A Case Report on Impetigo Treated by Tarentula
Abstract
Impetigo is a contagious local superficial bacterial infection involving the epidermis. Impetigo affects more than 160 million children in low to middle income countries.In India, it affects 5.96% of the population of children Conventional medicine treats these cases by topical application and anti-steroidal drugs. Hahnemann said in organon of medicine that it is a criminal treasure to treat skin disease by external application. Homeopathy has a great role in treating these kinds of cases. Here I’m presenting a case of impetigo treated by Tarentula.
Case summary: This case was treated with individualised homoeopathic medicine at the OPD of RBTS GOVERNMENT HOMOEOPATHIC MEDICAL COLLEGE & HOSPITAL, MUZAFFARPUR, BIHAR. A 7-year-old child presented with a complaint of a reddish eruption around the mouth and nose which oozes out in a few days and then forms a crust. Homoeopathic medicine Tarentula was given to the patient on the basis of an individualistic approach.
Keywords: Homoeopathy, Impetigo
Abbreviations: OPD: outpatient department.
Introduction
Impetigo is a highly contagious bacterial skin infection characterized by the formation of red sores or blisters that quickly rupture and form honey-coloured crusts. This common dermatological condition primarily affects children, but it can also occur in adults. Impetigo is typically caused by either Staphylococcus aureus or Streptococcus pyogenes bacteria, which can enter the skin through cuts, insect bites, or other breaks in the skin barrier. While impetigo is not usually a serious condition, it can be uncomfortable and socially distressing for those affected, especially children. The incidence of impetigo varies geographically and temporally, with higher rates often observed in overcrowded and underprivileged communities. Factors such as poor hygiene, warm and humid climates, and close contact with infected individuals contribute to the spread of impetigo. Additionally, individuals with compromised immune systems or pre-existing skin conditions are at an increased risk of developing impetigo.
Types of impetigo
–Two forms exist: Non bullous impetigo and bullous impetigo.
Impetigo contagiosa
Etiological agents
- Staph. Aureus: in developed countries
- Strep. Pyogenes: in developing countries
- Or by both
Epidemiology
- Prevalence: common, often occurring in epidemics
- Age: preschool and young school children
Clinical Features
Morphology: Multiple, thin-walled bullae with erythematous halo, rupture rapidly to form exudative plaques covered with honey-coloured crusts Spread peripherally, without (or only partial) central healing and often coalesce to form polycyclic plaques Removal of crust reveals erosion. On drying, crust falls, leaving erythema which fades without scarring. Untreated, may evolve into ecthyma.
Distribution of lesions: Face, especially periorificially (mouth and nose), most frequent site of involvement. Extremities and scalp, less frequently.
Associations:
- Regional lymphadenopathy frequent in extensive lesions (90%).
- Constitutional symptoms occasionally
Complications:
- Eczematisation, a frequent complication.
- Acute poststreptococcal glomerulonephritis
Investigations
- Gram stain: Of exudate shows polymorphs with intracellular and extracellular Gram-positive coco in chains (streptococci) or clusters (staphylococci) or both.
- Culture: Of pus to identify etiological agent. (Stapl aureus or/and Strep, pyogenes) and also for antibiotic sensitivity.
Diagnosis
- Points for diagnosis: Diagnosis of impetigo contagious is based on:
- Age: Patient is a child.
- Morphology: Appearance of multiple, crusted (honey-coloured) lesions with an erythematous halo
Distribution: Predominantly on face (periorificial areas).
Investigation: Gram stain (Gram-positive coca in chains /clusters) and culture of exudate (Stap.aureus/and Strep pyogenes) establish etiological agent.
- Differential diagnosis; Impetigo contagiosa should be differentiated from:
Bullous impetigo | Impetigo contagiosa | |
Aetiology | Staph.aureus | Staph.aureus or strep.pyogenes or both |
Prevalence | Sporadic | Frequent, often epidemic |
Age | Usually, infants | Children |
Morphology of bulla | Bullae, thick-walled, persistent &may become large | Thin-walled & transient so seldom seen |
Erythematous halo
| Absent | Common |
Crusts | Thin, varnish-like | Thick, honey coloured |
Central clearing & shape | Present, so annular lesions seen | Absent/polycyclic plaques |
Lymphadenopathy | Rare | Frequent |
Mucous membrane
| May be involved | Rare |
Distribution | Face and another part | Periorificial |
Herpes simplex virus differentiated with impetigo contagiosa
HSV infection | Impetigo contagiosa | |
Morphology | Grouped vesicles which rupture to form polycyclic erosions | Plaque covered with honey-coloured crusts; several lesions coalesce to form polycyclic lesion |
Distribution | Around & within mouth | Periorificial |
Treatment
General measures
- Measures to prevent spread: Encouraging hand washing and early institution of treatment.
- Local hygiene: Including washing with soap and water. And removal of crusts, often after softening
- Predisposing factors: Need to be addressed.
Bullous Impetigo
Etiological agent
Staph. Aureus (group II, type 55 and 77)
Epidemiology
- Prevalence: Sporadic.
- Age: Neonates and infants.
Clinical Features
Morphology: Bullae, containing turbid fluid and minimal perilesional halo, which gets ruptured in few days to form thin, varnish-like crusts. Centre heals to form annular plaques. Mucous membranes may be involved.
Distribution: Face. Sometimes extensive lesions, often favouring sites of existing skin diseases
Complications:
- Staphylococcal scalded skin syndrome (SSSS).
Investigations
- Gram stain: Polymorphs with intra- and extracellular Gram-positive cocci in clusters.
- Culture: Staph. aureus, Important to determine antibiotic sensitivity
Diagnosis
Points for diagnosis: it can be diagnosed on the basis of:
- Age: Patient is an infant.
- Morphology: Presence of bullae, which rupture to form plaques surmounted.
- varnish-like crusts.
- Lesions heal in centre to form annular plaques.
- Distribution-face.
- Investigations: Gram stain (Gram-positive cocci in dusters) and pus culture (Staph, aureus) establish the etiological agent.
Treatment
- General measures:
- Local hygiene, cleaning hands properly.
- Crusts can easily be removed.
Homoeopathic Therapeutics
- Mezereum-Formation of thick, dry crusts on the skin. The eruptions are very itchy, and the child continually scratches them. Tearing the scab causes pain and burning sensation. child is irritable and restless.
- Antim Crud-Eruptions are covered with thick, hard, honey coloured scab, crusty eruption are painful to touch. discharges are greenish in colour. Basically, eruptions present around mouth and nose.
- Dulcamara–Crusts are surrounded by red coloured border. these bleed on scratching and ooze watery fluid or pus eruption are itchy and sensitive to touch, <washing.
- Graphitis -The chief character includes eruptions which exudate watery, transparent, sticky, gluey discharges. The eruption is firstly of light colour with itching followed by scab formation. the discharges are may be corrosive
- Hepar Sulp–Very painful, oversensitive eruption developed here. Pus filled sores on the skin. These tend to turn into ulcers, foul smelling discharges with burning and stinging pain.
- Rhus Tox -Appearance of blisters filled with yellow watery content blisters were large and appear on the corners of mouth there is burning, biting tingling stinging sensation. Marked redness on the skin. Foul smelling fluid matter.
Case History: –
A 7 years old, Hindu male child reported in the paediatrics outpatient department of RBTS Government Homoeopathic Medical College & Hospital, Muzaffarpur, Bihar on 04/12/2023 Complaint of eruption around mouth and nose, crusty, yellowish brown in nature
Child is physically very restless and obstinate as well. Loves music and dancing.
Past History –Abdominal colic before 1 year for which he has taken allopathic medicines.
Family history–
Mother- Father – Alcoholic
Personal history – student
Physical General
- Outlook-lean and thin
- Tongue-moist
- Thirst – 1-2 Liter
- Appetite – good
- Perspiration – normal
- Thermal – hot
- Desire – sweet
- Aversion – Not specific
- Stool- constipation
- Urine -clear
- Sleep – Sound
- Dream – Not specific
- Physically patient was very restless
Mental general
Loves music and dance
Provisional diagnosis– Impetigo

Totality of symptoms
- Eruptions around mouth and nose
- Eruption crusty yellowish -brown in nature
- Sore eruption
- Loves music and dance
- Desire cold foods and drinks
- Patient is physically very restless.
Analysis And Evaluation of Symptoms with Miasmatic Analysis
S.No | SYMPTOMS | ANALYSIS | EVALUATION | MIASMATIC ANALYSIS |
Eruptions around mouth and nose | particular general | ++ | Psora | |
Eruption crusty in nature | physical general | ++ | Syphilis | |
3. | Sore eruption | physical general | ++ | Psora |
4. | Patient loves music and dance | mental general | +++ | Tubercular |
5. | Desires cold foods and drinks | Physical general | + | Syphilis |
6. | Physical restlessness | physical general | ++ | Psora |
Symptoms Converted into Rubrics
SYMPTOMS | RUBRICS |
Impetigo | FACE-ERUPTION-impetigo |
Soreness | GENERALS-PAIN-Sore |
Desires cold foods and drinks | GENERALS-FOOD AND DRINKS-cold food and drink |
Physical restlessness | GENERALS-RESTLESSNESS |
likes music and Dance | MIND-EXCITEMENT -music from |
Repertorization sheet
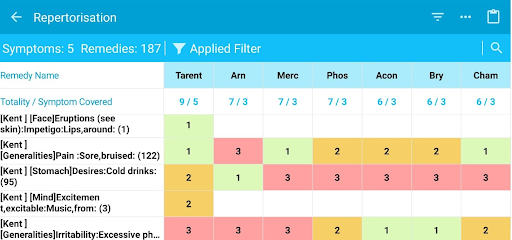
Repertory Used– Kent Repertory
Repertorial analysis: –
Tarentula: – 9/5
Arnica- 7/3
merc- 7/3
Phos. – 7/3
Aconite: – 6/3
Repertorial selection:
As TARENTULA covers maximum numbers of symptoms and got highest marks. After consulting with Materia-medica, tarentula was chosen for prescription.
Therapeutic intervention:
After proper case taking, the totality of symptoms were made based on mental generals, physical generals, constitution, miasmatic background, past history etc. according to homoeopathic principles.
After carefully analysing the mental and physical generals of the patient and considering the repertorial result, referring back to homoeopathic MM, a similimum was prescribed. Potency is selected as per susceptibility of the patient Individualised homoeopathic treatment was started with four doses of tarentula 30 BD for 2 days. (7)
Prescription
Tarentula 30 twice a day x 2 days
Rubrum 30/1dramch /bd
FOLLOW UPS
DATE OF VISIT | CHANGE OF | MEDICINE/ DOSE |
SYMPTOMS | /POTENCY | |
06/12/2023 | Slight aggravation was seen in the eruptions | Placebo |
19/12/2023 | Soreness get reduced | Placebo |
27/12/2023 | Standstill condition, eruption with oozing discharges | Tarentula 200/2 dose od |
10/01/2024 | All eruptions disappeared, appearance of normal skin | Rubrum |
Conclusion:
Here from this case, I concluded the efficacy of individualized homoeopathic medicine as a holistic treatment in case of impetigo. The conventional therapeutics for impetigo are application of topical steroids and immunosuppressants which may be related with various side effects, with limited relief only .so it is necessary to promote homoeopathy in treatment of such cases and further researches should be needed to emphasize the efficacy of homoeopathic medicine in impetigo complains.
References
- Behl P.N. Aggarwal A. Srivastava Govind. Practice of Dermatology. Tenth edition. CBS publishers and Distributors.2015
- Khanna, Neena. Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases-E-book. Elsevier Health Sciences, 2013
- Kent, James Tyler. Repertory of the homoeopathic Materia medica. B. Jain Publishers, 1992
- Boericke, William. Pocket Manual of Homoeopathic Materia Medica & Repertory: Comprising the Characteristic and Guiding Symptoms of All Remedies (clinical and Pathogenetic symptoms) Including Indian Drugs. B. Jain publishers, 2002.
- Allen H.C. Keynotes and characteristics with comparisons of some of the leading remedies of the Materia medica with bowel nosodes. B. jain publishers,2008
- Sherr Jeremy .Firefly Prime Repertory App. Kent repertory
- Dudgeon RE. Lectures on the theory and practice of homoeopathy. B. Jain Publishers; 2003.
Author
Dr. Jiya Kumari, (PG Scholar), Dr.Narendra Kumar (PG Scholar) Department of pharmacy
R.B.T.S. Govt Homoeopathic Medical College and Hospital Muzaffarpur, Bihar Email: [email protected]