
- It is defined as a chronic inflammation of the middle ear and mastoid cavity, which presents with recurrent ear discharges through a tympanic perforation and deafness.
The disease usually begins in childhood as a spontaneous tympanic perforation.
- It is long standing infection of a part or whole of the middle ear cleft characterized by ear discharge and a permanent perforation
- A perforation becomes permanent when its edges are covered by squamous epithelium and it does not heal spontaneously.
- A permanent perforation can be likened to an epithelium lined
fistulous track.
Epidemiology-
According to the World Health Organization (WHO), it affects anywhere between 65 and 330 million people worldwide. Global Burden of Disease Study 2010 assigned 4.68 million disability-adjusted life years (DALYs) to otitis media, a disease burden that is almost as high as the intestinal helminth infections. Incidence of CSOM is higher in developing countries because of poor socio economic status, poor nutrition and lack of health awareness. It affects both sexes and any age group can be affected. In India, the prevalence rate is 46 and 16 persons per thousand rural and urban populations respectively. It is the single most important cause of hearing impairment in rural populations in India . The global incidence rate is estimated at 4.76 cases per 1,000 inhabitants, whereby 22.6% of cases concern (6–7 months of age) children. The highest incidence is seen among children younger than 1 year. The lowest rate is among adults older than 65 years.
CLASSIFICATION OF CSOM-
1-Tubo tympanic type (Safe)
2- Attico antral type (Unsafe)
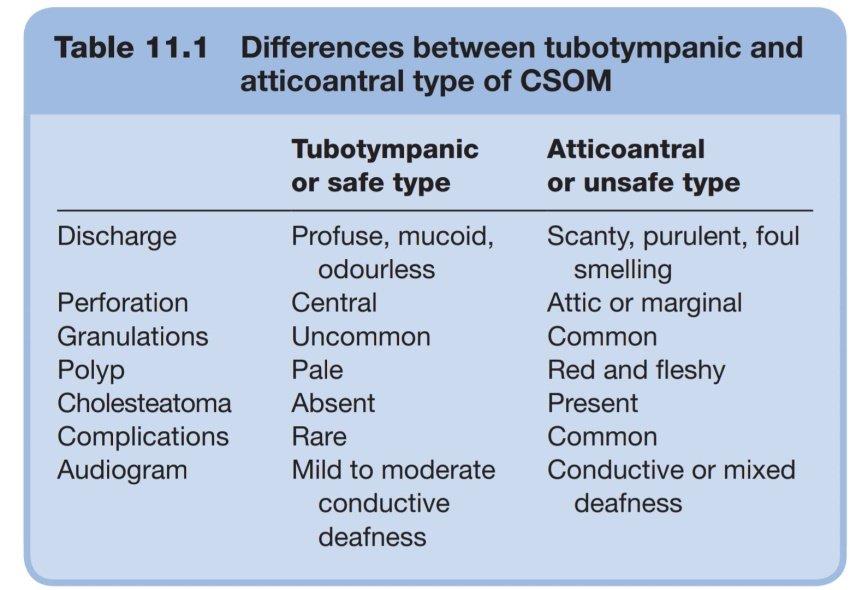
Differences between Tubotympanic and Attico-antral types of CSOM
1-TUBOTYMPANIC COSM (SAFE)
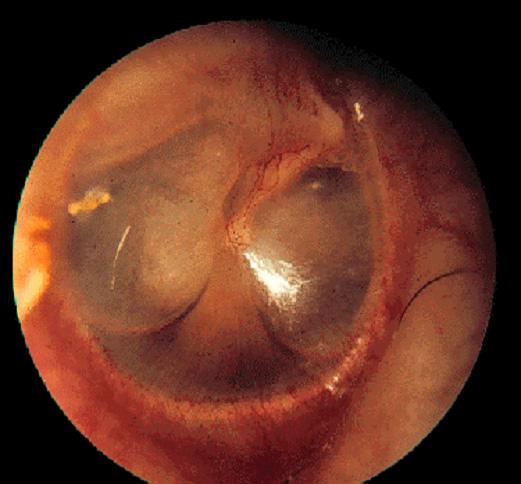
It is also called safe or benign type and inflammation is confined to the middle ear cleft . It is characterized by central perforation, profuse, mucoid, odorless discharge, and mild to moderate conductive deafness and absence of cholesteatoma formation. Cholesteatoma is a sac of keratinized desquamated epithelium in the middle ear cleft, resting on the fibrous tissue layer called matrix.
- Patency of Eustachian tube
- Nidus of infection in Upper Respiratory Tract Infection
- Aerobic and Anaerobic
Causes-
The disease starts in childhood and is therefore common in that age group.
1. It is the sequelae of acute otitis media usually following exanthematous fever and leaving behind a large central perforation. The perforation becomes permanent and permits repeated infection from the external ear. Also the middle ear mucosa is exposed to the environment and gets sensitised to dust, pollen and other aeroallergens causing persistent otorrhoea.
2. Ascending infections via the eustachian tube. Infection from tonsils, adenoids and infected sinuses may be responsible for persistent or recurring otorrhoea.
3. Persistent mucoid otorrhoea is sometimes the result of allergy to ingestants such as milk, eggs, fish, extra.
Pathogenesis- The tubotympanic disease remain localized to the mucosa and, that too, mostly to anteroinferior part of the middle ear cleft.
Tubotympanic CSOM usually starts from childhood. It can be the sequelae of acute otitis media following exanthematous fever, leaving a large central perforation. When the perforation becomes permanent, repeated infections from the external ear occur and middle ear mucosa gets exposed to dust, pollen and other aeroallergens causing persistent otorrhoea. Infections from tonsils, adenoids, and sinuses ascend via Eustachian tube causing persistent or recurrent otorrhoea. Allergic reactions to milk, egg, fish etc. may cause persistent mucoid ear discharge . Like all chronic infections, healing and destruction go hand in hand and either of them can be predominant, depending upon the virulence of the organism and resistance of the patient. This type is subdivided into tubal and tympanic types. In tubal types infection ascends through the Eustachian tube from nose, nasopharynx or sinuses. This type is more common in children. In tympanic type infection reaches the middle ear through tympanic perforation .
Pathological changes of tubotympanic type-
1. Perforation of tympanic membrane –Central perforation of pars tensa with varying size and position is the characteristic of tubotympanic type CSOM.
2. Edema of mucosa– Oedema and velveltty middle ear mucosa when there is active infection is another important pathological change. When disease is quiescent or inactive mucosa is usually normal in appearance.
3 . Polyp- A polyp is a smooth mass of edematous and inflamed mucosa which has protruded through a perforation and presents in the external canal. It is usually pale in contrast to pink, fleshy polyp seen in atticoantral disease.
4. Necrosis of ossicles- Usually the ossicular chain is intact and mobile. In advanced cases of CSOM, necrosis of bones occurs especially the long process of incus.
5. Tympanosclerosis- It is hyalinization and subsequent calcification of subepithelial connective tissue. It is seen in remnants of the tympanic membrane or under the mucosa of the middle ear. It is seen as white chalky deposit on the promontory, ossicles, joints, tendons and oval and round windows. Tympanosclerotic masses may interfere with the mobility of these structures and cause conductive deafness.
6. Fibrosis and adhesions- They are the result of healing process and may further impair mobility of the ossicular chain or block the eustachian tube.
Microbiology
CSOM is considered a multifactorial disease resulting from a complex series of interactions between environmental, bacterial, host and genetic risk factors. Pus culture usullay show multiple organisms. Common anaerobic organisms are pseudomonas aeruginosa, proteus, and E.coli and staphylococcus aureus. Common anaerobes include bacteriodes fragilis and anaerobic streptococci. P.aeruginosa, S.aureus and gram negative bacteria are the most common pathogens of CSOM. H. influenza is also found in some cases.
Clinical Features-
1.Ear Discharge- Discharge is usually non offensive, mucoid or mucopurulant; constant or intermittent. Discharge appears mostly with upper resoiratory tract infections or on accidental entry of water into the ear.
2.Hearing Loss- It is conductive deafness with varying severity but rarely exceeds 50 dB. Sometimes the patient presents with hearing better in the presence of discharge than when the ear is dry. This paradoxical effect is due to the round window shielding effect. When the ear is dry with perforation sound waves pass through an oval and round window simultaneously and cancel each other. In the presence of discharge phase differential is maintained, so the patient hears well. In long standing cases cochlea absorbs toxins from oval and round windows resulting in damage and hearing loss becomes mixed type.
3. Perforation- Central perforations can be anterior, posterior, inferior or subtotal. Usually perforations are described in relation with handle of malleus i.e anterior, posterior and inferior perforations to handle of malleus. Subtotal perforation of pars tensa is very large in size but the parts of pars tensa or annulus of tympanic membrane are preserved.
4. Middle Ear Mucosal Changes– Middle ear mucosa is seen when perforation is large. Normally it is pale, pink and moist. When inflamed, it becomes red, edematous and swellen. Polyp may be seen occasionally.
TYPES OF TUBOTYMPANIC CSOM-
A- Active TuboTympanic CSOM
B- Inactive TuboTympanic CSOM
2-ATTICOANTRAL CSOM (UNSAFE)
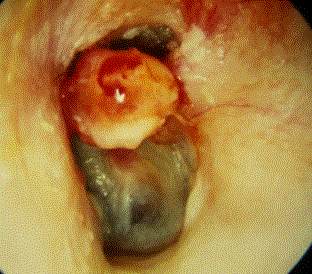
It involves the posterior superior part of middle ear cleft including attic, antrum and posterior tympanum and mastoid. It is associated with cholesteatoma.Cholesteatoma may cause bone erosions and serious complications are likely to occur. So this type is called unsafe or dangerous type. Atticoantral type is seen in sclerotic mastoid, and whether it is cause of effect, is not yet clear. It is characterized by marginal perforation, scanty, purulent, foul smelling discharge and is associated with presence of cholesteatoma and retraction pockets. The mainstay treatments are surgical with removal of cholesteatoma and reconstructive procedures like myringoplasty or tympanoplasty .
Pathological changes attico antral type-
- Cholesteatoma-
This term is misnomer.Cholesteatoma neither contains cholesterol nor it is an “oma” or tumor. Middle ear cleft is lined by different types of epithelium in different places. Anterior and inferior part lined by ciliated columnar epithelium, cuboidal in the middle and pavement like in the attic. Nowhere keratinized squamous epithelium is found in the middle ear cavity, when present in middle ear or mastoid it is called cholesteatoma.
It is the skin in the wrong place. Cholesteatoma consists of two parts, the matrix, made of keratinized squamous epithelium and central keratin debris. So it is also called epidermolysis or keratoma. The Genesis of cholesteatoma is a subject of debate. It may be due to congenital cell rests. There are various views regarding the origin of cholesteatoma.
In an article published in the journal of laryngology and otology in described that cholesteatomas originate from the retraction pockets of the tympanic membrane and there is active growth of the squamous epithelium of the retraction pockets, which may be enhanced in the presence of otitis media.
It is classified into congenital acquired primary and acquired secondary. Congenital variety originates from embryonic epidermal cell rests . It is usually seen in the middle ear, petrous apex and cerebellopontine angle. Symptoms depend on the location. A middle ear congenital cholesteatoma presents as a white mass behind an intact tympanic membrane and it causes conductive hearing loss. It may spontaneously rupture through the tympanic membrane and present with ear discharge, often mistaken as a case of CSOM. In primary acquired cholesteatoma, there is no previous history of otitis or tympanic membrane perforation. A secondary acquired cholesteatoma is seen in cases with a history of tympanic membrane perforation .
When cholesteatoma enters the middle ear cleft, it invades the surrounding structures and causes enzymatic bone destruction of ossicles, bony labyrinth, canal of facial nerve, sinus plate or tegmen tympani. Enzymes like collagenase, acid phosphatase, proteolytic enzymes liberated by osteoclasts and monocytes are seen in association with cholesteatoma. An attic cholesteatoma may extend backwards into the aditus, antrum and mastoid; downwards into mesotympanum; medially surround the incus and head of malleus.
2.Osteitis and granulation tissue- Osteitis involves attic wall and posterosuperior margin of tympanic ring. A mass of granulation tissue surrounds the area of osteitis. Fleshy red polyps may also be seen filling the meatus.
3. Ossicular necrosis- Usually destruction is limited to a long process of incus or it may involve stapes, handle of malleus or entire ossicles. So the hearing loss is always greater than that in the tubotympanic type. Occasionally cholesteatoma bridges the gap caused by destroyed ossicles and hearing loss is not apparaent. Such patients are called cholesteatoma hearers. Bateriology is the same as in tybotympanic type.
4. Cholesterol granuloma- It is a mass of granulation tissue with foreign body giant cells surrounding the cholesterol crystals. It is a reaction to long standing retention of discharges. Sometimes it coexists with cholesteatoma. Tympanic membrane appears blue when cholesterol granuloma is present behind the mesotympanum.
Clinical features–
- Ear discharge- Scanty, always foul smelling due to bone destruction.discharge may be so scanty that the patient may be unaware of it. Sudden stoppage of ear discharge must be viewd seriously because perforation can be sealed by crusted discharge, inflammatory mucosa or a polyp. Internal drainage of pus in such cases causes complications like meningitis, otogenic absesses etc.
- Hearing loss-Hearing is normal when ossicular chain is intact or when cholesteatoma, having destroyed the ossicles, bridges the gap caused by destroyed ossicles(cholesteatoma hearer). Hearing loss is mostly conductive but a sensorineural element may be added.
- Bleeding– Bleeding occurs from graulation tissue or polyps when cleaning the ear.
Signs-
1. Perforation- Perforation can either be attic or posterosuperior type. Small amount of crusted discharge or small granuloma may mask small perforations.
2. Retraction pocket- It is the invagination of the tympanic membrane seen usually in attic or posterosuperior area of pars tensa. In early stages, the pocket is shallow and self-cleansing but later when the pocket is deep, it accumulates keratin mass and gets infected.
3. Cholesteatoma– Pearly-white flakes of cholesteatoma can be sucked from the retraction pockets. Suction clearance and examination under operating microscope forms an important part of the clinical examination and assessment of any type of CSOM
DIAGNOSIS
1.History taking
2. Examination under microscope-
Presence of granulation, in-growth of squamous epithelium from edge of perforation, status of ossicular chain, tympanosclerosis, and adhesions can be seen through microscope. An ear which appears dry may show hidden discharge under a microscope.
- Culture of ear discharge–
It is used to identify the specific microorganism causing the disease.
- Mastoid x ray/ ct scan of temporal bone-
Mastoid is usually sclerotid but may be pneumatised with clouding of air cells. Bone destruction can be identified.
- Otoscopy–
The diagnosis of CSOM rests on the verification of a discharging tympanic membrane perforation. This is only possible by removing obstructing wax, ear discharge, debris or masses in the external auditory meatus and visualizing the whole expanse of the. This requires adequate illumination through a head mirror, head light, otoscope or otomicroscope, suction apparatus and small instruments.
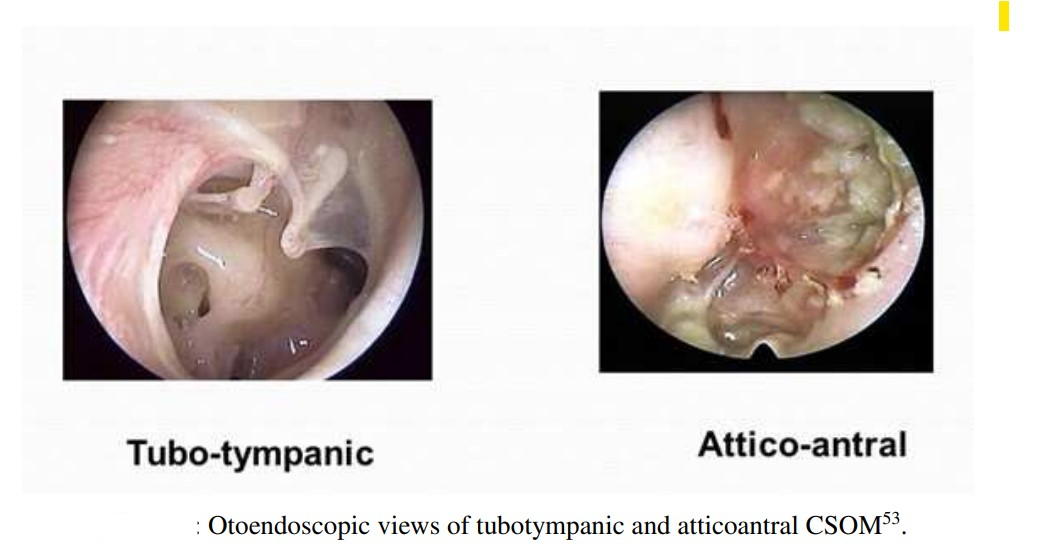
- Otoendoscopy-
Otoendoscopy is very useful technology in modern times. Endoscopes with small diameter and wide fields of view provide extra ordinary visualization of middle ear, which was previously accessible only by surgical means. Usually the otavite endoscopes in the size of 1.7 mm with 0° – 30° view of angle and in size of 2.4 mm with 0,30 and 70 degree view of angle are used. Using a 0-degree endoscope, the intact drum call is examined and the movements of the eardrum evaluated. A fluid level due to middle ear effusion can also be seen than with conventional otoscope. A 30-degree endoscope can sometimes be passed through the perforated ear drawn to determine the integrity of the ear ossicles.

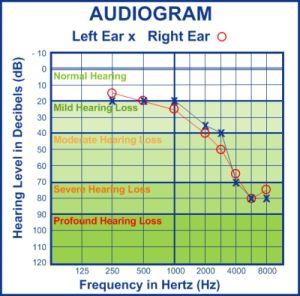
Audiogram–
Assessment of hearing Conductive deafness is usually caused by external ear obstructions, tympanic membrane perforations, middle ear fluids, fixation of disruption of ossicles, Eustachian tube obstructions etc. sensorineural deafness can be sensory or neural types. Lesions of cochlea causes sensory deafness and lesions of 8th cranial nerve and its central connections cause neural type of deafness. Deafness due to lesions The 8th alone is called retro cochlear and the other which is caused by central auditory connections is called central deafness. When elements of both conductive and sensorineural deafness are present in same ear, It is called mixed deafness.
Clinical tests of hearing
Normally a person hears voices of conversations at a distance 12 metres or 40 feet and whispers at 6 metres or 20 feet. Patients should be asked for any difficulty in hearing conversational or whispering voices.
1.Tuning fork tests-
Hearing through air conduction (AC) is louder and heard twice than through bone conduction (BC). Tuning fork of 512 Hz is activated by striking gently against examiners hand or elbow and the vibrating fork is placed vertically 2cm away from external auditory meatus of both ears then vibrating tuning fork is placed firmly on the mastoid bone. Both are compared to assess hearing. Bone conduction is a measure of cochlear function only but air conduction tests both conduction system and cochlear function.
2.Rinne’s test-
In this test air and bone conduction are compared. Bone conduction is tested first and then air conduction. If he still hears, it means air conduction is more than bone conduction. Rinne’s test is positive when AC is longer or louder than BC which is seen in normal persons or in sensorineural deafness. Rinne’s test is negative (AC<BC) in conductive deafness. A negative Rinne indicates minimum air bone gap of 15-20 dB. False Rinne’s negative can be seen in unilateral sensorineural hearing loss.
3.Weber test-
Vibrating tuning fork is placed either on the mastoid or vertex and the patient is asked in which ear sound is heard. Normally sound is heard equally on both sides. In conductive deafness sound is laterised to the worse ear and in sensorineural deafness it is lateralized to normal ear. Here sound travels directly to the cochlea via bone. Lateralisaition of sound in the weber test implies conductive hearing loss 15-25 dB in the ipsilateral ear or a sensorineural loss in the contralateral ear.
4.Pure tone audiometry-
An audiometer is an electronic device which produces pure tones, the intensity of which can be increased or decreased in 5 dB. The amount of intensity to be raised above normal is the measure of degree of impairment. It is charted in the form of a graph called an audiogram. Threshold of bone conduction is the measure of cochlear function and difference is thresholds of air and bone conduction is the measure of conductive deafness. When the difference between the two ears is 40dB or above in air conduction thresholds, the normal ear is masked to avoid getting a shadow curve from the nonmeat normal ear. Masking is done in bone conduction studies also. Degree and type of hearing loss can be studied by pure tone audiogram. The record can be used for hearing aid prescription, future reference and to predict speech reception threshold.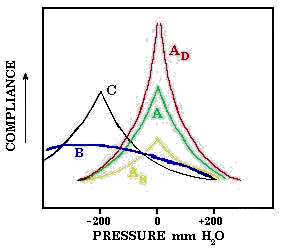
5.Tympanometry-
When sound waves strike the tympanic membrane some of the sound energy get absorbed while the resr is reflected. Stiffer tympanic membrane reflects more sound energy. Tympanometry is the measure of compliance or stiffness of tympano ossicular system and thus middle ear function. Graphical representation of tymanometry is called tympanogram.
6.Radiology–
It does not have a significant role in diagnosing CSOM. It is useful in assessment of anatomical type of mastoid bone, i.e. cellular, diploic or sclerotic pathological changes to mastoid air cells like blurring of cells, coalescence of cells bone erosions, cavitation size and extent of cholesteatoma. Standard X ray views are Law’s view which is the laletal oblique view of mastoid and schuller’s view to visualize exent of pneumatisation, destruction of intercellular septa, location of sinus plate and tegmen, choleateatoma and fracture of petrous pyramid.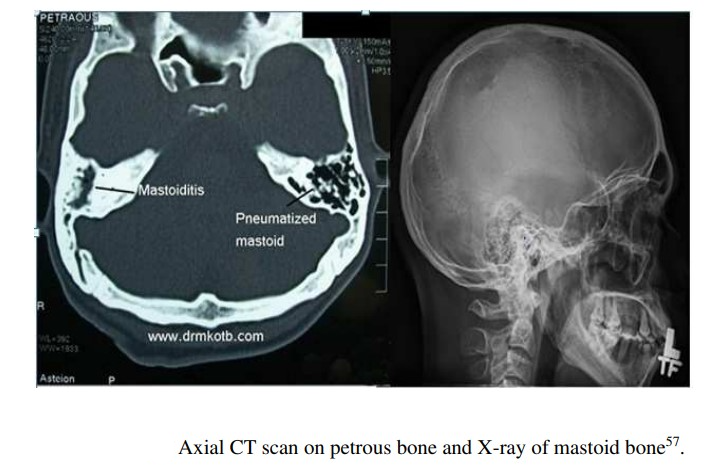
DIFFERENTIAL DIAGNOSIS
The presence of a persistent tympanic membrane perforation and middle ear discharge differentiates CSOM from other chronic forms of otitis media. CSOM is also called chronic active mucosal otitis media, chronic oto-mastoiditis, and chronic tympanomastoiditis. The non-CSOM group includes such entities as chronic nonsuppurative otitis media, chronic otitis media with effusion (COME), chronic secretory otitis media, chronic seromucous otitis media, chronic middle ear catarrh, chronic serous otitis media, chronic mucoid otitis media, otitis media with persistent effusions, and glue ear. All these are recurrent or persistent effusions in the middle ear with intact tympanic membrane in which the principal symptom is deafness and not ear discharge.
Acute otitis externa and acute otitis media also can produce both ear pain and ear discharge. Tragal pain is found in otitis externa and mastoid pain in otitis media. Fever is also higher in acute otitis media than in otitis externa. CSOM produces painless mucoid ear discharge without fever, unless accompanied by otitis externa or complicated by an extracranial or intracranial infection.
Tuberculous otitis media
It is usually secondary to pulmonary tuberculosis, seen in children and young adults. There is painless necrosis of tympanic membrane.Multiple perforation are characteristic which can coalesce to form a large perforation. Middle ear and mastoid get filled with pale granuloma.Bone caries, psot auricular fistula are seen. Facial paralysis is common. Painless discharges, severe conductive hearing loss due to involevement of labyrinth are other important features .
Syphilitic otitis media
It is a rare condition. Infection reaches the middle ear through the Eustachian tube or blood. Sensory end organs of the inner ear are invaded causing sensoruneural hearing, tinnitus or vertigo. Bone necrosis is also common.Secondary pyogenic infection results in symptoms similar to CSOM. Diagnosis is made by treponemal pallidum immobilization (TPI) test and fluorescent treponemak antibody absorption test (FTAABS). VDRL and wasserman tests are nonspecific and may give false positive results.
Otitis media with effusion
This condition is also called serous otitis media, secretory otitis media, and mucoid otitis media. This is an insidious condition with accumulation of non purulent effusion in the middle ear cleft. Effusion can be thick, viscid or thin, serous type. This condition is commonly seen in school going children. Malfunctioning of the Eustachian tube or increased secretory activity of middle ear mucosa, nasopharyngeal tumors, palatal defects like cleft palate are the important causes.Otitis externa presents with ear discharge but no membrane perforation. Foreign bodies in the ear, impacted earwax, very rarely wegers granulomatosis and neoplasms should be ruled out. International journal of otolaryngology reported a case of squamous cell carcinoma of middle ear mimicking CSOM reported in Department of ENT, Grant Medical College & Sir J.J. Hospital, Mumbai.The journal says “even though squamous cell carcinoma (SCC) of the middle ear and chronic suppurative otitis media (CSOM) co-exist, no definitive correlation has been proven”.
Homoeopathic Therapeutics
- AUR MET- Obstinate fetid otorrhoea after scarlatina.External meatus bathed in pus.Caries of ossicula and of mastoid. Chronic nerve deafness; Labyrinthine disease due to syphilis. Caries: of the nasal palatine and mastoid bones; ozaena, otorrhoea, excessively foetid discharge, pains worse at night; drive to despair; of mercurial or syphilitic origin (Asaf.)
- ANT CRUD- Moist eruption on external ear and behind it; scrofulous otorrhoea; chronic catarrhal otitis media with heat and tension, aggr. by heat.
- CALC CARB- Scrofulous inflammation with muco-purulent otorrhoea, and enlarged glands.
- CALC F- Calcareous deposits on tympanum; sclerosis of ossicula and petrous portion of temporal bone, with deafness, ringing and roaring. Chronic supuration of middle ear.
- CALC SULPH- Deafness, with discharge of matter from the middle ear, sometimes mixed with blood. Pimples around the ear.
- CAPSICUM– Burning and stinging in ears. Swelling and pain behind ears. Inflammation of mastoid. Tenderness over the petrous bone; extremely sore and tender to touch. (Onosmod) Otorrhoea and mastoid disease before suppuration.
- CAUSTICUM– Ringing, roaring, pulsating, with deafness; words and steps re-echo; chronic middle-ear catarrh; accumulation of ear-wax.
- FERR PHOS– Purulent discharge from the ear. Itching in my ear. Noises in the ear, roaring; buzzing, humming, ringing and singing.Catarrh of Eustachian tubes. Inflammatory pains in the ear. Otitis media. Pain deep in the ear. Drawing. Stitching.Pain and swelling of the parotid gland. Sensitive to noise. Impaired hearing
- KALI BICH- Discharge of thick, yellow, foetid pus; itching deep in ear, with stinging pains; sharp stitching pains dart from the ear to throat. Ulcers upon tympanum, which are dry but not painful, excepting the sharp stitches; naso pharyngeal catarrh. Ulceration of anterior nares with a discharge of tough, ropy mucus; indolent ulcers; glands swollen; neck painful to touch; after scarlatina.
- MANGANUM ACETICUM– Feel stopped; cracking on blowing nose. Pain from other parts extends to the ears. Deafness in damp weather. Whistling tinnitus.
- MERC SOL– Thick, yellow discharge; fetid and bloody. Otalgia, worse warmth of bed; at night sticking pains. Boils in an external canal. (Calc. pic.)
- MERC COR– Violent pulsations in ear. Fetid pus from ear.
- MERC DULCIS– Otitis media; closure of Eustachian tube; ear troubles of scrofulous children; membrana tympani retracted, thickened and immovable.
- PSORINUM– Chronic otorrhoea. Most fetid pus from ears, brownish, offensive.
- SILICEA– Fetid discharge; Caries of mastoid; loud pistol-like report; Sensitive to noise. Roaring in ears.
- THUJA OCC- Chronic otitis; discharge purulent; Creaking when swallowing. Chronic otitis; discharge purulent, like putrid meat; granulations, condylomata; polypi, pale red, cellular, bleeding easily.
- TELLURIUM– Otitis media with rupture of tympanum, pouring out pus which at first may be fair, but afterwards becomes offensive, smelling like fish brine. Membrana tympani irregular, thickened in parts, thin in other portions; vesicular eruption on membrane, then suppuration and perforation; whatever discharge touches becomes excoriated and little vesicles appear on excoriated surface; ear bluish-red, as if oedematous; hearing impaired; sensation as if something suddenly closed up the ear, as if air whistled through left Eustachian tube, when snuffing or belching; throat dry and sore, amel. By eating and drinking. Otto lesser in the textbook of Homoeopathic materia medica says tellurium is indicated for ear discharge smelling like herring brine due to presence of trimethylamine.
- TUBERCULINUM– Persistent, offensive otorrhoea. Perforation in membrana tympani, with ragged edges.
- KALI MUR– Chronic, catarrhal conditions of the middle ear; glands above the ear swollen; Snapping and noises in the ear. Threatened mastoid. Great effusion about the auricle.
- KALI SULPH– Eustachian deafness. Discharge of yellow matter. (Hydr). Deafness from congestion of the tympanic cavity, or with catarrh and swelling of Eustachian lining. Worse in a heated room, with a yellow, slimy coating on the tongue. Earache, with discharge of watery or yellow matter. Secretion of thin, bright-yellow, or greenish fluid after inflammation. (Thick, pus-like discharge, Calc. sulph.). Pain under the ear, sharp, cutting pain, tension, stitches and piercing below the mastoid process. Stinking, otorrhoea. Polypoid excrescence closes the meatus.
- KREOSOTE– Eruption around and pimples within. Difficult hearing and buzzing. Difficulty in hearing before and during menses.
- PULSATILLA– Sensation as if something were being forced outward. Hearing difficulty, as if the ear were stuffed. Otorrhoea; thick, bland discharge; offensive odor. Ache agg. night. Deafness as if ears were stopped up; can hear better in the car; and in a warm room. Otorrhoea; discharge of pus, of blood; thick yellow humour, offensive; after exanthemata.
- HEPAR SULPH– Discharge of fetid pus from the ears. Whizzing and throbbing in the ears, with hardness of hearing. Deafness after scarlet fever. Pustules in the auditory canal and auricle. Mastoiditis.
- ELAPS COR– Cerumen black and hard, with difficult hearing, or serous greenish discharge, offensive; buzzing, and illusion of hearing. Sudden attack of nightly deafness, with roaring and crackling in ears, cracking in ears on swallowing. Intolerable itching in the ear.
- LACHESIS– Tearing pain from zygoma into ear; also with sore throat. Ear-wax hard, dry. Roaring and ringing in ears, tinnitus aurium, amel. by putting finger in ear and working it; earwax pasty and offensive; catarrh of ear and swelling between ear and mastoid process, with throbbing pain and stiffness; left-sided deafness, with great dryness of affected ear and want of earwax; dry, scurfy nostrils
- LYCOPODIUM- Thick, yellow, offensive discharge. Eczema about and behind my ears. Otorrhoea and deafness with or without tinnitus; after scarlatina. Humming and roaring with the hardness of hearing; every noise causes a peculiar echo in the ear.
- SANICULA– Soreness behind ears with discharge of white, gray, viscid fluid (Graph., Psor.)
- SULPHUR– Whizzing in ears. Bad effects from the suppression of an otorrhoea. Oversensitive to odors. Deafness, preceded by exceedingly sensitive hearing; catarrhal deafness.
- SYPHILINUM– Deafness, without any obvious cause; nervous with cachexia. Calcareous deposit on tympanum. Abscess of the middle ear.
RARE MEDICINES FOR CSOM
- THYMULINUM–
Recurrent inflammation of middle ear. History of recurrent tonsillitis. Remedy for influenza. Constipation. Abundant ideas in morning after risisng
- SABAL SERRULATA–
Chronic inflammation of middle ear sounds seems distant.
- MANGANUM-
Chronic inflammation of the middle ear. Sensation as if one ear is hot and other not . Reddish discolouration of tympanum . Ofensive ear discharge. Coldness of meat as if from wind. Air sensation as if air rushing into the ear.
REFERENCES
- Dhingra PL, Dhingra shruthi, Dhingra deeksha. Diseases of ear, nose and throat and head and neck surgery. 6th edition: Elsevier; 2014.
- Monique Verhoeff a, Erwin L. van der Veen a, Maroeska M. Rovers a, b, c, Elisabeth A.M. Sanders c, Anne G.M. Schilder. Chronic suppurative otitis media: A review.international Journal of Pediatric Otorhinolaryngology (2006) 70, 1-12-elsevier.
- “Ear Bone – Anatomy”. Encyclopedia Britannica. N.p., 2017. Web. 5 May 2017.
- Levi J, Robert C O’Reilly. Chronic suppurative otitis media (CSOM): Pathogenesis, clinical manifestations, and diagnosis. http://www.uptodate.com/contents/chronic-suppurative-otitis-mediacsompathogenesis-clinical-manifestationsand-diagnosis
- Nelson, John D.chronic suppurative otitis media.Pediatric Infectious Disease Journal: 1988 ;7(6) : 446-448
- Morrison R .Desktop companion for physiological pathology. Hahnamann clinic publishers;1998
- Close Stuart.Genius of Homoeopathy.Second edition.New Delhi: B Jain publishers; 2005
- Clark J H. The presciber. New Delhi: B. Jain publishers; 1998
- Kent J.T. Repertoty of Homoeopathic materia medaica.New Delhi: B Jain publishers; 2007:285-320
- Allen T F. Boenninghaussen.therapeutic pocket book.13th edition.New Delhi;2003
- Boericke Oscar.Pocket Manuel of Homoepathic materia medica and repertory. 3rdrevised and augmented edition based on 9th edition. New Delhi: B Jain publishers; 2012
- Boericke William.Pocket Manuel of Homoeopathic Materia Medica and Repertory. 3rd revised and augmented edition, based on 9th edition: New Delhi. B.Jain Publishers; 2012.
- Hering C.Guiding symptoms of our Materia Medica. Reprint edition. New Delhi:B.Jain publishers;1997
- .Clarke J H .Dictionary of Practical Materia Medica.New Delhi: B Jain publishers;1978
- Deway W.A .Practical Homoeopathic Therapeutics.3rd edition. New Delhi: B Jain publishers;2005



