
ABSTRACT: –
PCOS is a hormonal-related disease. It is mostly found in patients in the child-bearing age group. Women suffering from PCOS may have uneven or prolonged menses and amenorrhea. In these women, unneeded male hormones (androgen) are found.
In this article, there is a case of 21 years female who was suffering from PCOS. She was treated within 6 months with a single constitutional homoeopathic medicine SEPIA OFFICINALIS 200, SEPIA OFFICINALIS 1M with repetition as per requirement.
Method – A detailed case taking was done and PCOS was diagnosed based on clinical examination, physical examination, and ultrasonography report.
A constitutional homoeopathic remedy was prescribed based on complete symptoms with aid of repertorization.
Result– The patient recovered remarkably with homoeopathic therapy.
KEYWORDS: – Constitutional homoeopathic medicine, polycystic ovarian disease, Sepia officinalis.
Abbreviations: Congenital adrenal hyperplasia (CAH), polycystic ovarian syndrome (PCOS), transvaginal sonography (TVS), luteinizing hormone (LH), follicle stimulating hormone (FSH), ultrasonography (USG), outpatient department (OPD),TDS – thrice a day
INTRODUCTION
This condition is also called Stein Leventhal Syndrome.[1] Polycystic ovary disease is a hormone-related disorder. Females who are suffering from PCOS have more androgen levels.[2]
Patients who suffer from this disease usually have uneven menses or none at all.[3]
It’s associated with a higher rate of depression and anxiety [4]. There are many causes of this disease, which is made from the male hormone of the ovary. Mostly these symptoms occur =
Anovulation, high androgen levels, multiple cysts.
There are other causes, some are listed below: –
CAH, thyroid dysfunction, elevated prolactin, Cushing’s syndrome
The incidence of the disease is 5-4 percent, it mostly occurs in infertile ladies. Multiple cysts in ovaries can be seen in 20% of healthy women. And this disease occurs in 20-30 percent of the childbearing age group.
Clinical signs:
1. weight gain increases rapidly
2. Menses problems — May be oligomenorrhea, amenorrhea, or DUB and infertility.
3. facial acne
4. excessive growth of unwanted hair
5. Acanthosis nigricans. In this problem, the skin is thickened and pigmented. The most commonly affected areas are the back of the neck, inner thighs, groin, and armpits.
5. HAIR-AN syndrome< hyperandrogenism, insulin resistance, and acanthosis nigricans>.
DIAGNOSIS CRITERIA:-
Rotterdam criteria—-
According to the Rotterdam consensus, polycystic ovarian syndrome (PCOS) is defined by the presence of two of three of the following criteria: oligo‐anovulation, hyperandrogenism, and polycystic ovaries (≥ 12 follicles measuring 2‐9 mm in diameter, and/or an ovarian volume > 10 mL in at least one ovary)[5]
Investigations: –
Sonography — TVS is particularly used in obese patients.
The ovaries increased in volume (> 10 cm3) and also increased in number (> 12) of peripherally arranged cysts (2–9 mm) observed.
Serum values: − LH level is increased and their ratio is LH: FSH > 2:1.
– The level of estrone and estradiol is significantly increased.
– SHBG level is decreased.
− Hyperandrogenism – is mainly from the ovaries, but less from the adrenal glands.
—elevated the level of Androstenedione.
− Elevated serum testosterone (> 150 ng/dL) and DHEA–S may be mildly increased.
− Insulin resistance (IR): Elevated fasting insulin levels is > 25 µIU/ml and a fasting glucose/insulin ratio < 4.5 suggest IR (50%).
Serum insulin response levels >300 µIU/mL 2 h after a glucose (75 g) load are indicative of the severity of Insulin resistance.
Laparoscopy — B/L multiple cysts in ovaries are characteristic of PCOS.
Pathology:
Typically, the ovary’s size is enlarged. The stroma is elevated. The capsule is reinforced and has a pearly white color.
The presence of multiple (> 12) follicular cysts about 2–9 mm in diameter is clustered around the cortex.[6]
Environmental factors have been shown to play a role in the pathogenesis of PCOS.
Several studies have been done to look at the role of socioeconomic status (SES) and unhealthy behaviors, including smoking, poor diet, and lack of exercise.[7]
There is a cure for PCOS in homoeopathy. Its treatment consists of choosing a constitutional homoeopathic medicine capable of acting on the ovaries and the patient’s entire entity. There are many homoeopathic remedies capable of affecting this condition if chosen after clearly understanding the constitution, disposition, and miasmatic background if any.[8]
Lack of realization and lifestyle changes are believed to be the main factor leading to this disease. Nowadays PCOS become the most common problem affecting young girls and women of reproductive age.
In India, PCOS affects nearly 40% of females. But only 60% of women apply for treatment in hospitals when they find out that they have infertility.[9]
PCOS have found a lot of points that are either genetic or environmental but most of them are genetic.[10]
To be sure whether it is genetic or environmental, all this will be known from the twin and familial clustering study. [11,12]
CASE HISTORY: –
A case of 21 years female suffering from PCOS reported here was treated successfully within 6 months by a constitutional homoeopathic medicine SEPIA OFFICINALIS 200, SEPIA OFFICINALIS 1M with repetition as per requirement.
The improvement was relevant to the regularity of the menstrual cycle and also from ultrasonography (USG) reports.
History of present complaints : – The patient was suffering from PCOS diagnosed on 08/09/2021 by ultrasonography. There was a history of infertility. The patient did not conceive till now. There was primary infertility.
The patient was suffering from backache in the scapula region for 2 years. Backache was aggravated by sitting and in winter. There was a burning sensation in the back region. Backache was ameliorated by lying on the back and walking. There was a history of infertility. The patient married 5 years ago. The patient was suffering from irregular menses and thin and offensive leucorrhoea after menses.
Physical generals :-
Shehad good appetite but less thirst. She loved to eat spicy food. Her stool was changeable, sometimes normal and sometimes hard. She had aversion from oily fatty food which causing nausea. Her sleep was disturbed, there was anxiety which causes sleeplessness. Thermally, she was chilly. There was burning during micturition.
The patient was suffering from hirsutism
Menstrual history: – Irregular menses comes after an 8-10 days gap, scanty menses, dark red.
Leucorrhoea: – After menses, offensive and thin.
Mental generals : – Suppressed anger, aversion to work, consolation aggravation, and the stress of not having a child.
DIAGNOSIS :-
Diagnosis was based on clinical symptoms, physical examination of the patient and according to Rotterdam criteria[5] of PCOS. Irregular menses with primary infertility.
ICD-10 = E28.2[13]
CASE ANALYSIS AND EVALUATION OF SYMPTOMS: –
| S.No | TYPE OF SYMPTOMS | SYMPTOMS | INTENSITY | MIASMATIC ANALYSIS[14] |
| 1 | Mental General | Anger suppressed. | 3 | Psoric |
| 2 | Mental General | Consolation aggravation. | 2 | Psoric |
| 3 | Mental General | Aversion to do work, not interested in doing housework. | 3 | Psoric |
| 4 | Physical General | Leucorrhoea after menses, leucorrhoea is thin and offensive. | 2 | Syphilitic |
| 5 | Particular | Back pain in the scapula region with burning. | 3 | Psoric |
| 6 | Particular | Back pain aggravated by sitting position. | 2 | Psoric |
| 7 | Particular | Multiple cysts in bilateral ovaries. | 3 | Sycotic |
| 8 | Particular Generals | Infertility in a patient not conceiving pregnancy. | 2 | Sycotic |
| 9 | Physical general | Scanty menses | 3 | Sycotic |
REPERTORIAL TOTALITY[14]:-
| TOTALITY OF SYMPTOMS: – | RUBRICS |
| Anger suppressed. | MIND-AILMENTS FROM-anger-suppressed |
| Consolation aggravation. | MIND-CONSOLATION-agg-sympathy agg |
| Aversion to do work, not interested in doing housework. | MIND-LAZINESS |
| Leucorrhoea after menses, leucorrhoea is thin and offensive. | FEMALE GENITALIA/SEX-LEUKORRHEA-menses-after-agg |
| Back pain in the scapula region with burning. | BACK-PAIN-DORSAL REGION-SCAPULAE-burning |
| Back pain aggravated by sitting position. | BACK-PAIN-sitting-agg |
| Multiple cysts in bilateral ovaries. | FEMALE GENITALIA/SEX-TUMORS- ovaries-cysts |
| Infertility in a patient not conceiving pregnancy. | -STERILITY |
| Scanty menses | FEMALE GENITALIA/SEX-MENSES-scanty |
REPERTORISATION: –
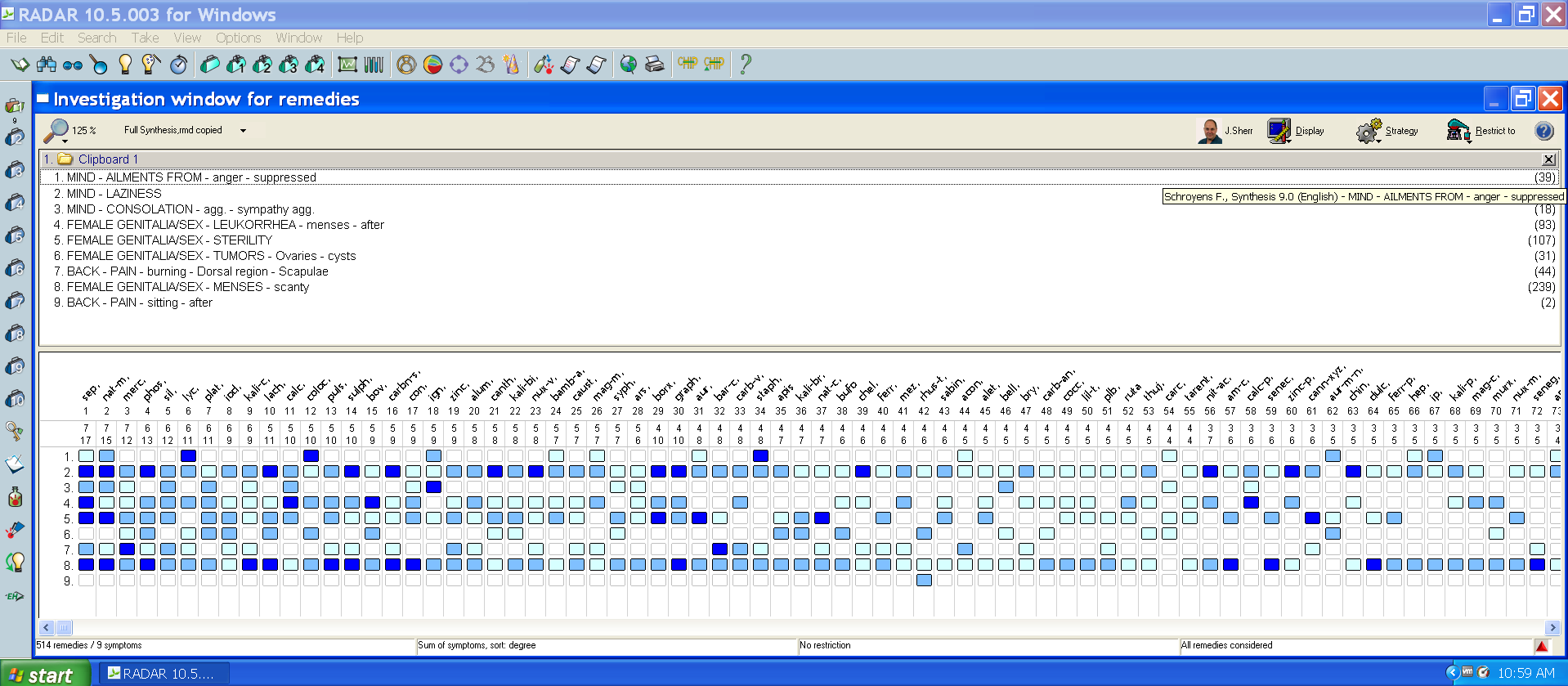
This repertorisation was done by Synthesis repertory using RADAR 10.0 software.[15]
REPERTORIAL ANALYSIS: –
- Sepia officinalis—17/7
- Natrum muriaticum—-15/7
- Mercurius corrosivus—12/7
- Phosphorus –13/6
- Silicea terra—-12/6
SELECTION OF THE REMEDY AND POTENCY: – The reportorial result showed that sepia covered maximum symptoms with the highest gradation. Therefore, an individualised single constitutional remedy,SEPIA was selected based on the totality symptoms covered in Materia medica books such as Allen’s keynotes[16] and Boericke Materia medica[17]. All symptoms are covered by sepia, although the patient was chilly so here, I have prescribed sepia 1M to the patient. High potency was selected based on the mental picture of the patient. as per guidelines from the 245 aphorism in Organon of Medicine 6th edition, higher potency was selected based on strong mental characteristics in the case.[18] The medicinal dose was only repeated when its action was ceased.[19]
Follow-up: –
After 4 months of regular treatment, the patient improved very much. She reported with USG. In USG, PCOD is cured.
| DATE | RESPONSE | PRESCRIPTION |
| 03/02/2022 | Backache relieved | Rubrum met 200 /3dose Sac lac 30/tds |
| 17/02/2022 | Her menses started coming on regular time. | Rubrum met 200 /3dose Sac lac 30/tds |
| 03/03/2022 | Backache relieved. leukorrhea is decreased | Sepia officinalis 1M /3dose Sac lac 30/TDS |
| 17/03/2022 | Improved. menses come on a regular date. | Rubrum met 200 /3dose Sac lac 30/TDS |
| 31/03/2022 | Improved. USG Report showed normal slightly enlarged ovaries. The size of the ovaries decreased. | Rubrum met 200 /3dose Sac lac 30/TDS |
| 07/03/2022 | Improved | Rubrum met 200 /3dose Sac lac 30/TDS |
DISCUSSION AND CONCLUSION: –
PCOS accounts for up to 70% of infertility in couples seeking treatment[20,21]. Poor lifestyle, diet, or any infectious negotiators increase the risk of PCOS.[22] There is currently no cure for PCOS.
Don’t eat high-energy food.[23]Mental tension, improper diet, and sedentary life are the most occurring factor worldwide.[24]
Studies in homoeopathy have shown a positive role, but these studies primarily evaluated menstrual irregularities and PCOD using ultrasonography.
Hyperandrogenism and the effect of lifestyle modification were not evaluated and statistical rigor was also lacking.[25] Due consideration has been given to all these aspects while drafting this protocol.[26] Despite the increasing incidence of this syndrome, limited research has been conducted that covers the full spectrum of PCOS.[27]
The patient was taking allopathic treatment and there was no relief so the patient came to the OPD SNHMC on the date 20/01/2022. She had earlier taken a course of ocps for treating this condition, to which she did not respond favourably.
All symptoms are covered by sepia, although the patient was chilly, so here, Sepia officinalis 1M was prescirbed to the patient. After prescribing medicine patient is improved so much. Her menstruation has become regular and leucorrhoea is also improved.
Ultrasonography (USG) showed a normal result.
This patient was successfully cured and followed up regularly.
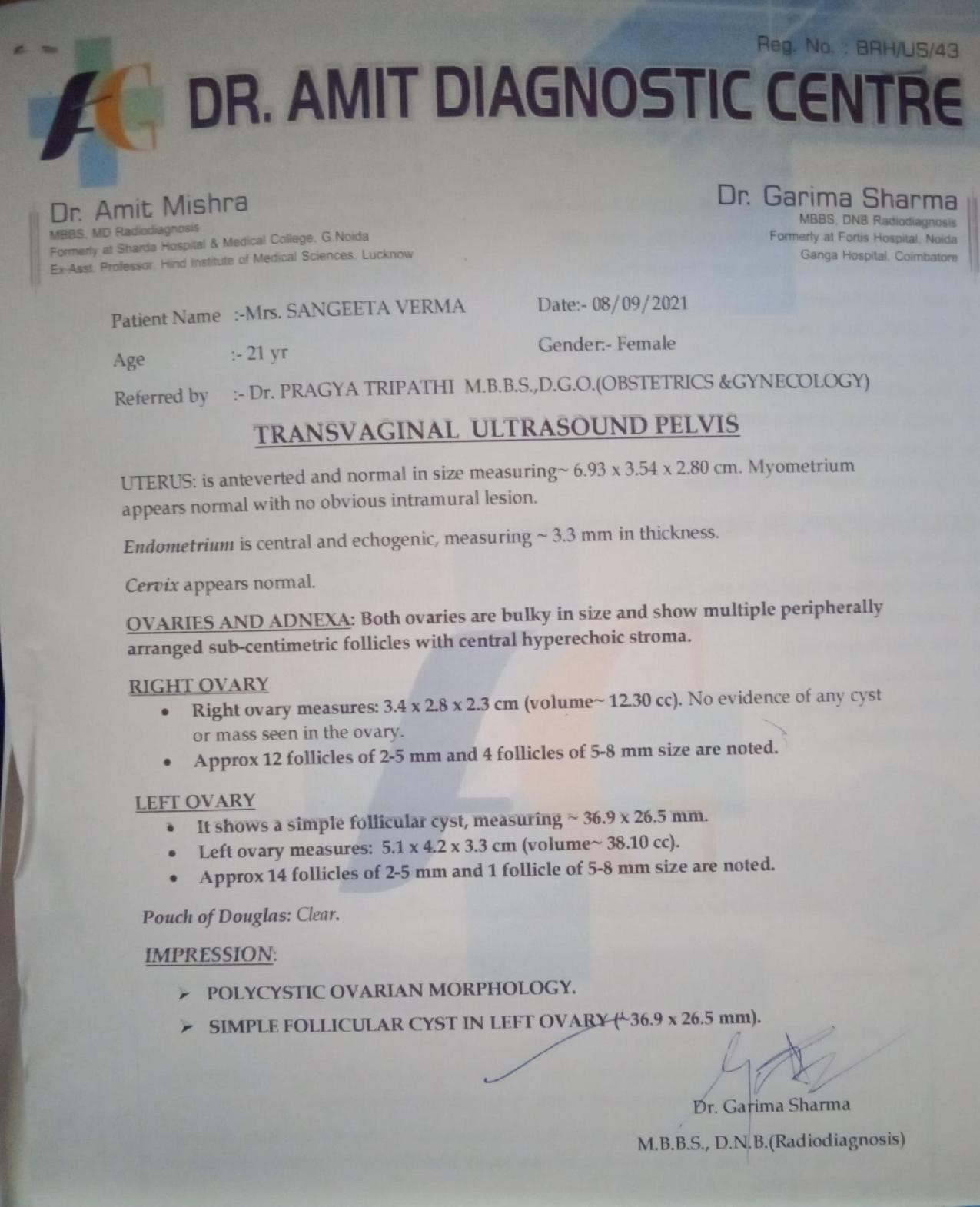
BEFORE TREATMENT
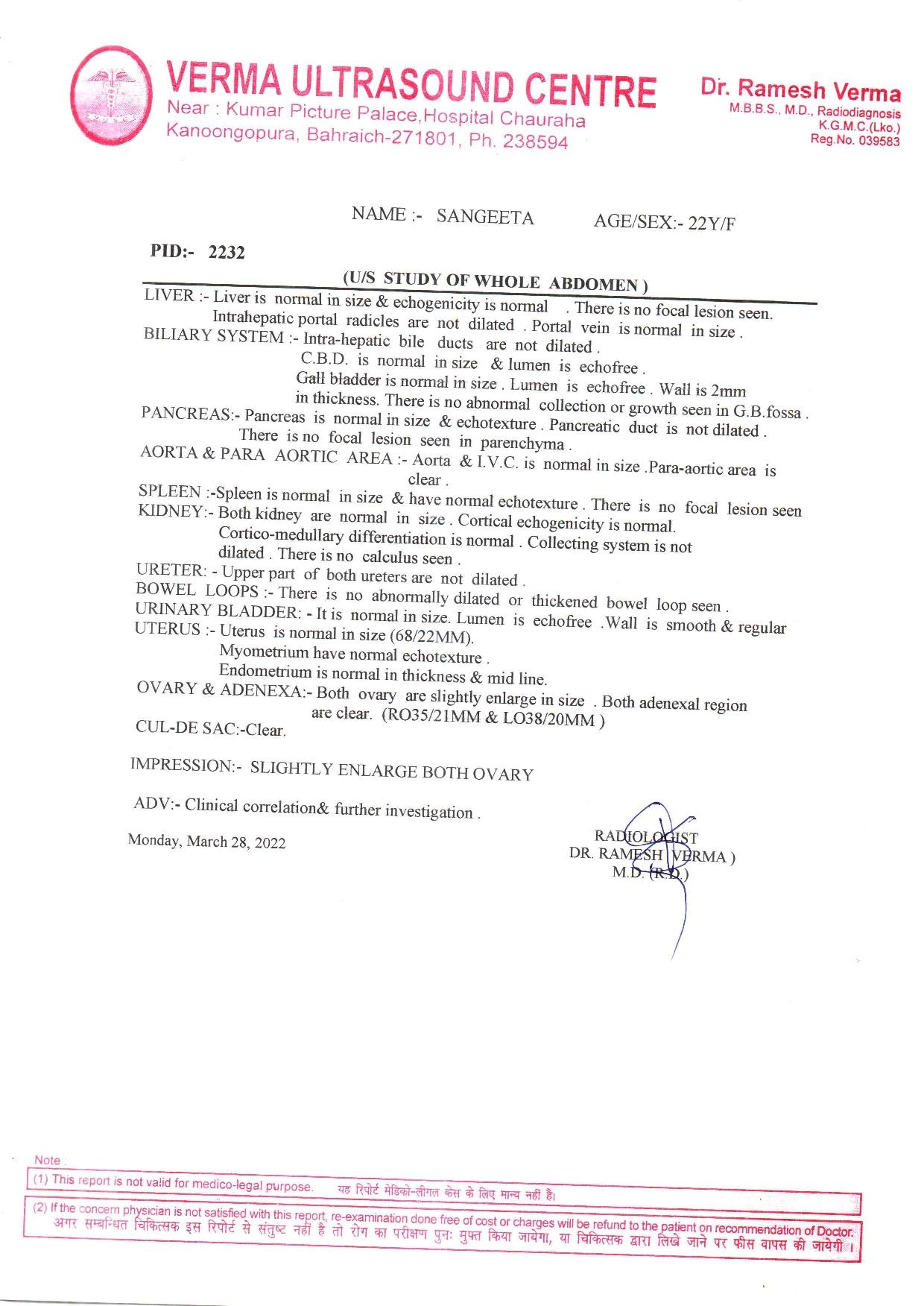
AFTER TREATMENT
REFERENCES: –
- Legro R.S. 2009. Stein-Leventhal syndrome. Encyclopedia Britannica.
- Torie Comeaux Plowden M.D. 2016. M.P.H. Reproductive endocrinology and infertility. Eunice Kennedy Shriver National Institute of Child Health and Human Development.
- Ranjith Reddy K. 2015. POLYCYSTIC Ovary Syndrome: ROLE OF AROMATASE GENE VARIANTS IN SOUTH INDIAN WOMEN. Int J Pharma Bio Sci. ;6(2)
- Joshi, Abhishek. 2022. PCOD (Polycystic Ovarian Disease): A Review Article. ECS Transactions. 107. 15973-15979. 10.1149/10701.15973ecst.
- Australas J Ultrasound Med. 2018 May; 21(2): 59–60.
- Dutta DC. Konar H. DC Dutta’s textbook of gynecology including contraception. 6th ed. Jaypee Brothers Medical Publishers (P) Ltd. Pg 459-461.
- Barthelmess, Erin K, and Rajesh K Naz. 1 Jan. 2014. “Polycystic ovary syndrome: current status and future perspective.” Frontiers in bioscience (Elite edition) vol. 6;1 104-19. doi:10.2741/e695.
- Central Council for Research in Homoeopathy. 2014. Homoeopathy in polycystic ovarian syndrome: A randomized placebo-controlled pilot study. Indian J Res Homoeopathy; 8:3-8.
- Gupta G, Gupta N, Singh S, Roja V, Dewan D. 2021. Homoeopathic treatment of women with polycystic ovarian syndrome: A prospective observational study. Indian J Res Homoeopathy 15:12-23.
- Haridas A. April 2009. Infertility and Polycystic Ovarian Syndrome. De Paul Times. [E-Journal]
- B. Roldán, J. L. San Millán, and H. F. Escobar-Morreale, , 2004.
- “Genetic basis of metabolic abnormalities in polycystic ovary syndrome,” American Journal of PharmacoGenomics, vol. 4; no. 2: pp. 93–107.
- ICD-10-CM Codes: L00-L99. 2022 ICD-10 CM Diagnosis Code L97. Available at http:// www.icd10data.com
- Babu NG, Comprehensive study of Organon, 1.1 ed. New Delhi: B. Jain publishers Ltd.:2009
- Radar Synthesis Computer Repertory, Version 10, London: Archipel Homoeopathic Software.
- Allen TIC, Allen’s Keynote Rearranged. & classified, 10 ed. New Delhi: B. Jain Publishers (P) Ltd.; 2013.
- Boericke W. Boericke’s New Manual Of Homoeopathic Material Medica & Repertory, LPE ed. New Delhi: B. Jain Publishers (P) Ltd.; 2014.
- Hahnemann S, Organon of Medicine sixth edition, Delhi, B Jain Publisher Pvt Ltd, 1996.
- Das AK. A treatise on Organon of medicine: Part 1. 2nd ed. Kolkata, India: Books & Allied; 2013.
- J. M. McAllister, R. S. Legro, B. P. Modi, and J. F. Strauss, 2015.
- “Functional genomics of PCOS: from GWAS to molecular mechanisms,” Trends in Endocrinology & Metabolism, vol. 26; no. 3: pp. 118–124.
- Diamanti-Kandarakis E.D.A . 2012. Insulin resistance and the polycystic ovary syndrome revisited: an update on mechanisms and implications. Endocrinology. 33:981–1030.
- Organization. 2011. Anonymous. ABOUT PCOS FOUNDATION. n-pc, editor.
- Goodarzi Mea. . 2011. Polycystic ovary syndrome: etiology, pathogenesis, and diagnosis. Nat Rev Endocrinol;7(4):219–231.
- Poehlman E.T.2000. Effects of resistance training and endurance training on insulin sensitivity in nonobese young woman a control randomized trial. J Clin Endocrinol Metab.;85:2463–2468.
- Urbanek M. 2014. The genetics of the polycystic ovary syndrome. Endocrinol Metab. ;3(2)
- J. D. McGarry. 1994. “Disordered metabolism in diabetes: have we underemphasized the fat component?” Journal of Cellular Biochemistry, vol. 5; no. S1994A: pp. 29–38.
ABOUT THE AUTHORS: –
- Dr Vandana Gupta, Junior Resident Doctor, Dept. of Case Taking & Repertory
State National Homoeopathic Medical College and Hospital, Lucknow.
- Dr Rahul Kumar Nirala, Junior Resident Doctor, Dept. of Case Taking & Repertory
State National Homoeopathic Medical College and Hospital, Lucknow.
- Dr Manoj Kumar Bharati Junior Resident Doctor, Dept. of Case Taking & Repertory State National Homoeopathic Medical College and Hospital, Lucknow.


