ABSTRACT
Introduction: Benign prostatic hyperplasia, (BPH) is a common condition as men get older. Enlarged prostate glands can cause uncomfortable urinary symptoms, such as blocking the flow of urine out of the bladder.
Objective: To study the components of IPSS for effective individualized homoeopathic medicine and Sabal serrulata Ø in cases of BPH.
Material and Methods: 30 patients (n= 30) of BPH of NCR-Delhi area, were selected and divided into two groups one group of 15 patients were given individualized medicines on the basis of subjective and objective symptoms in each case as per the law of similia and prescribed singly. Another group of 15 (n=15) patients was treated with ‘Sabal serrulata Ø’. Data was recorded and computed for the components of international prostate symptom score like incomplete emptying, frequency, intermittency, urgency, weak stream, straining and nocturia.)
Results: The treatment provided using ‘Sabal serrulata Ø’ and ‘individualised medicines’ had a significant improvement in patients. The symptoms changed to the desirable category (up to < half the time) was considered, the improvement ranged from 33.3% (nocturia) to 73.3% (intermittency). The number of total patients in the desired category ranged from 33.3% (weak stream) to 100.0% (straining). It was being observed that the components of international prostate symptom score had improved after the administration of homoeopathic medications as compared to before the trial. On overall basis, in twenty-six (86.7%) patients there was marked improvement in IPSS BPH.
Conclusion: Paired t-test showed that the treatment provided using ‘Sabal serrulata Ø’ and individualised homoeopathic treatment had significant improvement in patients.
KEYWORDS: benign
prostatic hyperplasia (BPH), homoeopathy, International Prostate Symptom Score
(IPSS), paired t-test, Sabal serrulata Ø.
ABBREVIATIONS: benign prostatic hyperplasia (BPH), International Prostate Symptom Score (IPSS), prostate specific antigen (PSA), outpatient department (OPD), incomplete emptying (IE) frequency (F), intermittency (I), urgency (U), weak stream (WS), straining (S), nocturia (N).
Introduction
About 105 million are affected globally by benign prostatic hyperplasia (BPH)1.The prostate (prostata; prostate gland) is an organ linked inextricably with the endocrine system. The main role of the prostate as a male reproductive organ is to produce prostatic fluid, which accounts to 30 per cent of the semen volume. Sperm motility and nourishment are aided by the prostatic fluid constituents and the environment they create. Prostatic fluid is a thin, milky alkaline fluid containing citric acid, calcium, zinc, acid phosphatase and fibrinolysin among its many constituents. Prostate specific antigen (PSA) is also a constituent found in prostatic secretions.
Benign prostatic hyperplasia condition prevalence increases markedly with age and it is most common condition in men especially over 50 years of age. BPH is rarely life-threatening but often affects the individual’s quality of life of the patient in varying degrees in similar ways as other chronic diseases such as diabetes mellitus, hypertension, and heart disease2,3.The symptoms of hesitancy in urinary flow, poor urinary stream, intermittent urinary stream, dribbling of urine, incomplete emptying of bladder, episodes of near retention of urine increased frequency, nocturia, urgency, urge incontinence, and nocturnal incontinence may be observed in patients with benign hypertrophy of prostate.
Numerous studies have been done to investigate the efficacy of homoeopathic medicine in cases of BPH. It has been observed that despite of limitations, there is increasingly clear evidence that Sabal serrulata extract along with homoeopathic simillimum based on symptom totality exerts beneficial effects by improving a number of urological symptoms and flow measures in cases of benign hypertrophy of prostate.
Objective of the present investigation was to study the components of IPSS for effective individualised homoeopathic medicine and Sabal serrulata Ø in cases of BPH.
Material and Methods
A randomised controlled trial was conducted on patients suffering from BPH of Delhi National Capital Region, OPDs of Bakson Homeopathic Medical College and Hospital, Greater Noida. A sample size of 30 patients was selected on the basis of random sampling method. The patients were screened in the outpatient departments of respective centres and as per the inclusion and exclusion criteria, and were enrolled and followed up for six months of the trial.
Study design was conducted in two randomly allocated groups, the ‘individualised medicine’ (group 1) intervention group and the ‘Sabal serrulata Ø’ (group 2) intervention group. On the basis of the symptoms with intension of the investigator was to cure the patients. A prospective randomised control single blind trial was performed to study the efficacy if individualised homoeopathic medicine selected on the basis of symptom totality over organ specific ‘Sabal serrulata Ø’ in cases of BPH.
Group I (individualised homoeopathic intervention)
Medicines in this group of patients were selected on the basis of subjective and objective symptoms in each case. The totality of symptoms is taken for prescription and the symptoms of each individual patient are taken as a whole.
The homoeopathic medicines were selected as per the law of similia and prescribed singly at one occasion. Detailed case taking, its recording and interpretation of the symptoms was done in standard case record. The symptoms were classified and evaluated to erect the totality. Help of repertorisation was taken as and when required. Cases were either repertorised by conventional repertories (Kent’s Repertory, Boger Boenninghausen’s Characteristic Repertory) or modern repertories (Synthesis Repertory, Murphy’s Homeopathic Repertory). Constitutional prescriptions were based on the totality formed by analysing and evaluating the mental generals, physical generals, characteristic particulars, and miasm.
The potency selection and repetition of doses was done according to the susceptibility of every individual case. The medicines were prescribed in accordance with instruction in Hahnemann’s sixth edition of Organon of Medicine.
Group II: ‘Sabal serrulata Ø’ intervention
The symptoms of each patient were studied in detail and every patient of this group was prescribed ‘Sabal serrulata Ø’ on the basis of its established value as an organopathic medicine in cases of BPH and administered in tincture form. Patients were instructed to take 10 drops of the ‘Sabal serrulata Ø’ in half cup of water three times a day
One group of 15 patients was prescribed ‘Sabal serrulata Ø’ and other group of 15 patients was prescribed medicines on the basis of symptom totality obtained from a complete and detailed case taking. Ignatia amara (2), Conium maculatum (2), Causticum (1), Medorrhinum (1), Selenium metallicum (1), Sulphur (2), Baryta carbonicum (2), Pulsatilla nigricans (1) and Lycopodium clavatum (2) were used. All the medicines were obtained by the researcher from the pharmacy of Bakson Homeopathic Medical College and Hospital, Greater Noida to avoid any unforeseen variation in the preparation of medicines by different medicine company.
Data recording and analysis
Patients were reviewed regularly during follow ups as per the requirement of the case. Majority of the patients were reviewed, during the follow ups on a fortnightly basis to assess the subjective and objective symptoms. Each case was followed for a minimum of six-months from the commencement of treatment was analysed according to follow-up criteria to elicit the prognosis of the treatment. Aggravations, amelioration, no change, disappearance of chief complaints, improvement in generals of the patient are emergence of new outcome assessment criteria.
International Prostate Symptom Score (IPSS)
The international prostate symptom score (IPSS) (1992) by the American Urological Association (AUA) adopted by the World Health Organization as the IPSS was used in the study. An additional 8th question on quality of life (QOL) was added later on4. The components of IPSS like incomplete emptying (IE) frequency (F), intermittency (I), urgency (U), weak stream (WS), straining (S) and nocturia (N) were also studied and understood through paired t-test.
The responses of the BPH patients at the hospital towards the Personal Data Schedule, IPSS (before the start of the experiment) and IPSS (at the end of experiment) were quantified. The statistical test t-test helped the researcher to find the significance of the treatment. The paired t-test were computed to test the significance of differences between IPSS (before the treatment) and IPSS (after the treatment) of the patients as well as for treatment by ‘Sabal serrulata Ø’ and other specific medicines in combination with ‘Sabal serrulata Ø’ to BPH patients.
Results and discussion
Study of treatment effects using ‘Sabal serrulata Ø’ and ‘individualised medicines’
Out of 30 patients, 15 patients were given ‘Sabal serrulata Ø’ and 15 were given medicines that were individually selected for them after detailed case taking and study of the totality of symptoms by the process of individualisation. The significant paired t-test values showed that the treatment provided by researcher using ‘Sabal serrulata Ø’ and ‘individualised medicines’ had a significant improvement in patients (Table 1). According to W. Boericke’s Pocket Manual of Homoeopathic Materia Medica and Repertory, ‘Sabal serrulata’ mother tincture has unquestioned value in cases of prostatic enlargement5. In a study on ‘Sabal serrulata’ mother tincture showed the reduction of prostate tumour xenograft size significantly in an in vivo trial6. Moreover, ‘Sabal serrulata’ decreased PC-3 cell proliferation and DU-145 cell proliferation.
On looking at the components of IPSS score, i.e. showed significant improvement in both ‘Sabal serrulata Ø’ and ‘individualised medicines’, however if computed over both the treatments than paired t-test was non-significant in all the IPSS components (table 1). Hence, we also conclude that paired t-test should be separately computed for different treatments.
Table 1: Effect of treatment by Sabal serrulata Ø and individualised medicines using paired t- values on the components of IPSS
| Character | Sabal serrulata Ø (Total Patients: 15) | Individualized Medicines (Total Patients: 15) | Over treatment (Total Patients: 30) |
| IE | 18.873** | 25.051** | 1.155ns |
| F | 11.374** | 17.576** | 0.615ns |
| I | 18.699** | 15.984** | 1.314ns |
| U | 7.897** | 25.200** | 0.901ns |
| WS | 33.500** | 75.093** | 1.420ns |
| S | 4.961** | 1.520** | 0.583ns |
| N | 8.290** | 16.897** | 0.742ns |
Note: IE: Incomplete emptying; F: Frequency; I: Intermittency; U: Urgency; WS: Weak Stream; S: Straining; N: Nocturia
Components of IPSS before and after the experiment
IPSS was computed from its components like, incomplete emptying, frequency, intermittency, urgency, weak stream, straining and nocturia. The details of these are studies indicating number of patients before and after the experimentation. In our study, there was desired improvement in the symptoms for the components of the IPSS score. When the change in symptoms was considered, the change in the desirable category (up to < half the time) was considered, the improvement ranged from 33.3% (nocturia) to 73.3% (intermittency) (table 2). On the other hand, it was important to look into the number of patients in desired category (up to < half the time) of components of IPSS score symptoms. The number of total patients in the desired category ranged from 33.3% (weak stream) to 100.0% (straining) (table 2).
Table 2: Status of the patients with desired level of symptoms for the components of IPSS (BPH) before and after the treatment of BPH.
| Status of patient | Components of IPSS for BPH | |||||||
| IE | F | I | U | WS | S | N | ||
| Not at all | Before | 0 | 0 | 0 | 0 | 0 | 1 | 3 |
| After | 1 | 5 | 0 | 1 | 0 | 6 | 13 | |
| Change | 1 | 5 | 0 | 1 | 0 | 5 | 10 | |
| <1 in 5 times | Before | 0 | 8 | 0 | 3 | 0 | 5 | 11 |
| After | 1 | 16 | 4 | 9 | 1 | 15 | 11 | |
| Change | 1 | 8 | 4 | 6 | 1 | 10 | 0 | |
| <Half the time | Before | 3 | 14 | 1 | 8 | 0 | 9 | 9 |
| After | 14 | 6 | 10 | 12 | 9 | 9 | 4 | |
| Change | 11 | -8 | 9 | 4 | 9 | 0 | -5 | |
| About half the time | Before | 9 | 8 | 2 | 10 | 0 | 10 | 2 |
| After | 9 | 3 | 11 | 7 | 11 | 0 | 0 | |
| Change | 0 | -5 | 9 | -3 | 11 | -10 | -2 | |
| More than half the time | Before | 9 | 0 | 14 | 6 | 12 | 5 | 3 |
| After | 4 | 0 | 5 | 1 | 8 | 0 | 2 | |
| Change | -5 | 0 | -9 | -5 | -4 | -5 | -1 | |
| Almost Always | Before | 9 | 0 | 13 | 3 | 18 | 0 | 2 |
| After | 2 | 0 | 0 | 0 | 1 | 0 | 0 | |
| Change | -7 | 0 | -13 | -3 | -17 | 0 | -2 | |
| Patients (%) with improved symptoms | (After-Before) | 13 (43.3%) | 13 (43.3%) | 22 (73.3%) | 11 (36.7%) | 21 (70.0%) | 15 (50.0%) | 10 (33.3%) |
| Total (%) patients with desirable symptoms after the treatment | Sum of desired symptoms (< half the time) | 16 (53.3%) | 27 (90.0%) | 14 (46.7%) | 22 (73.3%) | 10 (33.3%) | 30 (100.0%) | 28 (93.3%) |
Note: IE: Incomplete emptying; F: Frequency; I: Intermittency; U: Urgency; WS: Weak Stream; S: Straining; N: Nocturia; Before: Before the start of treatment; After: After 5-6 months of treatment; Change: Change in symptoms
Incomplete emptying
The patients were asked “how often have you had the sensation of not empting your bladder?”. The grading of the sensation of incomplete emptying of the urinary bladder was done for the entire sample within the IPSS into grades 5 to 0 which were: almost always, more than half the time, about half the time, less than half the time, less than 1 in 5 times and not at all. The data was collected before and after the trial and is represented in table 2.It can be observed from table before the trial a greater number of patients reported having the sensation of incomplete emptying of the bladder about half the time, more than half the time and almost always. Whereas, after the completion of trial a greater number of patients reported the sensation of incomplete emptying of bladder was less than half the time. Thus this showed improvement with the respective homoeopathic medicines. ‘Sabal serrulata’ is known for its anti-inflammatory activity, anti-androgen properties, anti-oedema effects, and spasmolytic and smooth muscle relaxant activity7. It is used as an herbal medicine to treat a variety of conditions, including chronic pelvic pain, bladder and urinary disorders, and hormone imbalances8.
Frequency
The grading of the frequency to urinate in less than every 2 hours was done for the entire sample within the IPSS into grades 5 to 0 which were: almost always, more than half the time, about half the time, less than half the time, less than 1 in 5 times and not at all. The data was collected before and after the trial for all the patients and is represented in table 2.It can be observed that the frequency of urination in less than every 2 hours in the patients was higher before the trial and a large number of patients had reported increased frequency of urination, with 14 out of 30 patients under study reporting to have the need to urinate in less than every 2 hours to be less than half the time. In the post trail representation it can be observed that 16 out of 30 patients reported having the need to pass urine every 2 hours to be less than 1 in 5 times. The increased frequency of urination due to BPH can be observed to have decreased after the administration of homoeopathic medication.
Intermittency
The grading of the intermittency of urine was done for the entire sample within the IPSS. The patients were asked if they found that while urinating they stopped and started again several times to urinate and the severity of the symptom was given grades from 5 to 0 which were: almost always, more than half the time, about half the time, less than half the time , less than 1 in 5 times and not at all. The data was collected before and after the trial and is represented in Table 2.
It can be observed from the figure that the symptom of intermittency was reported as almost always or more than half the time by nearly all the patients before the trial. The complaint of intermittency improved with the administration of the homoeopathic medication and the after the trail most of the patients reported to have a decrease in the intermittency of urine to about half the times or even less.
Urgency
The grading of the urgency to pass urine was done for the entire sample within the IPSS. The patients were asked “How often they found it difficult to postpone urination” and the severity of the symptom was given grades from 5 to 0 which were: almost always, more than half the time, about half the time, less than half the time , less than 1 in 5 times and not at all. The data was collected before and after the trial and is represented in table 2.It can be observed that the urgency to urinate has decreased after the administration of homoeopathic medications as compared to before the trial.
Weak stream
The grading of the weakness urinary stream was done for the entire sample within the IPSS. The sequelae of BPH include a decreased urinary flow and advancing voiding and storage symptoms; these may eventually result in acute or chronic urinary retention9. The patients were asked to report how often they had a weak urinary stream and their symptom were graded from 5 to 0 which were: almost always, more than half the time, about half the time, less than half the time , less than 1 in 5 times and not at all. The data was collected before and after the trial and is represented in table 2.
It can be observed that all patients reported a weak urinary stream either always or more than half the time. In the data collected after the trial it was observed that almost all patients experienced an improved flow of urine after administration of homoeopathic medications. Thus this showed the high efficacy of homoeopathic medications. BPH patients with bladder outflow obstruction complaint of initial increased detrusor contractility in the compensatory phase with normal bladder emptying10,11. Prolonged obstruction to urine outflow results in detrusor hypertrophy and bladder wall thickening, ultimately culminating in detrusor underactivity and emptying failure11,12.
Straining
The grading of the need for straining to start urination was done for the entire sample within the international prostate symptom score (IPSS). The patients were asked to report how often they had to strain to start urination and their symptom were graded from 5 to 0 which were: almost always, more than half the time, about half the time, less than half the time, less than 1 in 5 times and not at all. The data was collected before and after the trial and is represented in table 2.A decrease in need to strain in an increased number of patients was observed after the homoeopathic medications were used and data collected post the trial.
Nocturia
The number of times a patient needs to urinate at night was recorded for the entire sample population before and after the trail as a component of the IPSS. The symptom were graded from 5 to 0 which were: almost always, more than half the time, about half the time, less than half the time, less than 1 in 5 times and not at all (table 2). A decrease in frequency was observed in a number of patients after the trial.
IPSS score before and after the experiment
IPSS score indicated that the efficacy of homeopathy in case of BPH through various homoeopathic medications was subjective. More patients shifted from severe grade of IPSS score to moderate grade (figure 1). On the basis of the clinical symptoms collected from the patients related to BPH, the patients were categorized into mild (0), moderate (7) and severe (23) before the conduct of the experiment on the basis of the information provided by them with respect to the various items (subheadings/points). Similarly, after the conduct of the experiment, the patients were again categorized into mild (3), moderate (23) and severe (2) (figure 1).
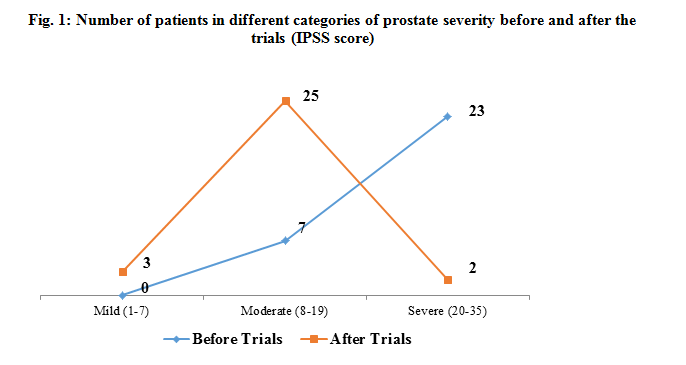
The results of the trial indicated that most of the patients with severe BPH were improved to moderate or mild BPH. This indicated the overall subjective improvement of the patients through various homoeopathic medications, thus showing the efficacy of homeopathy in case of BPH.
Conclusion
Paired t-test showed that the treatment provided
using ‘Sabal
serrulata Ø’ and ‘individualised medicines’ had a significant improvement in patients. The symptoms changed to
the desirable category (up to < half the time) was considered, the
improvement ranged from 33.3% (nocturia) to 73.3% (intermittency). The number
of total patients in the desired category ranged from 33.3% (weak stream) to
100.0% (straining). It was be observed that the sensation of incomplete
emptying of the urinary bladder, frequency of urination, complaint of
intermittency, urgency to urinate, improved flow of urine, decrease in need to
strain and needs to urinate at night has improved after the administration of
homoeopathic medications as compared to before the trial. On overall basis, in
twenty-six (86.7%) patients there was marked improvement in IPSS score of BPH
patients.
References
| 1 | GBD 2015 Disease and Injury Incidence and Prevalence, Collaborators. (8 October 2016). “Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015”. Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577 . PMID 27733282. |
| 2 | Michel MC, Heemann U, Schumacher H, Mehlburger L, Goepel M. Association of hypertension with symptoms of benign prostatic hyperplasia. J Urol 2004;172:1390-3. |
| 3 | Parsons JK, Carter HB, Partin AW, Windham BG, Metter EJ, Ferrucci L, et al. Metabolic factors associated with benign prostatic hyperplasia. J Clin Endocrinol Metab 2006;91:2562-8 |
| 4 | Roy A, Singh A, Sidhu DS, Jindal RP, Malhotra M, Kaur H. New visual prostate symptom score versus international prostate symptom score in men with lower urinary tract symptoms: A prospective comparision in Indian rural population. Niger J Surg 2016;22:111-7. |
| 5 | Boericke W. Pocket Manual of Homoeopathic Material Medica and Repertory. 9th ed. New Delhi: B. Jain Publishers; 1994 |
| 6 | MacLaughlin BW, Gutsmuths B, Pretner E, Jonas WB, Ives J, Kulawardane DV, et al. 2006 Effects of homeopathic preparations on human prostate cancer growth in cellular and animal models. Integr Cancer Ther 2006;5:362-72 |
| 7 | Chua T, Eise NT, Simpson JS, Ventura S. Pharmacological characterization and chemical fractionation of a liposterolic extract of Saw palmetto (Serenoa repens): effects on rat prostate contractility. J Ethnopharmacol 2014; 152:283–291 |
| 8 | Avins AL, Bent S. Saw palmetto and lower urinary tract symptoms: what is the latest evidence. Curr Urol Reports 2006; 7:260–265. |
| 9 | Jacobsen SJ, Jacobson DJ, Girman CJ, Roberts RO, Rhodes T, Guess HA, et al. Natural history of prostatism: Risk factors for acute urinary retention. J Urol 1997;158:481-7. |
| 10 | Levin RM, Haugaard N, O’Connor L, Buttyan R, Das A, Dixon JS, et al. Obstructive response of human bladder to BPH vs. rabbit bladder response to partial outlet obstruction: A direct comparison Neurourol Urodyn 2000;19:609‑29 |
| 11 | Oelke M, Rademakers KL, van Koeveringe GA. Detrusor contraction power parameters (BCI and W max) rise with increasing bladder outlet obstruction grade in men with lower urinary tract symptoms: Results from a urodynamic database analysis. World J Urol 2014;32:1177‑83. |
| 12 | Mirone V, Imbimbo C, Longo N, Fusco F. The detrusor muscle: An innocent victim of bladder outlet obstruction. Eur Urol 2007;51:57‑66. |
About Author:
Srishti Mahajan : Part of MD Dissertation
Rashid Akhtar : Prof. & Guide, Department of Organon of Medicine & Homoeopathic Philosophy, Bakson Homoeopathic Medical College & Hospital, Greater Noida (U.P.)
Jaya Gopalani : Prof. & HOD Department of Organon of Medicine & Homoeopathic Philosophy, Bakson Homoeopathic Medical College & Hospital, Greater Noida (U.P.)
Moumita Chakarborty : Senior Medical Officer & Incharge Homoeopathic Dept., GTB Hospital, New Delhi
Vishal Chaddha : Senior Medical Officer & Incharge Homoeopathic Dept., Dr Headgwar Hospital, New Delhi