Abstract
Dysmenorrhoea—painful menstruation—is more than a monthly discomfort; it also reflects a deeper constitution. Conventional therapy provides symptomatic relief of pain but may cause side effects. Homoeopathy offers a holistic approach aimed at addressing the internal expression of disease as well as the pain itself. This article reviews the classification, clinical features, and homoeopathic management of dysmenorrhoea, highlighting key remedies and a detailed case report.
Introduction
Dysmenorrhoea affects 50–70 % of menstruating women worldwide. While typically defined by pelvic pain, it is increasingly understood as a multidimensional condition— physical, hormonal, and psychological. It is divided into:
• Primary dysmenorrhoea: Cramping pelvic pain without detectable pathology, usually beginning soon after a menarche.
• Secondary dysmenorrhoea: Pain associated with pelvic disorders such as endometriosis, pelvic inflammatory disease, or uterine fibroids.
Risk factors
Include early menarche, heavy menstrual bleeding, smoking, and emotional stress.
Pathophysiology
High prostaglandin levels in the endometrium trigger strong uterine contractions, reduced uterine blood flow, and ischemic pain. In secondary dysmenorrhoea, structural abnormalities such as endometriotic implants or fibroids contribute to the symptoms.
Homoeopathic Perspective
Homoeopathy views dysmenorrhoea as a manifestation on of an outward expression of internal imbalance—an outward sign of the patient’s constitutional state. Treatment is based on the totality of symptoms: patient`s physical, mental, and emotional state. Acute remedies offer relief during menses, while constitutional prescriptions aim to restore long-term balance.
Key Remedies
Magnesia phosphorica: Lightning like pain, coming and going, Paroxysmal cramping pain, better from warmth and firm pressure; often right-sided. Menses early; flow dark stringy; pain ameliorate when flow begins.
Cimicifuga racemosa: Neuralgic pains radiating to back or thighs; associated mental restlessness or gloom. Menses irregular; exhausting; delayed or suppressed by mental emotion, from cold, from fever, with hysteria. Mental symptoms increased during menses.
Colocynthis: Intense colicky pain forcing the patient to bend double; with restlessness; relief from hard pressure or heat. Affection from anger and indignation.
Pulsatilla: Delayed or scanty menses with changeable flow; gentle, tearful temperament; relief in open air. Never been well since puberty; thirstlessness.
Belladonna: Sudden, throbbing pain with a sense of pelvic congestion; flushed face and heat.
Chamomilla: Severe pain with extreme irritability and oversensitivity; dark clotted flow; pain with numbness of affected part.
Caulophyllum: Pain violent, intermittent, paroxysmal, spasmodic. Late menses; flow little, labour like pain fly to the breast.
Viburnum opulus: Colicky, spasmodic pain in pelvic organs. Pain at sacrum and pubes with anterior muscle of thigh; from back to loin to womb. Menses too late, scanty, las ng few hours.
Xanthoxylum: Neuralgic dysmenorrhea, pain in loins and lower abdomen; worse left side, extending to thigh, along the Genito-crural nerve. Menses too early, thick, almost black in neurasthenic patients.
Management Plan
1. Acute phase: Select a remedy according to the characteristic pain modalities and accompanying general symptoms.
2. Constitutional treatment: After acute relief, prescribe a deeper constitutional remedy to correct underlying susceptibility.
3. Supportive measures: Encourage balanced diet, hydration, regular exercise, and stress-reduction practices.
Case study (Dated on 23 June 2025)
A 24-year-old female patient working at finance came with the complain of intolerable pain during menstruation with dizziness and fainting episodes. Pain located on lower abdomen, lower back and anterior of thigh; crampy in nature; ameliorated by warm application and bending double.
Menstrual history:
Menarche: 12 years of age
LMP: 21 June 2025
Duration: 5 days / 25-26 days
Character: Dark; clots present, stain linen brown
Before menses: Desire- panipuri, lower back pain
During menses: back and abdominal and thigh pain, weakness – unable to get up and do daily activity
After menses: No significant complain
No leucorrhoea
Effect of complain on patient: she has to has take rest and unable to do daily activity due to severe pain.
Physical general
Appetite: Poor
Desire: Spicy food, added spices, panipuri
Aversion: Vegetable (only eats potato and ladyfinger) Thirst: Adequate; 2 lit/day, prefer cold water
Urine: No complain, frequency- 6-7 me/day
Stool: Frequent cons pa on with hard stool
Perspiration: Moderate, on axilla, face
Sleep: Sound; position- sideway
Dreams: Forgets
Thermal: Hot
Past history
Jaundice
Malaria
Piles with bleeding
Family history
Parents – No major illness
G. Mother – HTN
Patient as a person
Patient working in back office- table and chair mode, is shy in nature, she doesn’t talk much and she doesn’t initiate conversation as she thinks that what will be my impression in other`s mind and no desire to go outside in a crowd or group of people. She has had one best friend since her school time.
Quiet disposition.
Sensitive- get emotional when watching someone cry, in sad movies, and when someone reproaches her.
The patient prefers to be alone.
She loves animals like turtles- she had a pair of them but they died. Now she has love birds- she is very attached to them.
School life- Majorly she was worried before exams and has stage fright.
She gets angry when things don’t go according to what she has planned, but she can adjust.
She loves drawing.
Totality of the case
1. Shy, quiet, mild in nature
2. Introverted- don’t share easily
3. Sensitive to emotions
4. Stage fright before exams
5. Menstrua on complains
6. Menses staining linen- difficult wash off
7. Menses painful with fainting spells
8. Desire spices
9. Aversion to vegetables
Repertorization:
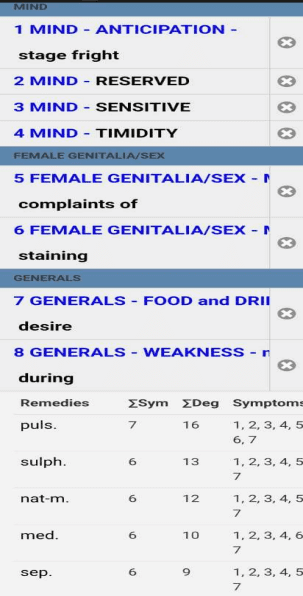
Basis of Prescription
After case taking, analysis and repertorization, Individualized Homoeopathic medicine Pulsatilla 200 three doses with placebo twice a day for 7 days.
Follow ups
18 July 2025 – First day of menses, Moderate flow, pain better and can do her daily activity, weakness improved, Had mild per rectal bleed from piles before 7 days.
Prescription- Placebo 30 BD for 3 days
13 August 2025 – First day of menses, Pain decreased further, Flow moderate, No weakness
Prescription- Placebo 30 BD for 3 days
9 September 2025 – Afternoon– Menses came too early, Profuse Bleeding of dark colour with large clots with generalised weakness with pain in hypogastrium better by bending double.
Prescription – On the Basis of acute Totality Cinchona off 200 five drops in half cup water every 1 hour for 3 hours
9 September 2025 Evening – Bleeding decreased, clots decreased.
15 September 2025 – Pulsatilla 200 three doses repeated
3 October 2025 – First day of menses, mild pain in hypogastrium, flow moderate, no weakness.
Prescription: SL 200 bd for 7 days
4 November 2025 – LMP: 28 oct 2025. Bleeding moderate, pain tolerable, can-do daily activity
Prescription: SL 200 bd for 7 days
27 December 2025 – LMP: 18 dec 2025. Pain better than last cycle.
Prescription: SL 200 bd for 7 days
Discussion
Homoeopathy addresses both symptom relief and the deeper constitutional imbalance. Evidence and clinical observation suggest that properly selected remedies can reduce prostaglandin overproduction, improve uterine tone, and provide lasting relief.
Conclusion
Dysmenorrhoea is more than a physical ailment; it reflects the individual’s inner state. Homoeopathy, through careful
individualisation, offers a safe, effective, and holistic path to healing, making it a valuable option in women’s healthcare.
References
1. Dutta DC. Textbook of Gynaecology, 9th ed. New Delhi: Jaypee Brothers Medical Publishers; 2018.
2. Allen HC. Keynotes and Characteristics with Comparisons. New Delhi: B. Jain Publishers.
3. Boericke W. Pocket Manual of Homoeopathic Materia Medica. New Delhi: B. Jain Publishers.
4. Phatak SR. Materia Medica of Homoeopathic Medicine. 2nd ed.: B. Jain; 1999.