vesicular pattern.
References: Allen, Boericke.
7. Nux vomica
Ruled-out
- Nux vomica’s personality is irritable, impatient, competitive, sensitive to noise/light, unlike patient’s philosophical, calm, solitary nature.
- Desires stimulants (coffee, alcohol, spicy food), not present here.
- Skin complaints in Nux are usually urticarial, not guttate.
References: Kent, Boericke, Hering’s Guiding Symptoms.
LIMITATIONS
- This report is based on a single clinical observation; therefore, the findings cannot be generalized to a larger population.
- Objective diagnostic tools such as dermoscopy or histopathological confirmation were not employed to document internal changes.
- Assessment of improvement was primarily based on visible and subjective parameters rather than quantitative scoring systems.
SUGGESTIONS
- Further clinical studies and case series with larger sample sizes are recommended to validate the role of Lycopodium clavatum in psoriasis management.
- Incorporating standardized dermatological scoring systems and objective follow-up imaging could strengthen the evidence base.
- Comparative studies between individualized Homeopathic treatment and conventional therapy may help establish the integrative potential of Homeopathy in dermatological care
CONCLUSION
This case demonstrates the effectiveness of Individualized Homeopathic treatment in managing guttate psoriasis. A single dose of Lycopodium clavatum 200C produced significant and sustained improvement, highlighting the power of constitutional prescribing in restoring systemic balance and promoting holistic healing.
CONSENT
Written informed consent was obtained from the patient for publication of this case report
BEFORE TREATMENT
MID TREATMENT
AFTER TREATMENT
Guided by: Professor Dr Mini I.V.
REFRENCES
- Guttate psoriasis. MedlinePlus Medical Encyclopedia. U.S. National Library of Medicine. Available from: https://medlineplus.gov/ency/article/000822.htm
- Thomas J. Textbook of Psoriasis. Jaypee Brothers Medical Publishers; 1st ed. 2016. ISBN 978-9352501656.
- Weinberg J, Lebwohl M (eds). Advances in Psoriasis: A Multisystemic Guide. Springer Cham; 2021. ISBN 978-3-030-54858-2.
- Annu Kanwar — “Plaque Psoriasis Successfully Treated with an Individualised Homoeopathic Medicine Lycopodium: A Case Report”.
- Boericke W. Pocket Manual of Homoeopathic Materia Medica. 9th ed. New Delhi: B. Jain Publishers; 2007.
- Allen T F. A Handbook of Materia Medica and Homoeopathic Therapeutics. F E Boericke; 1889.
- Hering C. Materia medica. Boericke & Tafel; 1873.
- Boger CM. A Synoptic Key to the Materia Medica:(a Treatise for Homoeopathic Students). Jain Publishers; 2003.
- Kent JT. Lectures on Homoeopathic Materia Medica. New Delhi: B. Jain Publishers; 2002.
- Phatak SR. Materia Medica of Homoeopathic Medicines. New Delhi: B. Jain Publishers; 1999.
- Murphy Robin ND. Lotus Materia medica 1400 homoeopathic and herbal remedies.
- Hahnemann S. Organon of Medicine. 6th ed. Translated by William Boericke. New Delhi: B. Jain Publishers; 2011.
- Schroyens F, editor. Synthesis Repertory: Edition 9.1. New Delhi: B. Jain Publishers; 2004.