
Abstract: Pruritus vulvae (vulval itch) is a common gynaecological condition with innumerable causes that can cause immense pain and embarrassment for those affected, with a negative impact on quality of life. Despite its high prevalence, it is challenging to reach an accurate diagnosis. A thorough history and examination are crucial to providing effective treatment. 1
Keywords: pruritus vulva, homoeopathy.
Definition: In Latin, pruritus means itch, and vulvae mean the external female genitalia (includes the clitoris, the vaginal orifice, mons pubis, and the labia on both sides). Itch on the external female genitalia is a symptom and not a pathological diagnosis. It affects about 1 in 10 women during their lifetime. Pruritus vulvae is caused by various factors as follows:
Etiological classification of pruritus vulvae:
Pruritus vulvae have multiple etiological causes as listed below, and a full investigation should be undertaken:
- Dermatological: The International Society for the Study of Vulvar Disease (ISSVD 2006 classification) along with hidradenitis suppurativa
- Infections and Infestations: candidiasis-vulvovaginal, trichomoniasis, bacterial vaginosis, Herpes simplex, pubic lice (Phthirus pubis), scabies (Sarcoptes scabiei hominis), and thread worm (Enterobius vermicularis).
- Neoplastic conditions Squamous: VIN usual type (Warty, Basaloid, Mixed), VIN
- Differentiated type Non-squamous: Paget’s disease, tumors of melanocytes
- Hormonal: atrophic vaginitis, breastfeeding Urinary or fecal incontinence
Systemic Causes: secondary to renal (chronic renal failure), Hematologic (iron deficiency, polycythaemia rubra vera, hypereosinophilic syndrome, essential thrombocythemia, myelodysplastic syndrome), Hepatic (Cholestasis), endocrine (Thyroid and Parathyroid Disorders, Diabetes mellitus), malignancies (Hodgkin’s disease, leukemia, carcinoid syndrome), and immunosuppression leading to vulvovaginal candidiasis
Psychosexual disorders
Others: pubic hair regrowth after shaving.
Causes of Pruritus vulvae in various age groups:
- Females in prepubertal age: poor hygiene, Streptococcal infection, Escherichia coli infection, pinworms, scabies, and allergic contact dermatitis.
- Females in reproductive age: vaginitis, allergic contact dermatitis, hidradenitis suppurativa, lichen simplex chronicus.
- Postmenopausal Females: Atrophic vaginitis, lichen sclerosus, vulvar cancer, Paget’s disease, females with diabetes mellitus, candidiasis, and illnesses caused by dermatophytes.
Pathophysiology of pruritus vulvae:
Pruritus vulvae can present as an acute or chronic condition. The sensation of pruritus is transmitted through C fibers to the dorsal horn of the spinal cord to the cerebral cortex via the spinothalamic tract. Pruritus generates a spinal reflex response, the scratch, which is as innate as a deep tendon reflex. Pruritus is often exacerbated by skin inflammation, dry or hot ambient conditions, skin vasodilatation, and psychological stressors.
The mechanisms in acute presentation vary depending on the underlying pathophysiology. Some examples include:
1) Histamine released by mast cells in allergic dermatitis
2) Cytokines and immune-mediated pro-inflammatory agents are involved in atopic vulvitis.
3) Nerve paraesthesia in Herpes simplex
4) Serotonin-mediated pruritus occurs in polycythaemia vera, uraemia, cholestasis, and lymphoma.
Women with pruritus vulvae are quite often present with symptoms that are not always specific to one clinical diagnosis, and new symptoms may appear over time.
Most patients are managed in a primary care setting. Referrals to secondary care (specialist vulval clinic) are recommended in the following circumstances:
1) No obvious cause has been identified.
2) Poor response or persistence of symptoms to preliminary treatment.
3) Premalignant conditions: review of suspicious lesions like unexplained vulval lump, ulceration, or bleeding
4) Suspicion of malignancy: suspected cancer pathway referral within 2 weeks
It is advisable to make a secondary referral for professional opinion for additional investigation, biopsy, or treatment guidance.
Gynecological history should include eliciting the duration of presenting symptoms, severity, impact on quality of life, and any past or present treatment. A detailed history of treatment taken is important as it will influence future treatment plans. Information regarding personal or family history of autoimmune conditions, atopic conditions, urinary or fecal incontinence, smoking, and cervical smear abnormalities is highly significant. The clinician should also inquire about the impact of symptoms on social, psychological, and sexual life. A full examination of the anogenital region and other skin and mucosal sites should be done.
Investigations for thyroid disorders, diabetes, and sexually transmitted diseases should be considered.
Skin patch testing could be performed for women seen with vulval dermatitis in a general gynecology clinic. A vulvar biopsy is indicated if there is a suspicion of VIN or is no response to first-line treatment in a general gynecology clinic.
General advice should be provided at every initial consultation to any patients with vulval symptoms.
Fewer than 5 in 100 women (5%) with pruritus vulvae if diagnosed with lichen sclerosus or lichen planus might develop vulval cancer. Chronic itch can be debilitating psychologically, sexually, and socially. Women might feel embarrassed and stigmatized to talk about their symptoms. Pruritus can cause insomnia, which could lead to somnolence and further could cause occupational hazards. Itching and scratching can lead to skin breakdown and secondary bacterial infection. 2
Case Study:
A 35-year-old female complains of intolerable itching over her genitalia with no eruption for the past 3 months. She keeps on scratching. She cannot restrain herself from scratching, which aggravates her complaint. She also had a painful coition with an aversion to it. Soreness in the breast before menses, which gets relieved after the arrival of menses. In association with the main complaint, she had body aches, pain in extremities, and tenderness over the stitches of the caesarean section scar.
The patient had irritability, especially from her daughter, who asks so many questions from her every time.
Occupation: Housewife
No conventional mode of treatment was taken.
Physical General:
Appetite: 3 meals/day
Thirst: Adequate
Desire: sweets
Stool: D1, satisfactory
Urine: D4 to D5, Normal
Sweat: Generalised
Sleep: Adequate
Dreams: Nothing significant
Thermal: Chilly
Gynecological history: Menarche: at the age of 14 years
Menstrual cycle: 28±2 days
Duration: 4 to 5 days.
Obstetrical history: P2 A0 L2
Delivery: Caesarean Section
On examination
Per vaginal = no red discoloration, eruption, or swelling was seen. No discharge or odor was there.
General examination
Inspection: brown discoloration on facial skin
Prescribing totality:
Irritability from her daughter.
Desire for sweets (+++)
Thermal- chilly
Painful coition with an aversion to it
Soreness in the breast before menses
Itching over genitalia, which aggravates by scratching
Chloasma on face
Repertorial Totality
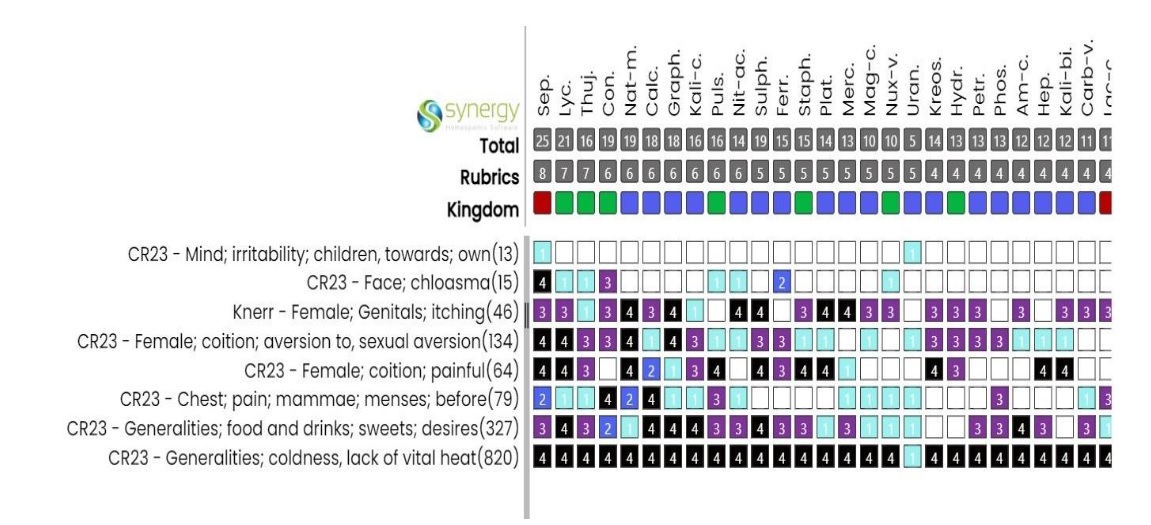
Prescription:
Sepia 200/ Single Dose/ Stat was given on 04/07/23, followed by Placebo for 4 days.
Follow Up:
08/07/23 | Improvement was seen in particulars (itching relieved) | Placebo / OD / 15 days |
21/07/23 | Relief was seen in painful coition | Placebo / OD / 30 days |
03/10/23 | Case came to stand still so medicine repeated | Sepia 200 / single dose/stat Placebo / OD / 10 days |
14/10/23 | Improvement was seen in particulars and irritability | Placebo / OD / 30 days |
11/12/23 | Case again came to stand still | Sepia 1M / single dose/ stat Placebo / BD / 30 days |
09/01/24 | Complete resolution of complaints of vulval itching and with significant relief in painful coition. | No medicine was given after that |
Discussion
Pruritus vulvae can lead to psychological distress, stigmatization, embarrassment, and insomnia and can have a negative impact on sexual function. So based on individualization, Sepia was selected and prescribed to the patient as a constitutional remedy.
Result
Sepia was given in medium to high potency, based on the totality of the patient. Marked improvement was seen in the physical state of the patient as well as in the psychological state.
Conclusion
Homoeopathic medicines based on individualization showed complete resolution of Pruritus vulvae with significant improvement in the treatment of dyspareunia. Thus, homeopathic medicines help to enhance the patient’s quality of life suffering from pruritus vulvae.
Reference
- Bansal J., Datta S. Pruritus vulvae. Obstetrics, Gynecology & Reproductive Medicine. 2019 Jun;29(6):170–4.
- Gopal G, Hadoura E, Mahmood T. Pruritus vulvae. Obstetrics, Gynecology & Reproductive Medicine. 2016 Apr;26(4):95–100.
Authors
Dr. Vaishali Vyas (MD Scholar)
Department of Homoeopathic Repertory and Case Taking.
Govt. Homoeopathic Medical College and Hospital, Bhopal, Madhya Pradesh
Co-author
Dr. Sarita Verma (I/C HOD and Guide)
Department of Homoeopathic Repertory and Case Taking.
Govt. Homoeopathic Medical College and Hospital, Bhopal, Madhya Pradesh



