Abstract
Introduction: This is a case of polycystic ovarian disease in a girl of 18 years old. The right ovarian cyst was 41 X 30 mm in size with left ovary in normal measure. Case Summary: This case was treated with individualised homoeopathy at the OPD of RBTSGHMC & Hospital, Muzaffarpur, Bihar. Homoeopathic medicine Lycopodium was given to the patient on the basis of individualistic approach. The patient improved in her presenting complaints as well as there was change in diagnostic parameters. USG declared no obvious abnormality after homoeopathic treatment. This case report suggests that a correctly chosen homoeopathic medicine can be beneficial in unusual cases.
Keywords: Homoeopathy, Lycopodium, Polycystic Ovarian Disease, Hyperandrogenism.
Introduction
PCOD Stands for polycystic ovarian disease. This is one of the most well- known hormonal problems among women of reproductive age and a main cause of sub – fertility. (1) This condition affects the ovary in women by causing cysts. This leads to a hormonal imbalance within the body by producing more male hormones than needed for women. (2)
The hormonal disproportion leads to problems in menstruation and fertility. The ovaries may produce a large number of tiny collections of fluid and fail to release eggs on a regular cycle. This is portrayed by persistent anovulation and hyperandrogenism with variable clinical indications, for example, oligomenorrhoea, inability to conceive, hirsutism and skin inflammation.(1) Patient with PCOD may have symptoms of irregular or non – existent periods, acne, weight gain, pelvic pain, high blood pressure, lower back pain, dysmenorrhea, dyspareunia & nausea. (3)
Two most common types of cysts are:(3)
- Follicle cysts- In a normal menstrual cycle, an ovary releases an egg each month & grows inside a tiny sac called a follicle. When the egg matures, the follicle breaks open to release the egg usually. follicle cysts form when the follicle (tiny sac) doesn’t break open to release the egg. This leads the follicle to continue growing into a cyst.
- Corpus luteum cysts- once the follicle breaks open & releases the egg, the empty follicle sac shrinks into a mass of cells called corpus luteum. corpus luteum cyst form if the sac doesn’t shrink instead, the sac reseals itself after
the egg is released, filling up fluid inside. Most corpus luteum cysts go away after a few weeks. They may bleed or twist the ovary and cause pain.
After detailed case taking on a standard case taking proforma, the totality of symptoms was built for patient based on mental generals, physical generals, constitution, miasmatic background, family history, previous medical history etc. as per the homoeopathic principles.
Causes
In PCOD many follicles fill up with fluid inside the ovaries. Each follicle contains an immature egg that never provoke ovulation. The absence of ovulation results in a hormonal imbalance with a high release of androgen. However, certain factors that cause to it. (2) They are:
- Genetic makeup
- Obesity
- Excess insulin
- Excess androgen
- Insulin resistance
Symptoms
Irregular menstruation– Most common signs of PCOD is irregular menstruation. Due to high amount of male hormone, the body prevents ovulation.
Heavy bleeding– Since the periods are irregular, uterine wall build up more. This leads to heavy bleeding.
Acne– Due to higher amount of male hormones, the skin secrets more oil causing more acne.
Hair growth– Most women, who suffer from PCOD, have hair growth on their face, back, stomach and chest. The condition is known as hirsutism.
Weight gain– Most women who suffer from PCOD are obese or overweight.
Crown baldness– Most women with PCOD suffer from male pattern baldness and hair become thin on crown.
Headache– headaches are triggered by hormonal imbalance.
Skin darkening– Women with PCOD experiences darkening of skin in the groin, axilla and neck region. This condition is known as acanthosis nigricans. (4)
Complications
- Infertility- PCOD causes infertility as it reduces or may be completely absent the ovulation in the body.
- Diabetes- PCOD causes insulin resistance in the body results into diabetes.
- Heart disease- PCOD increases blood pressure in the body leading to heart problem.
- Endometrial cancer- since in PCOD there is delayed ovulation, so thickening of the endometrium, the inner lining of uterus. This increases the chance of getting endometrial cancer.
- Depression– women with PCOD undergo depression due to hormonal imbalance in the Body.(2)
A CASE REPORT CASE HISTORY
An 18 years old girl reported in the outpatient department of RBTSGHMC&H, Muzaffarpur, Bihar on 09/06/2022 with a complaint of pain in right inguinal region. The patient was a known case of PCOD with a history of pain in right iliac region continue for which she underwent few investigations on physician’s advice for assessment and took conventional treatment with temporary relief. The patient did not suffer from any other major illness in the past except from gastric disturbances. Family history was also not significant.
Mental general
The patient was very well behaved. She felt anxious before performing new work but performed well once she started. She had the fear of being alone at home, though she didn’t interact with others much. She was miserly in her expenses.
Physical general
Her appetite was good and she always preferred warm food. She had the desire for sweet and spicy things with moderate thirst. She was prone to have gastric disturbance with bloating of abdomen. Sleep was usually adequate, refreshing with non-specific sleep posture and dreams. She felt heat sensation in palm. She also complained of pain in right inguinal region. Menstrual cycle was regular with scanty bleeding, her menses lasted only for 1½ days.
Diagnostic assessment
This is based upon the presence of any two of the following three criteria-
- Oligo and/or anovulation.
- Hyperandrogenism
- Polycystic ovaries.
Investigations such as ultrasonography (whole abdomen) were carried out. Post- treatment outcome corroborated with follow-up investigation with significant changes. USG revealed no obvious abnormality after 1½ months of continuous homoeopathic treatment with improvement in PCOD.
Analysis and evaluation of the symptoms:
| s.no. | symptoms | analysis | evaluation | Miasmatic analysis |
| 01. | Avarice | Mental general | +++ | Sycotic |
| 02. | Desire for company | Mental general | ++ | Psora |
| 03. | Desire for spices food | Physical general | ++ | Psora |
| 04. | Desire for hot food | Physical general | +++ | Psora |
| 05. | Moderate thirst | Physical general | ++ | Psora |
| 06. | Clotted menses | Particular | ++ | Psora |
| 07. | Scanty menses | Particular | +++ | Psora |
| 08. | Stitching pain in inguinal region | Particular | ++++ | Psora |
| 09. | Sensation of heat in hand and palm | Physical general | ++ | Psora |
Totality of symptoms
- Fear of being alone
- Expand money hardly
- Preferred warm food
- Desire for sweet & spicy things
- Clotted menses
- Menses with scanty bleeding
- Hot sensation of palm
- Stitching pain in right inguinal region
| S.no. | symptoms | Rubrics |
| 01. | Expand money very hardly | Avarice |
| 02. | Fear of being alone | Company desire for |
| 03. | Desire spicy things | Food & drink, spices, desire |
| 04. | Desire warm food | Warm food desire |
| 05. | Takes adequate quantity of water | Thirst |
| 06. | Clotted menses | Menses clotted |
| 07. | Menses with scanty bleeding | Menses scanty |
| 08. | stitching like pain in right inguinal region | Pain, inguinal region, stitching pain |
| 09. | Hot sensation of palm | heat, hands, palm |
REPERTORISATION SHEET:(5)
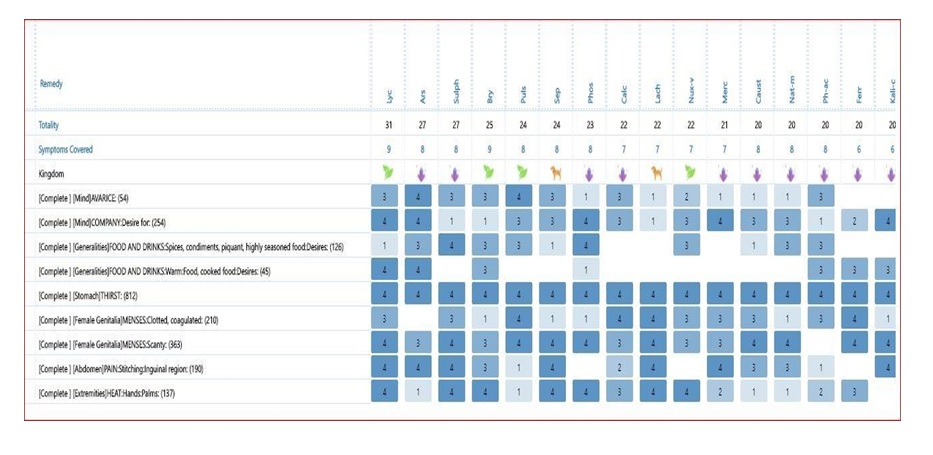
REPERTORIAL ANALYSIS
Lycopodium- 9/31
Arsenic- 8/27
Sulphur- 8/27
Bryonia- 9/25
REPERTORIAL SELECTION
As Lycopodium covers maximum numbers of rubrics and got highest marks. After consulting with Materia-Medica, Lycopodium was chosen for prescription.
THERAPEUTIC INTERVENTION
After detailed case taking on a standard case taking proforma, the totality of symptoms was built for patient based on mental generals, physical generals, constitution, miasmatic background, family history etc. as per the homoeopathic principles.
After repertorisation, the top medicines were Lycopodium, Arsenic, Sulphur, Bryonia, Pulsatilla. After carefully analysing the mental and physical generals of patient, considering the repertorial result and referring back to homoeopathic MM similimum was prescribed. Individualised homoeopathic treatment was started with single dose of lycopodium 200 followed by placebo following the law of minimum dose.
PRESCRIPTION
Lycopodium 200/1 dose was given on the first visit in empty stomach early morning.
Follow – up sheet
| Date of visit | Change in symptoms | Prescription |
| 19/07/2022 | Pain in right inguinal region relieved much | Placebo for 3 days |
| 10/08/2022 | No pain in right inguinal region and now menses with normal bleeding | Placebo for 3 days |
| 24/08/2022 | No pain in right inguinal region and menses with normal bleeding and no clots. | Placebo for 3 days |
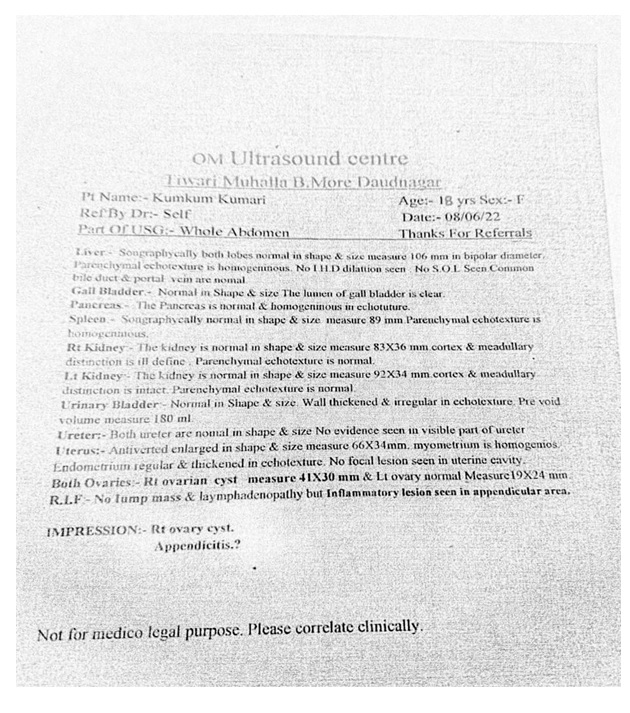
Before treatment: USG report show: Right ovarian cyst. Measure – 41*30 mm and left ovary normal in size.
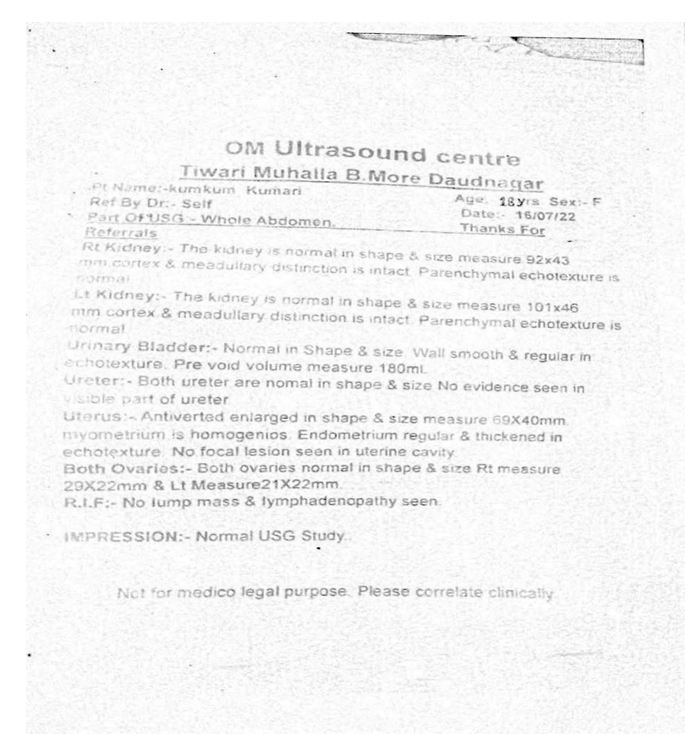
After treatment:
Normal USG study.
Both ovaries normal in shape and size.
No lump masses. No lesion seen in uterine cavity.
CONCLUSION
Homoeopathy is a specialised system of medicine. It treats the patient as a whole and not just symptoms. Homoeopathic treatment is based on individualisation, acting best to cure the disease without harming other system of body. Post – treatment USG report is a documentary evidence. This case shows a positive role of homoeopathy in treating PCOD.
REFERENCE
- Sheehan M T. polycystic ovarian syndrome: diagnosis & management. clin med res 2004 feb; 02(01):13-27;cited 2022 nov.23.
- Banerjee nikita. what is PCOD [internet]. [2022, march 23; cited 2022 nov.21].
- Available from: https://pharmeasy.in/blog/pcod-problems-know-its-symptoms-causes-and- treatment/
- Ross EK, Kebria M. incidental ovarian cysts: when to reassure, when to reassess, when to refer. Cleve Clin J Med 2013; 08:503-14;
- Dutta D C. Textbook of gynecology.#[8].new delhi:jaypee brothers medical publishers (p) ltd;2013.
- Zomeo hompath software (complete repertory), Mind technology, Mumbai.
About the author
- Dr. Vinita Kumari PGT; R.B.T.S Govt. Homoeopathic Medical College and Hospital.
- Dr. KM. Shruti Prabha PGT; R.B.T.S Govt. Homoeopathic Medical College and Hospital.