
Most of the woman now a day refers their private part as vagina so before explaining the anatomy of vagina it is necessary to understand the term that most women misuse. Thus without feeling ashamed to tell it out loud that your private part is not vagina it is“vulva”
Vulva
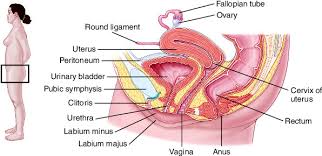
It includes mons veneris, labia majora, Labia minora, clitoris, vestibule and conventionally the perineum. These are visible on external examination but whereas vagina is not visible on external examination
Vagina
It is a fibro muscular membrane sheath communicating the uterine cavity with exterior at vulva. It is bounded anteriorly by Mons veneris, laterally by labia majora and posteriorly by perineum. It constitute excretory channel for the uterine secretions and menstrual blood. It is the organ of copulation and forms the birth canal of parturition.
Vaginal discharges
Physiological pathological
The vagina the vagina in a woman of reproductive age normally contains secretions consisting of
- vagina transudate
- cervical mucus
- uterine secretion
- secretion from bartholin glands
- fallopian tube secretion
An increase production of this normal secretion is the most common cause of symptomatic vaginal discharge and it is termed leucorrhoea.
The main causes are:-
- Hyper secretion of the cervical glands associated with
- Pelvic congestion (due to pelvic pathology or psychosomatic)
- Cervical ectopic columnar epithelium (due to increase in oestrogenic stimulus which causes hypertrophy of endocervical glands)
- Oestrogenic oral contraceptives
- Pregnancy
- Ovulation cascade
b) Uterine secretions (blood and menstruation)
c) Bartholin’s glands (activated by sexual excitement)
d) Increased vaginal transudation (due to sexual excitement)
Pathological discharge
- Trichomonas vaginalis Vaginitis –It is most common and important cause of vaginitis in child bearing period. Discharge will be frothy yellow green and offensive may be associated with pruritis. Possible associated finding dysuria inflamed vagina (Strawberry vagina) can be even asymptomatic.
- Monilial vaginitis/Thrush/Moniliasis/Candida vaginitis- It is caused by candida albicans (gram positive yeast like fungus). The discharge will be thick yellow, creamy or yellow- white discharge which can be associated irritation causes a desire to rub vulva. On examination, classically inflamed with white cheesy plague of discharge which on rubbing away leave multiple haemorrhagic spots.
- Childhood vaginitis- It is commonest during childhood. Due to lack of oestrogen, vaginal defence is lost. The discharge can be purulent (pre-pubertal child) associated with soreness of vulva and dysuria.
- Atrophic / senile vaginitis –It is seen in post menopausal woman. The discharge maybe blood stained can also have vulva or perineal discomfort and on examination vaginal epithelium – thin and atrophic with multiple reddened areas.
- Chlamydial vaginitis –It is caused by chlamydia trachomatis (gram negative obligate intracellular bacteria). It is common sexually transmitted disease. The discharges are irritant mucopurulent associated with dysuria. Diagnosis is only confirmed by tissue culture and serological test.
- Traumatic Vaginitis –It is due to chemical irritation (dettol household acidic solution used as spermicide etc), burns (douching with hot fluid), abrasion and laceration (commonly following intercourse and childbirth).
- Malignancy –Malignancy of vagina, cervix, uterus/ fallopian tube may cause a mucopurulent or haemorrhagic vaginal discharge. Ovarian tumors can have bloody discharge secondary to hormonal effects on endometrium
- Foreign bodies –Most common cause of vagina discharge in children.
- Fistula – Maybe urinary/faecal, typically follow radiation, major gynaecological surgeries, diverticulitis, crohn’s disease or “less commonly” a different confinement.
- Other
Granulation: after hysterectomy, mucopurulent discharge
Vagina, cervical and uterine polyps and sub mucus fibroids: ulceration and infection, foul purulent discharge.
Abortions: retained products of conception may undergo autolysis and become secondarily infected leading to a haemopurulent discharge.
Investigation and diagnosis of vaginal discharge and pelvic infection
- When a woman presents with a vaginal discharge and/or evidence of pelvic inflammation a systemic diagnostic approach is essential. Two things in particular must always be excluded. Firstly, a pregnancy state (including ectopic pregnancy, threatened abortion and hydatidiform mole and, secondly, malignancy (ovarian to vulva).
- Take a full gynaecological history and perform a complete examination. This will often give a definite if diagnosis or will at least suggest the relevant investigations to be carried out.
- Take a papanicolan smear. This should be done routinely if one has not been taken in the previous 12 months and is particularly indicated in case of abnormal vagina bleeding, dyspareunia, or if the cervical epithelium appears abnormal when visualised.
- If an infected vagina discharge is present, high vagina, cervical and urethral swaps should be taken for culturing. If charcoal impregnated swabs and Stuart’s transport medium are used, then gonococci, if present, will survive and grow as distinct colonies. This specimen should be cultured on both blood Agar and chocolate blood Agar in CO2 enriched atmosphere (for gonococci).
- Microscope slide preparation may be made using gram stains (looking for intracellular gonococci and monilial hyphae) or, if it is desired, trichomonas maybe visualised alive in a drop of warm Saline.
- If pelvic infection is suspected the following investigation may be also helpful
- Haemoglobin – may be low if chronic bleeding has occurred
- White cell count – high values indicate infective process.
- ESR- elevated values are of little use as they may reflect an inflammatory or malignant process.
- Mantoux test – a negative result may be exclude TB
- Chest x-ray- may reveal a primary TB focus or secondary neoplastic lesion.
N.B: D&C and hysterosalpingogram should not be performed if active pelvic inflammatory disease is suspected.
Homoeopathy therapeutics
- Aconite
Leucorrhoea, with sensation of heat, fullness and tension in internal parts; continual tinkling, not disagreeable, but forcing her to scratch; burning on urinating; discharge copious, tenacious, yellow; abdomen exceedingly sensitive.
- Ammonium carb
Acrid leucorrhoea, with sensation of excoriation and ulceration in vulva; profuse, watery, burning, from uterus with violent tearing in abdomen and acrid, profuse from the vagina; irritation of clitoris; want of appetite, poor, unrefreshing sleep; headache after waking in fresh air ;sleepy by day, sleepless at night; adapted to sickly, delicate, weak woman.
- Calcarea carb
Leucorrhoea of infants and before puberty; before and after menses; Milky, with burning and itching of vulva; cervical leucorrhoea, discharge albuminous, attended with great lassitude and debility; sinking and trembling at stomach; sharp stitches and burning in cervix; increased discharge after excitement; aching in vagina an itching in pudendum; much mucus between Labia and thighs, with biting pains; voluptuous sensation in genital organs of woman with too copious and often recurring menstruation; worse by day, when urinating, after exercise; chlorosis.
- Erigeron canad.
Profuse uterine and vagina leucorrhoea, with spasmodic pain and irritation of bladder and rectum, usually scanty menses; chronic uterine leucorrhoea; urination painful or suppressed.
- Kreosotum.
Leucorrhoea like menses, discharge bland or acrid; before and after menses, especially when standing hardly any when sitting or lying down; discharge of blood and mucus in the morning when getting up; acrid yellowish- white leucorrhoea, with great itching at vulva; Milky leucorrhoea, acrid leucorrhoea, leaving yellow spots on linen and stiffening it like starch, flesh coloured discharge, having a foul smell yellow, offensive and acrid discharge with itching, biting, smarting an burning in pudendum, between Labia and thighs; stitches in vagina from above downwards, causing her to start; frequent urging to urinate, preceded by a white discharge from vagina, which colors her clothes yellow; ineffectual urging to urinate, and when accomplished is accompanied by chilliness and Milky leucorrhoea; great debility, every little excretion throws her into a profuse sweat; white, painless leucorrhoea, smelling like fresh green corn, flowing like the menses with pain in back and flushes of heat in face; especially adapted to a cachetic state during and after climaxis or to blonde, overgrown girls of a sad, irritable disposition.
- Lycopodium
Profuse leucorrhoea in start and at interval, preceded by sharp cutting pain in hypogastrium; Milky, blood- red our rose- coloured discharge aggravation just before the full of the moon; corroding leucorrhoea with cutting pain across abdomen from right to left and jerking of lower extremities; discharge of flatus from vagina; fermentation in abdomen.
- Pulsatila
Painless leucorrhoea, discharge of thick, white mucus, milky, < on lying down; burning, thin acrid, Milky, mucus; thick and white leucorrhoea before and during menses, with cutting pain in abdomen and cramps in bowels; Milky leucorrhoea with swelling of Labia, particularly after menses; masturbation causes leucorrhoea and hysterical symptoms with great sexual excitement; leucorrhoea in young girls about puberty or when menses were suppressed by fright or from exposure to cold and dampness; leucorrhoea with chilliness, sadness and peevishness, <evening, > fresh air
- Sepia
Suitable to children and feeble debilitated woman of dark complexion, with fine delicate skin and extreme sensitiveness to all impressions. Leucorrhoea, with stitches in uterus and great itching in vagina and vulva; profuse leucorrhoeal discharge with darting pain in the region of cervix uteri; shooting upwards; Milky leucorrhoea only in daytime; sudorhystericus, a peculiar foetid perspiration, especially from the genital organs, axilla and soles; foetid putrid urine, depositing a reddish clay-coloured sediment, sensation as if everything would come out of the vagina, she has to cross her limbs to prevent it; sexual intercourse very painful, hardly endurable; putrid, excoriating discharge from uterus; with shooting stitching and burning in the neck of uterus; Painful sensation of emptiness and goneness at the pit of the stomach; leucorrhoea < after coition.
About Author:
Dr Ashna S, Assistant Professor, Department of Obstetrics & Gynecology,
Yenepoya Homoeopathic Medical College & Hospital,
Mangaluru, Yenepoya (Deemed to be University).