
Dependence, Addiction, Withdrawal: Alcohol & Homoeopathy
Abstract-
Dependence, addiction, and withdrawal are critical components in understanding substance use disorders. Addiction is often characterized by three key elements: compulsive use, loss of control, and continued use despite adverse consequences. These elements highlight the severe impact substances can have on an individual’s behaviour and health. The World Health Organization’s ICD-10 outlines specific criteria for diagnosing dependence, which include a strong desire to use the substance, difficulties in controlling use, the presence of withdrawal symptoms, and the development of tolerance.
Alcohol dependence, in particular, illustrates the complex interaction between psychological and physical dependence. Symptoms of alcohol withdrawal can range from mild discomfort to severe conditions such as delirium tremens, which require immediate medical intervention. Relapse remains a significant challenge in the treatment of addiction, often triggered by stress, exposure to alcohol-related cues, or the consumption of small amounts of alcohol. Effective management of withdrawal involves a combination of pharmacological and psychosocial interventions, with benzodiazepines being a primary treatment option. Additionally, the “Trans-theoretical” model of behaviour change emphasizes the importance of understanding the stages of recovery and the potential for relapse. While homeopathic remedies may offer supportive care in managing cravings and withdrawal symptoms, they should be used as a complement to, rather than a replacement for, conventional medical treatments.
Keywords- Addiction, Dependence, Withdrawal, Alcohol, Alcohol, Substance use, Complications, Homoeopathic approach.
Abbreviations- ICD – International Classification of Disease, AWS- Alcohol Withdrawal Syndrome, CNS- Central Nervous System, GABA-A – GABA-alpha, NMDA – N-methyl-D-aspartate.
Introduction–
Understanding what is Dependence, addiction and withdrawal?
The primary elements of adductive- 3 C’s
- Compulsive Use- compulsive urges, repetitive ritualistic behaviours, and intrusive, ego – dystonic thoughts
- Loss Of Control- The inability to limit or resist inner urges makes it very difficult to stop without outside help, marking a pivotal point in addiction. While an individual may manage to abstain or control use temporarily, they inevitably return to compulsive, uncontrollable use.
- Continued Use Despite Adverse Consequences- Substance use persists despite escalating issues such as deteriorating health, embarrassment, humiliation, shame, and growing family, financial, and legal problems.
Diagnostic guidelines for Dependence Syndrome in ICD- 10 (WHO,1992) :
A definite Diagnosis of Dependence made only if three or more of following have been present in last year:
- A strong desire or sense of compulsion to take the substance.
- Difficulties in controlling substance-taking behaviour in terms of its onset, termination, or level of uses.
- A physiological withdrawal state occurs when substance use is stopped or reduced, indicated by characteristic withdrawal syndrome or the use of a similar substance to relieve or avoid withdrawal syndrome.
- Evidence of tolerance- increased doses of substance required in order to achieve desired effects produced in low dose.
- Progressive neglect of alternative pleasurable activities.
- Persisting with substance use despite clear evidence of harmful consequences.
Two types of dependence- 1. Psychological 2. Physical
Psychological dependence involves an impaired ability to control drug use.
Physical dependence is characterized by the development of tolerance and withdrawal symptoms when substance use is stopped.
There are several alcohol dependence typologies. Two most popular ones with their phenotypic characters are:-
By JELLINEK, 1960
Alpha: indicating a purely psychological dependence without loss of control or inability to abstain.
Beta: physical complications without any physical or psychological dependence
Gamma: acquired tissue tolerance, adaptive cell metabolism, physical dependence, and loss of control
Delta: shares the first three characteristics of gamma, but inability to abstain replaces loss of control.
Epsilon: dipsomania or periodic alcoholism.
By CLONINGER ET AL. 1981; SIGVARDSSON ET AL. 1996
| Type 1 alcoholism | Type 2 alcoholism |
| Age of onset above 25 years | Teenage age of onset {under 25 years} |
| No Family history of alcohol | Family history of alcohol present |
| Loss of control (or psychological dependence) | Inability to abstain or stop |
| Guilt and fear about dependence | Aggressive behaviour |
| Harm avoidance | Novelty- seeking personality traits |
| Rewards dependence |
Risk factors favouring use of substance use-
- Community norms favourable towards alcohol use.
- Perceived availability of alcohol.
- Poor family management.
- Family history of substance use.
- Parental attitudes favourable to alcohol use.
- Favourable attitudes toward antisocial behaviour.
- Friend’s alcohol use.
- Sensation seeking
- Antisocial behaviour
Alcohol dependence–
The development of alcohol dependence is a complex and dynamic process influenced by numerous neurobiological and environmental factors that affect the motivation to drink (Grant 1995; Samson and Hodge 1996; Vengeliene et al. 2008; Weiss 2005). An individual’s propensity to consume alcohol at any given time is thought to reflect a balance between alcohol’s positive reinforcing effects, such as euphoria and anxiety reduction (anxiolysis), and its aversive effects, which are typically associated with negative consequences like hangovers or withdrawal symptoms. Memories of these rewarding and aversive qualities, along with learned associations between these internal states and related environmental stimuli or contexts, influence both the initiation and regulation of alcohol intake. These experiential factors, combined with biological, environmental, and social influences, shape expectations about the consequences of alcohol use, which in turn affect an individual’s decision to engage in drinking behaviour.
The stage of addiction, whether it’s the initial experience with alcohol, early problem drinking, or later excessive consumption leading to dependence, significantly impacts the progression of alcohol abuse. While many individuals abuse alcohol without becoming dependent, persistent excessive consumption can result in dependence. Neuroadaptive changes from ongoing alcohol use and abuse, such as tolerance and physiological dependence, are key factors in the shift from controlled alcohol use to more frequent, excessive, and uncontrollable drinking (Koob and Le Moal 2008). The fear of withdrawal symptoms upon attempting to quit or reduce drinking can strongly contribute to the continuation of alcohol use and abuse.
Withdrawal
When an individual who is dependent on alcohol suddenly stops or significantly reduces their alcohol intake, they experience a characteristic withdrawal syndrome. Typically, alcohol suppresses central nervous system (CNS) activity. Similar to other CNS depressants, the withdrawal symptoms that occur after chronic alcohol use cessation are the opposite of the effects of intoxication.
Typical clinical features of alcohol withdrawal include the following
- Signs of heightened autonomic nervous system activation, like rapid heartbeat (i.e., tachycardia), elevated blood pressure, excessive sweating (i.e., diaphoresis), and shaking (i.e., tremor);
- Increase activity of the CNS (i.e., CNS hyper-excitability) that may present in motor seizures; and
- Hallucinations and delirium tremens in the most severe form of withdrawal..
In addition to physical withdrawal symptoms, a range of symptoms that contribute to distress and psychological discomfort are a significant part of the withdrawal syndrome (Anton and Becker 1995; Roelofs 1985; Schuckit et al. 1998). These symptoms include emotional changes such as irritability, agitation, anxiety, and dysphoria, along with sleep disturbances, an inability to experience pleasure (anhedonia), and frequent complaints of “achiness,” which may indicate a lowered pain threshold. Many of these symptoms, including those reflecting a negative affect state (e.g., anxiety, distress, and anhedonia), have also been observed in animal studies using various models of dependence.
Alcohol withdrawal syndrome (AWS) is a collection of signs and symptoms that usually begins in alcohol-dependent individuals within 6–24 hours after their last drink. AWS can occur unintentionally if abstinence is imposed by illness or injury, or intentionally if the person voluntarily stops drinking due to an alcohol-related illness or as a step towards achieving and maintaining abstinence.{3}
Relapse:
Relapse can be defined as the return to alcohol consumption after a prolonged period of abstinence. Clinically, the vulnerability to relapse is often linked to an intense craving or desire to drink. Events that strongly trigger relapse typically fall into three categories: exposure to small amounts of alcohol (alcohol-induced priming), exposure to alcohol-related cues or environmental contexts, and stress.
Pathophysiology
Alcohol withdrawal syndrome is driven by various mechanisms. The brain maintains a neurochemical balance using inhibitory and excitatory neurotransmitters. The primary inhibitory neurotransmitter is γ-aminobutyric acid (GABA), which operates through the GABA-alpha (GABA-A) receptor. One of the key excitatory neurotransmitters is glutamate, which functions through the N-methyl-D-aspartate (NMDA) receptor..
Alcohol amplifies the effect of GABA on GABA-A receptors, leading to reduced overall brain excitability. Prolonged exposure to alcohol causes a compensatory decrease in the GABA-A receptor’s response to GABA, which is demonstrated by an increased tolerance to the effects of alcohol.
Alcohol inhibits NMDA receptors, and chronic exposure leads to an up-regulation of these receptors. When alcohol consumption is suddenly stopped, the previously inhibited receptors are no longer suppressed, resulting in brain hyper-excitability. This hyper-excitability clinically manifests as anxiety, irritability, agitation, and tremors, with severe cases leading to alcohol withdrawal seizures and delirium tremens.
Diagnostic Criteria for Alcohol Withdrawal
| A. Cessation of / or reduction in alcohol use that has been heavy and prolonged. | |
| B. Two (or more) of the following, developing within several hours to a few days after criterion A: | |
| 1. Autonomic hyperactivity (for e.g., sweating or pulse rate more than 100 beats per minute) | |
| 2. Increased tremors | |
| 3. Insomnia | |
| 4. Nausea & vomiting | |
| 5. Transient visual, tactile, or auditory hallucinations or illusions | |
| 6. Psychomotor agitation | |
| 7. Anxiety | |
| 8. Grand mal seizures | |
| C. The symptoms in criterion (B) cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. | |
| D. The symptoms are not due to a general medical condition and are not better accounted for by another mental disorder. | |
Adapted with permission from American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed., text revision. Washington, D.C.: American Psychiatric Association, 2000:216.
A key concept in both alcohol craving and withdrawal is the “kindling” phenomenon, which refers to long-term changes in neurons following repeated detoxifications. It is believed that recurrent detoxifications heighten obsessive thoughts and alcohol cravings. Kindling explains why each subsequent episode of alcohol withdrawal tends to become progressively more severe.. Although the significance of kindling in alcohol withdrawal is debated, this phenomenon might influence the choice of medications for treatment. If certain medications can reduce the kindling effect, they may be preferred options for managing withdrawal.
Symptoms of Alcohol Withdrawal Syndrome
| Symptoms | Time of appearance after cessation of alcohol use |
| Minor withdrawal symptoms: insomnia, tremulousness, mild anxiety, gastrointestinal upset, headache, diaphoresis, palpitations, anorexia | 6 to 12 hours |
| Alcoholic hallucinosis: visual, auditory, or tactile hallucinations | 12 to 24 hours* |
| Withdrawal seizures: generalized tonic-clonic seizures | 24 to 48 hours† |
| Alcohol withdrawal delirium (delirium tremens): hallucinations (predominantly visual), disorientation, tachycardia, hypertension, low-grade fever, agitation, diaphoresis | 48 to 72 hours‡ |
*— Symptoms generally resolve within 48 hours.
†— Symptoms reported as early as two hours after cessation.
‡— Symptoms peak at five days.
Differential Diagnosis
Alcohol withdrawal syndrome can be mistaken for other conditions. Thyrotoxicosis, anticholinergic drug poisoning, and amphetamine or cocaine use can lead to increased sympathetic activity and altered mental status. Central nervous system infections or hemorrhages can cause seizures and changes in mental status. Withdrawal from other sedative-hypnotic agents can produce symptoms similar to those of alcohol withdrawal syndrome.
Goals of Treatment
The American Society of Addiction Medicine outlines three immediate goals for the detoxification of alcohol and other substances:
(1) “To ensure a safe withdrawal from the dependent drug(s) and help the patient achieve a drug-free state”;
(2) “To ensure a humane withdrawal process that preserves the patient’s dignity”;
(3) “To prepare the patient for continued treatment of their dependence on alcohol or other drug”
Management:
General Care
Abnormalities in fluid, electrolyte, or nutrition levels should be corrected. In patients experiencing severe withdrawal, intravenous fluids may be necessary due to excessive fluid loss from hyperthermia, sweating, and vomiting. However, intravenous fluids should not be routinely given to patients with less severe withdrawal, as they may become overhydrated..
Pharmacologic Treatment of Withdrawal
Benzodiazepines , Adjunctive Agents- Haloperidol (Haldol) , atenolol (Tenormin) in conjunction with oxazepam, Clonidine (Catapres) , phenytoin (Dilantin). Iazepam (Valium), lorazepam (Ativan), chlordiazepoxide (Librium, clorazepate (Tranxeme) and phenobarbital.
Detoxification
Pharmacologic therapies are recommended for patients with addictive disorders to prevent life-threatening withdrawal complications such as seizures and delirium tremens, and to improve adherence to psychosocial addiction treatments. Laboratory testing is necessary to determine the type and timing of drugs used addictively and to guide the management of withdrawal and recovery.
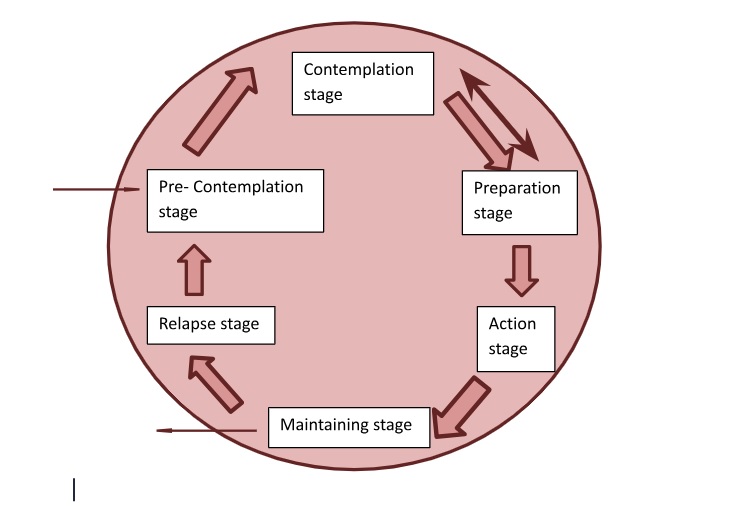
Model of overcoming Addiction- Also known as “Trans-theoretical” Model-
- Pre-contemplation- Denial or not even considering change of addiction habit.
- Contemplation- Realise & want to change but cannot commit.
- Preparation- Initiate to prepare to make behavioural change, change by shifting and adjusting on micro level with help of self-control or doctor/ therapy (patches use etc)
- Action- making active choices, attending OPD treatment, counselling, group meetings.
- Maintenance stage- continues practicing the habits to maintain long term recovery. There’s always the risk of relapse.
- Relapse stage- when a person restarts the consumption of substance and the whole process starts again.
Homoeopathic Approach-
Angelica Atropurpurea– Produces aversion to alcohol as disgust. Addresses atony of various organs, dyspepsia, nervous headaches, and chronic bronchitis to enhance expectoration.
Asarum Europaeum – Craving for alcoholic beverages. A medication for nervous disorders, fatigue, and excessive irritability. Constantly feels cold.
Avena Sativa – Insomnia, especially in alcoholics; adverse effects of morphine addiction. Excessive indulgence in sexual activities leading to mental depression and physical exhaustion.
Bufo – Induces a desire for intoxicating drinks and causes impotence. Affects the nervous system and skin, often linked to sexual dysfunction.
Kola / Sterculia Acuminata – A remedy for reducing alcohol cravings and drinking habits. Enhances appetite and digestion. Increases endurance for prolonged physical exertion without food and without experiencing fatigue. Effective for neurasthenia. Acts as a tonic to regulate circulation, cardiac rhythm, and as an antidiarrheal.
Quercus Glandium Spiritus / Quercus-E-Glandibus – Counteracts the effects of alcohol and reduces the craving for it; administered in low doses for several months. Treats chronic spleen and liver conditions. Diarrhoea often occurs for a time when using it.
Strophanthus Hispidus – Gradually reduces the craving for alcoholic spirits slowly but surely. Treats heart conditions such as mitral regurgitation, arteriosclerosis, and weak, rapid, and irregular heart action due to muscular debility.
Strychninum Nitricum – said to reduce alcohol cravings with weeks of use.
Sulphuric Acid – desire for alcohol. Water produces coldness in the stomach and must be mixed with liquors. Very relaxed feeling in my stomach.
Reference–
- World health Organisation, The ICD-10 classification of Mental and Behavioural Disorders – Clinical Descriptions and Diagnostic Guidelines. AITBS Indian ed. Delhi, India. AITBS Publishers & Distributors; 2007
- Becker HC. Alcohol dependence, withdrawal, and relapse. Alcohol Res Health. 2008;31(4):348-361.
- Hall W, Zador D. The alcohol withdrawal syndrome. The Lancet. 1997 Jun 28;349(9069):1897-900.
- Bayard M, Mcintyre J, Hill KR, Jack Woodside JR. Alcohol withdrawal syndrome. American family physician. 2004 Mar 15;69(6):1443-50.
- Miller NS, Gold MS. Management of withdrawal syndromes and relapse prevention in drug and alcohol dependence. American family physician. 1998 Jul 1;58(1):139-46.
- Prochaska JO, Prochaska JM, How TT, Action M. 23 Transtheoretical Model. Lifestyle Medicine. 2024 Aug 29:251.
- Boericke W. Boericke’s New Manual of Homoeopathic Materia Medica with Repertory. 3rd revised & augmented ed. 9th ed. New Delhi, India: B. Jain Publishers Pvt Ltd; 2015.
- Abuse S. Clinical Subtyping for Alcohol Use Disorders. Oxford Textbook of Psychopathology. 2008 Nov 20:280.
Authors-
Dr. Ashok Yadav, Professor, Department of Practice of Medicine, Dr. M.P.K. Homoeopathic Medical College, Hospital & Research Centre, Homoeopathy University, Jaipur, Rajasthan, India
Dr. Virendra Chauhan, Associate Professor, Department of Practice of Medicine, Dr. M.P.K. Homoeopathic Medical College, Hospital & Research Centre, Homoeopathy University, Jaipur, Rajasthan, India
Dr. Mansi Saini, MD scholar, Department of Practice of Medicine, Dr. M.P.K. Homoeopathic Medical College, Hospital & Research Centre, Homoeopathy University, Jaipur, Rajasthan, India
Dr. Yashaswi Choudhary, MD scholar, Department of Practice of Medicine, Dr. M.P.K. Homoeopathic Medical College, Hospital & Research Centre, Homoeopathy University, Jaipur, Rajasthan, India
Dr. Hemlata Kumawat, MD scholar, Department of Practice of Medicine, Dr. M.P.K. Homoeopathic Medical College, Hospital & Research Centre, Homoeopathy University, Jaipur, Rajasthan, India

