FISTULA
➢ A fistula is a communicating track between
two epithelial surfaces, commonly between a
hollow viscus and the skin or between two
hollow viscera.
➢ The track is lined with granulation tissue
which is subsequently epithelialized.
➢ Fistulas are usually caused by injury or
surgery, but they can also result from an
infection or inflammation.
➢ Fistulas can occur in many places like eyes,
ears, circulatory system, respiratory system,
digestive system, urogenital system, etc…
Types
I. Blind: – Fistulas having only one open
end; may also be called sinus tracts.
II. Complete: – Fistulas having both
internal and external openings.
III. Incomplete: – Fistulas having an
external skin opening that does not
connect to any internal organ.
FISTULA – IN – ANO
➢ Fistula-in-ano is an inflammatory track which
has an external opening in the perianal skin
and an internal opening in the anal canal or
rectum.
➢ Anal fistula is a chronic abnormal
communication track between the epithelial
surfaces of the anal canal and usually the
perianal skin.
➢ The track is lined by unhealthy granulation
tissue and fibrous tissue.
➢ An anal fistula commonly occurs in the
people with a history of anal abscesses.
➢ They can form when anal abscesses do not
heal properly.
➢ Anal fistula originates from the anal glands,
which are located between the external and
internal anal sphincter and drain into the anal
canal.
➢ If the outlet of these glands becomes
blocked, an abscess can form which can
eventually extend to the skin surface.
➢ Abscesses can recur if the fistula seals over,
allowing the accumulation of pus.
➢ It can then extend to the surface again,
repeating the process.
Epidemiology
➢ Fistula-in-ano is one of the most common
anorectal disease.
➢ The prevalence is greater in men than
women, with a rate of 12.3 cases/100,000
and 5.6 cases/100,000, respectively.
➢ The average age at diagnosis is 38 years,
with most occurring between 20-40 years of
age.
Causes
➢ Risk factors for anal fistula development
includes obesity, diabetes, smoking,
hyperlipidaemia and a sedentary lifestyle.
➢ Other causes could be :-
a. The fistula usually originates from a
perianal abscess in the intersphincteric
space of the anal canal from infection of
the anal gland. Due to the tone of the
internal sphincter the duct cannot aptly
discharge the contents of the gland. Stasis
and secondary infection lead to abscess
formation from the anal gland in the
intersphincteric region. From here the
internal opening travels through internal
sphincter to open into the anal canal and
the abscess usually tracks down and
opens in the perianal skin externally, thus,
fistula-in-ano is formed.
b. Ulcerative colitis.
c. Crohn’s disease.
d. Tuberculosis.
e. Colloid carcinoma of rectum.
Classification
➢ Broadly, anal fistula can be divided into two
groups, low level fistula and high level fistula,
depending on whether the internal opening is
below or above the anorectal ring,
respectively.
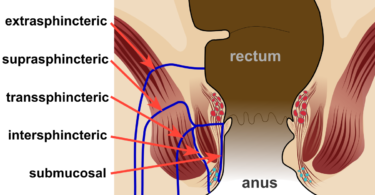
1) LOW LEVEL FISTULA: – This fistulae opens
into the anal canal below the anorectal
ring. These can be subdivided into :-
• Subcutaneous type
• Sub mucous type: – Pass superficially
beneath the submucosa and do not
cross either of the sphincter muscles.
• Intersphincteric type: – This fistula
penetrates through the internal
sphincter and opens very close to
anus.
• Transphincteric type: – This fistula
begins between the internal and
external sphincter muscles or behind
the anus, crosses the external
sphincter muscle and opens an inch
more away from anus. These may
take a ‘U’ shape and form multiple
external openings. This is termed as a
‘Horseshoe fistula’.
• Suprasphincteric type: – The fistula
penetrates through the internal
sphincter and then extends superiorly
in the plane between the sphincters
before extending to the perineum and
opens an inch or more away from the
anus.
2) HIGH LEVEL FISTULA: – These fistulae
opens into the anal canal at or above the
anorectal ring. These can be subdivided
into :-
• Extrasphincteric or Supralevator type:-
This fistula is very rare. It forms a
connection from the rectum to the
perineum that extends laterally to the
internal and external sphincter. It
begins at the rectum or sigmoid colon
and proceed downward through the
levator ani muscle and open into the
skin surrounding the anus. These can be
the most difficult to treat due to the
need to preserve the sphincter
complex.
• Pelvi-rectal fistula.
➢ The importance of deciding whether a fistula
is a low or a high level fistula type, is that a
low level fistula can be laid open without fear
of permanent incontinence as the anorectal
ring or sling is not disturbed.
➢ Whereas, in case of high level fistula one
must diagnose the case before operation and
it is usually treated by stages, least damage to
the anorectal ring may cause permanent
incontinence.
Clinical features
➢ Anal fistula per se do not generally harm, but
can be very painful and can be irritating
because of the drainage of the pus.
➢ Past history of perianal abscess can be
received.
➢ The abscess formed and ruptured by itself,
the condition healed leaving a tiny discharging
sinus.
➢ After few months, again abscess is formed,
ruptures by itself and discharging opening
left.
➢ After a few recurrent attacks the discharging
fistula fails to heal and continues to discharge.
➢ Similarly new abscess may form to cause
multiple fistulae.
➢ Additionally, recurrent abscesses may lead to
significant short term morbidity from pain and
importantly, create a starting point for
systemic infection.
➢ More common is solitary fistula with an
external opening within 3.7 cm of anus.
➢ Anal fistula can present with the following
Symptoms :-
• Pain.
• Swelling.
• Tenderness.
• Fever.
• Unpleasant odour.
• Pruritis ani.
• Skin maceration.
• Pus, serous fluid and/or faeces discharge
can be bloody or purulent.
Examination
1) Rectal examination
• The internal opening must be felt by
digital examination.
• If it is above the anorectal ring, it is a
high level fistula and the treatment is
different from low level fistula.
• Number of internal opening must be
noted.
• Even if there are multiple external
fistulae there may be one internal
opening.
2) Proctoscopy
• It is sometimes necessary to visualise
internal opening of the fistula.
3) Lipiodal injection
• It is given in the external opening, prior
to radiography, will show the track of
fistula-in-ano.
4) Chest x-ray
• To exclude tuberculosis is important as,
fistula-in-ano is often associated with
tuberculosis.
Diagnosis
➢ Diagnosis is done by examination, either in an
outpatient setting or under anaesthesia.
➢ The fistula may be explored by using a fistula
probe.
➢ In this way, it may be possible to find both
openings.
➢ The examination can be an anoscopy.
➢ Diagnosis may be aided by performing
fistulogram, proctoscopy and/or
sigmoidoscopy.
POSSIBLE FINDINGS
1) The opening of the fistula onto the skin
may be observed.
2) The area may be painful on
examination.
3) There may be redness.
4) Discharges may be seen.
5) An area of induration may be felt, due
to chronic infection.
Treatment
➢ The treatment of an anal fistula depends on
the location of the fistula as well as
precipitating factors.
➢ Most fistulas are treated surgically, through a
variety of different procedures depending on
external and internal sphincter involvement.
➢ Complex fistulas, particularly those caused by
crohn’s disease, are treated medically.
➢ Definitive treatment of a fistula aims to stop
it recurring.
➢ Some of the treatments are as follow :-
1) Suprasphincteric fistula requires treatment
of the primary condition and the fistula is
ignored. Any attempt to lay open the fistula
will cause incontinence.
2) Transphincteric fistula with a perforating
secondary tract: – The lower track is opened
as usual and the upper track opening is
made wide with scraping the high fistula
with Volkmann spoon. The upper track will
heal by itself along with the low fistula.
3) High intersphincteric fistula is also treated
in the similar fashion.
4) Gabriel’s two stages operation.
5) Fistulotomy.
6) Endorectal advancement flap.
7) Seton placement.
8) LIFT [Ligation of Intersphincteric Fistula
Tract].
9) Fibrin plug and glue.
10) MEDICAL MANAGEMENT
• Antibiotics are often unnecessary in the
setting of an uncomplicated and
drained rectal abscess.
• Medical management should be
considered in the patients of crohn’s
disease.
• Infliximab, a TNFa monoclonal antibody
has demonstrated a fistula closure rate
of 36% following 54 weeks of
treatment.
• If medical treatment is unsuccessful, a
staged fistulotomy may be necessary.
Homoeopathic treatment
1) Berberis Vulgaris
• Berberis vulgaris works well in
the cases where there is a
shooting pain around the anus.
• In addition to this, a stitching
pain around the anus also points
towards the use of berberis
vulgaris.
• The skin around the anus is very
sore in such patients and is
accompanied by itching. The itch
is mostly worse in the evening.
2) Calcarea Fluorica
3) Calcarea Phosphorica
• Patients have chest symptoms
alternating with anal fistula.
• Painless anal fistula.
• There is blood and pus discharge
from anal fistula.
• These discharges can be
accompanied by warm or burning
sensation around the anus.
4) Calcarea Sulphurica
• Anal fistula with thick and yellow
discharge.
• Discharge is often purulent and in
some cases, blood may also
appear.
• Pain is prominent in anal region.
5) Kalium Phosphoricum
6) Natrium Muriaticum
7) Natrium Sulphuricum
8) Silicea Terra
• Anal fistula with copious pus
discharges and sometimes blood
may be present in the purulent
discharge.
• Discharges are highly offensive
and putrid smelling.
• Discharges accompanied by
perianal swelling.
• Silicea is also used to treat
hardness/indurations left around
the anus after the healing of an
anal fistula