A Stubborn Case of Lipodermatosclerosis- A Case Report
Abstract:-
Lipodermatosclerosis refers to bound down, hard, sclerotic change in the skin of the lower legs due to chronic venous insufficiency leading to chronic inflammation and fibrosis. A 68-year-old Non-diabetic, Non- Hypertensive male patient reported to Outpatient department of JIMS Homeopathic medical college and Hospital with complaints ulceration and blackish discoloration on the right foot since 3 months which was a flareup episode where the patient suffers with similar episodes atleast twice a year for past 30yrs and takes allopathic medication which resolves and recurs again, lastly resorted to split-thickness skin grafting (STSG), for which patient turned up for Homoeopathic treatment. Now, The patient came with swelling over the right foot with discoloration and oozing of watery discharge along with itching and numbness sensation, dragging type of pain. Remedy was prescribed based of symptoms and general management was advised. The condition was improved in a consecutive follow-ups
Key words:- Lipodermatosclerosis, Homeopathy, Chronic Venous Insufficiency
Introduction:
LIPODERMATOSCLEROSIS (LDS) is a common form of chronic panniculitis associated with chronic venous insufficiency. This inflammatory condition of the skin and subcutaneous tissues affects the lower third of the leg and is because of sustained ‘congestion’ resulting due to high interstitial fluid and venous pressures.1
Lipodermatosclerosis is a complication of severe chronic venous insufficiency that results from high venous pressure and resulting increased capillary permeability, perivascular fibrin cuffing, and tissue hypoxia. These events culminate in fibrosis and membranous fat necrosis. Lipodermatosclerosis can present as painful, red, indurated plaques that may be easily misdiagnosed as cellulitis, thrombophlebitis, and morphea.2
Huriez et al. were the first to recognize and describe LDS in 1955 .They called it Hypodermitis sclerodermiformis (HS) and believed that the disease was caused by cellulitis in patients with venous insufficiency. Cantwell et al. believed that acid-fast microorganisms played role in the pathogenesis of this condition for which they used the terms pseudo scleroderma as well as Hypodermitis sclerodermiformis (HS).3
CLINICAL PRESENTATION OF LDS: CLASSIFICATION
It is currently accepted that LDS forms a part of pathological progression of venous disease that ultimately results in skin ulceration. An international consensus committee on chronic venous disease proposed the CEAP Classification system based on the increasing severity of venous disease.
- The clinical part of the classification grades patients from those with no visible evidence of venous disease (class I), to those with superficial varicose veins without (class II) or with edema (class III) to patients with skin changes including LDS (class IV), healed ulcers (class V), and active venous ulceration (class VI).3
LDS is divided clinically into two stages: acute and chronic. The pain is mostly pronounced in the medial leg above the medial malleolus. The area is red to violaceous, scaling, tender, and warm. At this stage some induration is already present although the affected area is diffusely involved. The sharp demarcation of the induration noted in chronic LDS may be absent.
- This acute stage is usually misdiagnosed as cellulitis, phlebitis, inflammatory morphea or erythema nodosum, and other forms of panniculitides. It is therefore suggested that well-demarcated, indurated, exquisitely tender “cellulitis” that involves the lower legs, should prompt the clinician to consider a diagnosis of LDS. The chronic phase most often develops following the acute phase (in months or even more than a year) or may occur independently as hyperpigmented thick, hard, tight, and contracted skin, in the lower third of the patient’s leg. Skin tightening may eventually lead to constriction of the ankle region giving the leg the characteristic “Inverted champagne bottle” appearance. It should be noted that patients with classic chronic LDS may develop acute onset of pain and represent an “acute on chronic” form of LDS.
- The chronic phase of LDS is considered as the stage preceding the ulceration. Kirsner et al. proposed that the degree of skin induration associated with LDS directly relates to subsequent breakdown and ulceration. Ulceration rate associated with LDS has been estimated to be around 13% in a recent retrospective analysis. Furthermore, the degree of skin thickening associated with LDS around an ulcer has been found, in at least one study, to be predictive of difficulty healing.
In a combined retrospective and prospective study the lipodermatosclerotic skin area was excised in 7 non-healing venous ulcers and then covered with split skin graft4. The study indicates that excision of the lipodermatosclerotic skin area followed by split skin grafting can accomplish healing in non-healing venous leg ulcers that have failed to respond to previous superficial venous surgery4.
CASE REPORT:-
CHIEF COMPLAINTS:-
A 68-year-old male patient previously working as Auto-driver with a habit of Smoking reported to OPD on 18/09/2024 with complaints
- Ulceration and Blackish discoloration on the right foot since 3 months.
- Pain in both knees on & off since 20 years
HISTORY OF CHIEF COMPLAINTS:-
The patient developed gradual swelling of the right limb with discoloration and gradual progressing to ulcer formation over Right foot after Scratching and peeling of superficial layers of skin with oozing of watery discharge along with itching and numbness sensation in the whole limb, and no burning. Now using herbal medicines for one month with no significant relief.
He also suffers from pain in both knee joints on and off since 20 years which aggravates walking, standing with mild stiffness of knee joints on 1st movement, Early morning.
PAST HISTORY
- Recurrent Acute-on episodes of either of the both legs (leading to ulceration of foot) since 30 years. Uses allopathic medication for the complaints, gets resolution in 30-45days with a recurrence ( once in 4-5 months).
- N/K/O HTN, DM.
PHYSICAL GENERALS
Appetite:- satisfactory
Thirst:- normal,2L/day
Bladder:-clear, no burning
Bowel :-regular, soft stools
Sleep:- Disturbed due to pain
Perspiration:- Profuse on face
LIFE SPACE INVESTIGATIONS:
Hails from lower Middle class family, didn’t have specific interest in studies, started his occupation as an auto-driver, married, has 4 children – 3 Daughters and 1 Son. Made his Children study well and settle in good professions. Readily speaks with all, probes into others personal matters gives advises if he knows or else seeks information he wanted. He quit smoking 20yrs back for his health. Joined Heartfullness Society 10-15yrs back, practises meditation. On observation, obeys to higher officials and scolds the people whom he feel inferior to him. Gets anger easily on least contradiction. Boasting Nature.
ON EXAMINATION:-
Ulcer examination :-
- Hyperkeratosis appearance of skin with inflammation of right foot was noted
- Thick debris cleared off with difficulty exposing irregular ulcer beneath with minimal slough & ulcers in webs of toes
- Multiple, irregular ulcers on the right dorsum of foot allover measuring 4 x 3 cms( widest ones).
- Tiny ulcers 1 x 1 cm with prominent depth, 2cms punched out with slough underneath.
Musculo-skeletal system examination:-
- Inverted champagne bottle-shaped noted in both legs with discoloration in lower 1/2 th of both legs.
- Varicose ulcers noted on bilateral foot with blackish discoloration of bilateral foot.
- Pitting oedema present – B/L
On 18/09/2024
Complete blood count:- HB -13.8gms%, PCV-38.4vol%, TOTAL RBC-4.5mill/cumm ,Platelet count-3.6 lakhs/cumm, Total WBC-7,600cells/cumm, D/C-N 51, L 34. E 06, M 09, B 00.
ESR-14mm
FBS-106mg/dl, PLBS-117mg/dl, HBA1C :- 5.4, Average blood glucose-107.93mg/dL
S creatinine 1.1mg/dl, blood urea 22g/dl, BUN 10.1mg/dl, Uric acid 6.8mg/dl, BUN/Creatinine ratio 9.2
C reactive protein- 12.5mg/L
PRESCRIPTION:-
On 18/09/2024, Lyco 0/1 OD, Sac lac BD was prescribed
Aspetic Dressing with Calendula Q and Echinacea Q
Foot elevation was advised
Advised to stop herbal medication
FOLLOWUP:-
| DATE | SYMPTOMS | REMEDY PRESCRIBED | |
|---|---|---|---|
| 19/09/2024- 4/10/24 | Numbness in the ulcer site on right foot & whole limbItching around the wound is reducedKnee joints < walking O/E:-No slough formation Healthy granulation noted with multiple irregular ulcers are seen.Measurements; leg circumference- Right 42cms, left 40cms ( 15 cms from knee joint)Appetite-good, thirst-normal , bowels:- regular, sleep disturbed | Lyco 0/1 ODSac lac BDAdvise for foot elevationAseptic dressing with calendula Q and echinacea Q | |
| 05/10/24 | Itching at Right foot & numbness– decreasedPain in both knee -betterPatient experiencing pain in foot on dressingNo other complaintsO/EUlcer on Rt.foot healed except at Base of great toe-irregular borders with 2cms x 2cms approximatelyOedema right 39cms,left 39cms( 15cms from base of knee)Right 39cms ,left 36cms(20cms from base of knee) | Lyco 0/1 ODSac lac BDAdvised for foot elevationAseptic dressing with Calendula Q and Echinacea Q Advise Physiotherapy daily (for improving circulation in lower limbs) | |
| The patient was left on sac. Lac with no dressing in between, then came an acute-on episode with fever. | |||
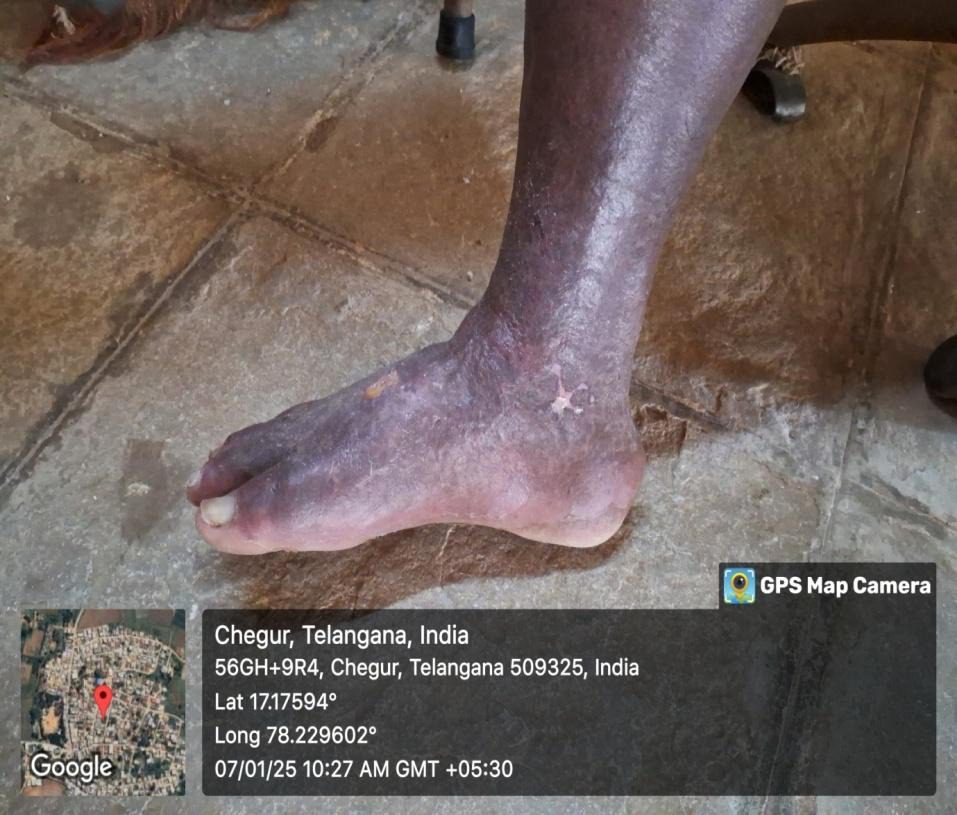
| 28/11/24 | Itching and burning at right leg with fever & chillsDry and flaky around ankles and at wound area and at lower 1/3rd of Right limb.O/E: Temp-100 F (A)Warmth noted on right leg with Enlarged femoral Lymph nodes.Hyperkeratosis on dorsum of Right foot, oozes marked around the ankles, scabs tough with cracks in between like Honey comb appearance.INVESTIGATIONS:-AEC-0.3 Pictures during Acute Flare-up | Graphites 200-ODSac lac BDAdvised foot end elevation | |
| 29/11/24 | Itching and burning at foot >+, feverish feeling +O/E: Temp- Afebrile; Enlarged femoral Lymph nodes. Warmth of leg reduced.Easily falling of scabs on foot exposing irregular ulcers | Graphites 200-ODSac lac BDAdvised foot end elevation | |
| 30/11/24 | Itching of foot decreasedPain at right foot increasedFeverish feeling reducedO/E: Scabs fell off from right foot exposing irregular multiple ulcers underneath Oozing and offensiveness.femoral Lymph nodes- Normal. | Graphites 200-OD Sac lac BDAdvised foot end elevation | |
| 14/12/24 | Itching at right foot increased with dragging type of painO/E: Pitting oedema presentlesion on right dorsum of foot and medial malleolus with mild oozing, sour smell (which permeates whole room)Rest of the areas are cracked with scabs. | Psorinum 200- one dose- powder dose in half cup of water / 15daysSac lac BDAdvised foot end elevation | |
| 7/1/25 | Ulcer sinked off leaving 1*1 cm at dorsum of center of right foot-rest of skin normal.O/E:-Pedal oedema – reduced.Right leg 39cms, left leg 37.5cms ( 15cms from patella)Right leg 36cms ,left leg 33cms(20cms from patella)Oozes at centre of dorsum of foot | Sac lac 1p/Hs/WklyAdvised weight reduction.Compressive Leg Stocking | |
| 13/5/25 | No ulcers or oedema on foot | Sac lac 1p/Hs/WklyAdvised weight reduction.Compressive Leg Stocking | |
| 21/10/25 | No further acute episodes or recurrence | Sac lac 1p/Hs/WklyCompressive Leg Stocking | |

Discussion: Patient reported to us after a well established advance stage of the Disease with an acute Flare-ups often. In such cases, we can visualise two phases of the Disease, one being the chronic phase with Acute on Chronic in between. The Patient addressed us on the chronic phase of the disease, start with a constitutional remedy and the base of the Disease-Poor Circulation with LYCO 0/1 for daily repetition in advanced cases. Then, he established his sensations in the foot and appreciated the burning sensation in the foot post dressing which were absent at the beginning. Then, an acute flare-up episode came with fever with chills, inflammation of whole limb & lypmhadenopathy- Graphites 200 was prescribed based on characteristic Symptoms, managed the acute episode, followed up by Psornium 200 (based on characteristic Smell of the ulcer) which dried the secretion and ulcer was healed. Thus, Phase of the Disease and seat of the Disease are important in handling the cases.
CONCLUSION: In clinical practice, Homoeopaths frequently encounter challenges in managing such cases, as patients often present at an advanced stage after exhausting other therapeutic modalities, usually as a last resort, with an expectation of rapid relief. Despite these limitations, homoeopathy has demonstrated clinical efficacy in several instances, even under such adverse circumstances, by facilitating gentle, safe, non-toxic intervention and sustained restoration of health.
The present case illustrates the effective management of an acute exacerbation, wherein timely homoeopathic intervention not only alleviated the acute symptoms but also significantly reduced the recurrent tendency. Prior to treatment, the patient experienced episodic exacerbations at intervals of approximately 4–5 months. Following the administration of indicated homoeopathic medication, the patient remained asymptomatic for a follow-up period of 10 months, suggesting a favorable long-term outcome.
Reference:-
1.Nishant A Tambe, Epidemiological Study of Lipodermatosclerosis, J Res Med Dent Sci, 2021, 9(7): 403-405
2. Fallahzadeh, M.K., Khalesi, M., and Namazi, M.R. (2010) Lipodermatosclerosis: a commonly misdiagnosed complication of chronic venous insufficiency. TheScientific World JOURNAL 10, 576–577. DOI 10.1100/tsw.2010.60.
3. Lipodermatosclerosis Maria Miteva, Paolo Romanelli &Robert S. Kirsner dth_1338 375..388 Department of Dermatology and Cutaneous Surgery, University of Miami Miller School of Medicine, Miami, Florida,©2010Wiley Periodicals, Inc. DERMATOLOGIC THERAPY,Vol. 23, 2010, 375–388, ISSN 1396-0296.
4. Ahnlide I, Bjellerup M, Akesson H. Excision of lipodermatosclerotic tissue: an effective treatment for non-healing venous ulcers. Acta Derm Venereol. 2000 Jan-Feb;80(1):28-30. doi: 10.1080/000155500750012478. PMID: 10721829.
5. Allen H C. keynotes and characteristics with comparisons of some of the leading remedies of the materia medica, 8th edition. New delhi . B. Jain Publishers(P) ltd.2006.
6. Boericke W,2018, New manual of Homoeopathic Materia medica with Repertory, 3rd revised and augmented edition, B Jain publishers p ltd., New Delhi.
7. Hahnemann S. Organon of Medicine. 5th Edition with Additions & Alterations of Sixth Edition translated by William Boericke. New Delhi,India: B Jain; 6th impression 2011.
About the Authors
Dr. Y. Ramanujaneyulu (Prof., HOD, Dept.Of Organon, JIMS Homoeopathic Medical college & Hospital)
Dr. M. Ramya Krishna( Assistant Professor, Dept. Of Paediatrics, JIMS Homoeopathic Medical college & Hospital)
Dr.Likhitha Thotha, (PG Scholar, Dept. Of Paediatrics, JIMS Homoeopathic Medical college & Hospital)