
Abstract
Hyperparathyroidism is an endocrine condition, which is marked by excessive secretions of parathyroid hormone (PTH), which cause calcium and phosphorus imbalances. The condition can be in the form of primary, secondary and tertiary hyperparathyroidism, each having a different etiology and clinical implications. Since the introduction of biochemical screening, there are currently numerous instances that are diagnosed at an early or asymptomatic stage. Nonetheless, unmanaged hyperparathyroidism may result in serious skeletal, renal, gastrointestinal, as well as neuropsychiatric complications. This paper is a literature review of the parathyroid glands, anatomy, physiology, classification, pathogenesis, clinical presentation, diagnosis, complication, and the current management options of hyperparathyroidism.
Keywords: Hyperparathyroidism, Parathyroid hormone, Hypercalcemia, Primary hyperparathyroidism, Parathyroidectomy.
Introduction
Hyperparathyroidism is a calcium metabolic disorder that comes about as a result of excess production of parathyroid hormone (PTH) by the parathyroid glands. PTH is an important hormone that regulates the level of calcium and phosphate in the serum through its activity on gastrointestinal tract, kidney, and bones. The over secretion of PTH disturbs this balance causing hypercalcemia and its systemic consequences. The condition is becoming more known because of routine biochemical investigations and this has changed the clinical presentation of the condition to mild or asymptomatic type.
Anatomy and Physiology of the Parathyroid Glands.
The parathyroid glands are usually four small glands that are situated on the back of the thyroid gland which are endocrine glands. The secretion of PTH keeps calcium homeostasis by three main ways: firstly, by heating bone resorption, secondly, by accelerating renal tubular calcium reabsorption and excreting phosphate, and thirdly, indirectly by raising intestinal calcium absorption by stimulating vitamin D. The secretion of PTH is regulated by the calcium levels in the serum via a negative feedback process.
Hyperparathyroidism can be classified in the following way.
Primary Hyperparathyroidism
Primary hyperparathyroidism is caused by independent secretion of PTH, the majority of which are caused by one parathyroid adenoma. Rare causes are parathyroid hyperplasia, carcinoma and inherited endocrine syndromes, including multiple endocrine neoplasia (MEN). It is mainly manifested in middle-aged and old people, women in particular.
Secondary Hyperparathyroidism
Secondary hyperparathyroidism is physiological reaction to long term hypocalcemia. The common causes are chronic kidney disease, vitamin D deficiency and malabsorption syndromes. PTH level is high and the level of serum calcium is normal or low in this condition.
Tertiary Hyperparathyroidism
Tertiary hyperparathyroidism is a condition that occurs following secondary hyperparathyroidism especially in individuals with a long history of renal failure. The parathyroid glands turn autonomous causing continuous hypersecretion of PTH and hypercalcemia.
Clinical Features
Clinical manifestations of hyperparathyroidism could be either asymptomatic biochemical abnormalities to severe systemic involvement. Classical symptoms can be said to be summarized as stones, bones, abdominal groans and psychiatric moans. Renal manifestations are nephrolithiasis and nephro calcinosis. The involvement of the skeletons causes bone pain, osteoporosis, and fracture. The gastro intestinal symptoms are constipation, abdominal pain, nausea, and pancreatitis. Neuropsychiatricity is also likely to be fatigue, depression, and cognitive impairment.
Diagnosis
It is mainly a biochemical diagnosis, which is backed by imaging studies. Lab results comprise of high calcium in the serum with increased or inappropriately normal PTH. In primary hyperparathyroidism serum phosphate is usually low. Localization of abnormal glands is done using imaging modalities like the neck ultrasonography and technetium-99m sestamibi scans. The assessment of bone mineral density and renal imaging can be used to assess the complications of the disease.
Complications
The untreated hyperparathyroidism may lead to osteoporosis, pathological fracture, frequent renal stone, chronic kidney disease, neurocognitive dysfunction. CVD complications (hypertension and arrhythmias) were also reported.
Management
Surgical Management
The primary hyperparathyroidism (symptomatic as well as asymptomatic) is treated with parathyroidectomy the choice of treatment option in selected patients who are not symptomatic as well as those who are. Surgical cure is associated with high cure rates and offers much better long term outcomes.
Medical Management
The medical therapy is applied to the patients that are not surgical candidates. Management would incorporate proper hydration, vitamin D deficiency, administration of bisphosphonates to strengthen bones and calcitropic medication like cinacalcet to lower the calcium level in the blood.
Prognosis
When the condition is diagnosed and treated promptly, the prognosis of hyperparathyroidism is good. In the majority of cases, surgical management offers long-term remission, whereas in some patients, medical therapy is an effective treatment of biochemical abnormalities and decreases complications.
Conclusion
Hyperparathyroidism is a widespread endocrine disease that has a variety of clinical manifestations. Improvement of diagnostic methods has helped to detect them at an early stage and avoid the impact of serious complications. The full grasp of how it is pathophysiologically, naturally classified and managed is vital in providing the best care to a patient. Early intervention, especially surgery where necessary, will result in great results and better life quality.
Case:
The patient is a female, and her chief complaints were left renal region pains which became worse when motion and lifting of the body, cervical pain to cold air, frequent urination, generalized weakness, anxiety, and emotional disturbance due to changing residence repeatedly. The analysis of the case in detail showed a high level of necessity in stability and at the same time in the desire to move because of external conditions, which are characteristic of a mineral kingdom pathology. Calcifornia phosphorica was chosen with physical generals, mental state, and keynotes and source themes using 5 finger analytical method. Constitutional treatment was followed by marked improvement.
Patient Profile
Gender: Female
Marital status: Married
Occupation: Homemaker
Occupation of husband: State Bank of India officer.
Socio-family history: Badly shuffled around as a result of husband being a worker.
Chief Complaints (C/C)
Pain in left renal region
Cervical pain
Frequent urination
Weakness and musculoskeletal pains that are generalized.
History of Present Illness
According to the patient, the pain in the left-hand area of the kidneys is acute when walking and turning in bed. This pain grows during the process of lifting heavy items like buckets or bags. She cannot do routine chores in the house because of this pain which makes her very angry and frustrated.
She kept on comparing herself with other women of the same age where she said:
Other women of my age are able to work easy, I am weak and not able to work.
Complaints related to it are:
Cervical pain and made worse by cold air and better by wrapping the neck.
Frequent urination
In the morning it is made worse by sneezing.
Pains in muscles, heel, pains in bones, and significant weakness.
Psychological and Emotional Symptoms.
The patient stated that she is a reserved person that prefers to stay inside. Nevertheless, as the husband has a transferable occupation, she will have to switch residence every now and then, at times after two years.
She said she wanted a place of her own permanently, that she had been moved around:
Disturbs her emotionally
Interferes with the education of her children.
Eliminates emotional settlement.
She told me that as long as they get applied in a location, make friends there, and get emotionally settled, they are pushed to relocate once more. She is emotionally attached to individuals, prefers to have nurturing relations and wants to be nurtured.
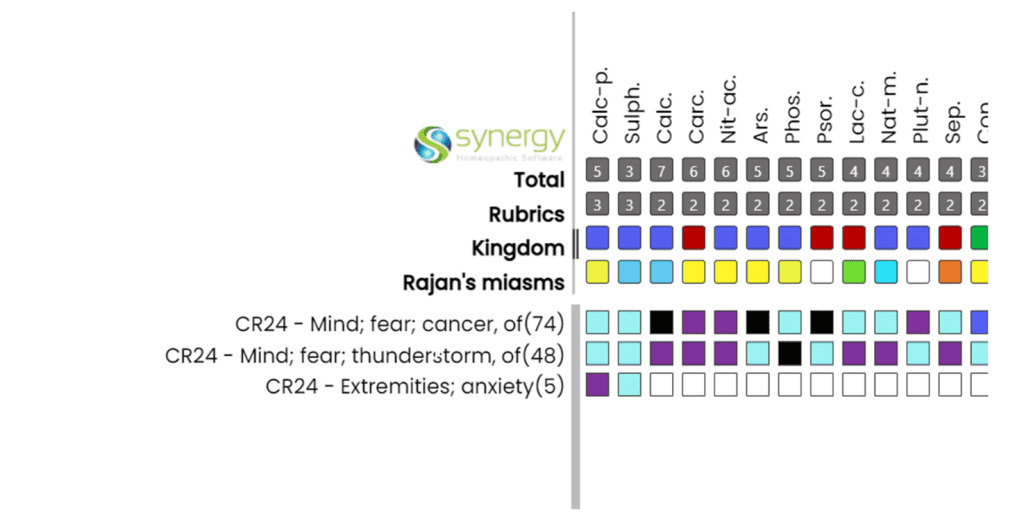
There was a serious anxiety that arose after a doctor noted that she had a tumor in her neck and this led to her being scared of contracting cancer particularly with the rising cases of cancer today.
She has some episodes of anxiety and restlessness in hands and feet, which are:
aajeeb si bechaini ho gayi thi haath aur pairon mein.
Fears
Fear of cancer
Concern with insufficiency of settlement and insecurity.
Fear of thunderstorm
Dreams
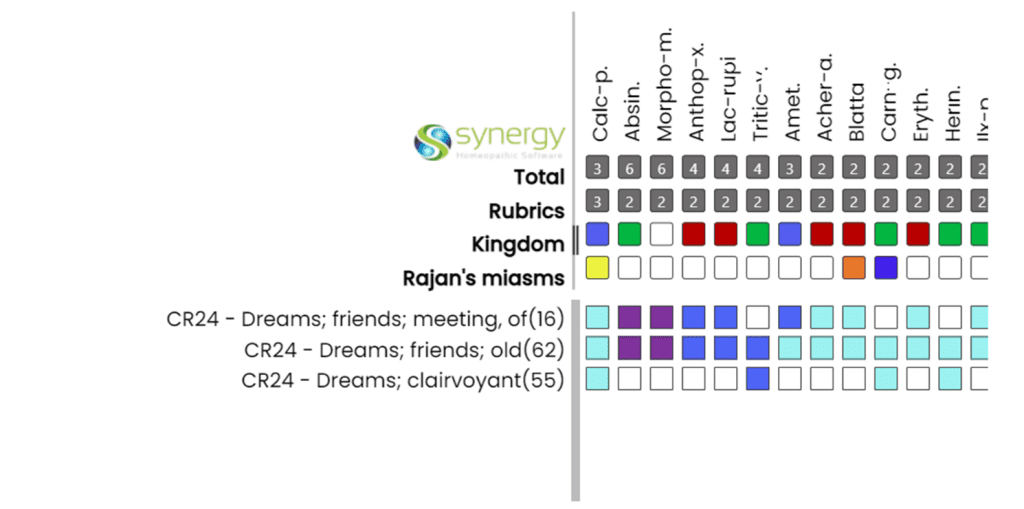
Reminiscences of school life, greetings with forgotten friends.
Flashbacks of past houses that she stayed in the past.
Delighted with fantasies, and identifies living persons with fancied ones.
Physical Generals
Thermal reaction: Chilly
Thirst: Thirsty
Desires:
Cold drinks
Ice cream
Salty food (chips)
Extreme craving meat and fish (quit when got married because of family regulations)
Perspiration:
Excessive on the head and face when cooking.
Watery, non-staining
Clinical Observations
Cold hands on touch
Long fingers
White spots on nails
Analysis (5-Finger Method)
Superclass / Subclass
Stability vs. Mobility 5th Series.
Powerful need of permanence, home, settlement.
Concurrent agony to act over and over again because of the situation.
Restless with malady, but made to move.
Theme: “Have to go, but once gone, would like to go back home.
Kingdom / Subkingdom
Calcium group, Mineral Kingdom.
Problems of sustainability, framework, frailty.
Bones, muscle pains, pains in kidneys.
Parental insecurity and support.
Nutritional and developmental malfunctions.
Miasmatic Understanding
Tubercular miasm
Want to change but feel too tired of being on the go.
Restlessness with weakness
Flashbacks of former locations and previous relationships.
Phobia, nervousness, and delicacy.
Characteristic Symptoms (Totality)
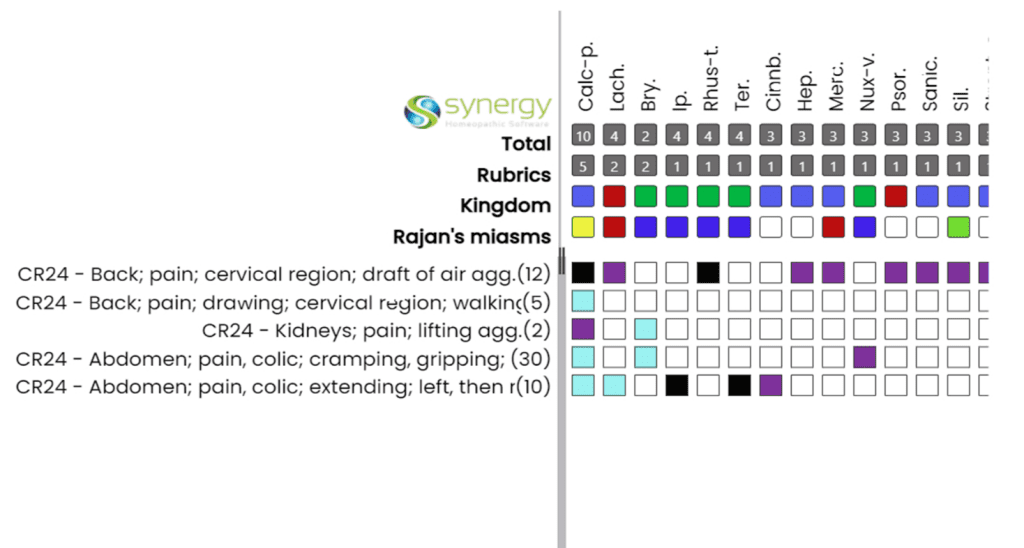
Left sided renal pain, worsened by movement, bed turning, exerting weight.
Cervical pain: < cold air, > covering
Cold-blooded thirsty constitution.
Longing after meat, fishes, salt food.
Sabrent perspiration on head.
Dissatisfaction caused by non-settlement.
Fear of cancer
White spots on nails
Source Quality / Keynotes
Homesickness and emotional insecurity.
Inability to stay stable under the pressure of the outside conditions.
White spots on nails
Bone and muscular pains
cold extremities, long fingers.
Sectorial Repertorial totality –
Remedy Selection
Remedy Selected: Calcarea Phosphorica.
Justification:
Calcium group remedy dealing with structure, support, weakness.
High bone, kidney, muscle affinity.
Strong need to be stable and movement needed.
Sensitivity to emotional instability and displacement.
Lust after meat and salt food.
White spots on nails
Miasmic background of tuberculosis.
Source reference:
Substance- The Mineral Kingdom.
The necessity to be stable and to move, the possibility to leave his/her stable world and come back to it.
Prescription
Calcarea Phosphorica 200C
two times per day in two days.
Followed by Sac Lac
Repetition plan:
200C after 1 month
1 M in 3 rd month (on condition of improvement)
Result of Investigation:
BEFORE TREATMENT
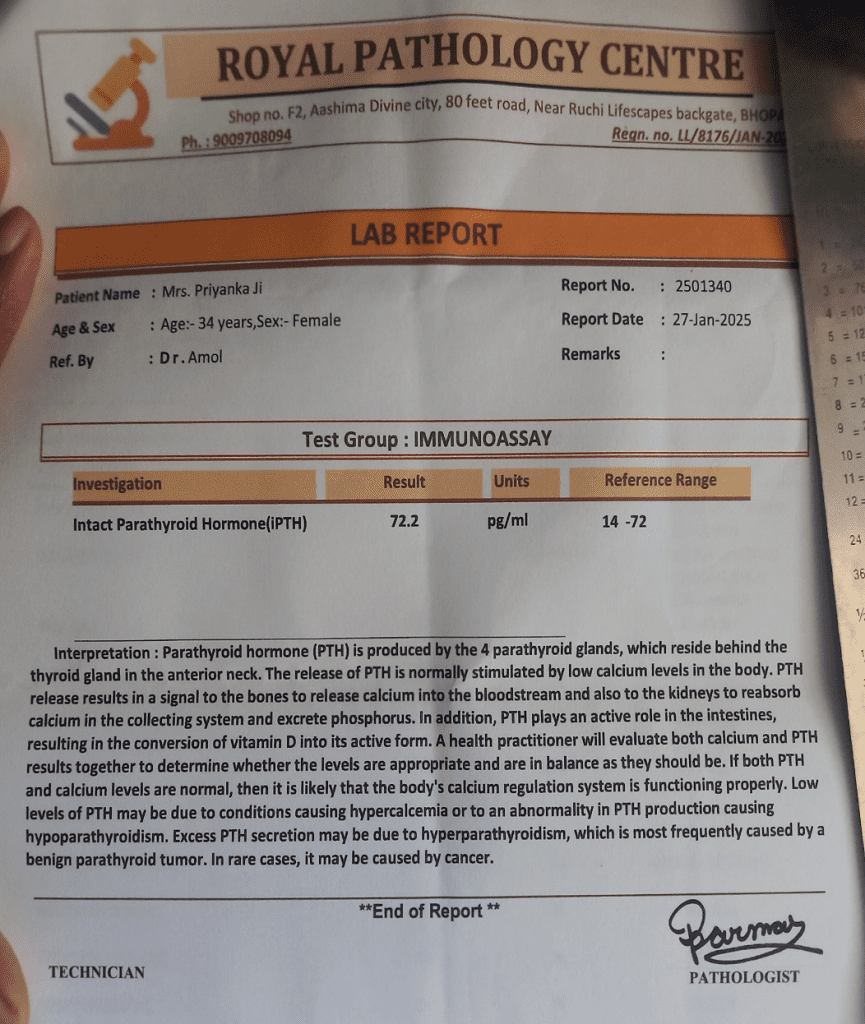
AFTER TREATMENT
Conclusion
This case illustrates that it is possible to see the main life theme of a patient when it is not limited to isolated symptoms. The tampering of the patient between his stability and forced mobility, as well as the typical physical and mental generals, it was evident that he was in a Calcarea phosphorica state. Holistic based constitutional treatment lead to a lot of relief and better emotional balance.
Author
Dr. Amol Singh Kirar
MD Scholar
Batch– 2022–23, Dept–Homoeopathic Repertory And Case Taking
Govt. Homoeopathic Medical College And Hospital, Bhopal (MP).
Co – Author
Dr. S.K Mishra
GUIDE,
PRINCIPAL AND CEO
Govt. Homoeopathic Medical College And Hospital, Bhopal (MP)



