
ABSTRACT:
Introduction: Generalized Anxiety Disorder, commonly known as GAD, involves a pervasive feeling of anxiety and worry about different events or activities that occurs most days for a (minimum of six months). The worry can be difficult to control and is usually accompanied by physical symptoms such as muscle tension, irritability, difficulty in sleeping, and a feeling of restlessness. Such symptoms cause significant distress or impairment in everyday functioning in personal, social, or occupational domains. The anxiety is not produced by another medical condition or the consumption of drugs or substances. [1][2]In old age, GAD is less prevalent than young age, this anxiety is often overlooked in such patients as these people consider it as a part of their routine, especially in old age, thus anxiety is rarely addressed until severe. Allopathic medicines, when given in patients having GAD, may lead to dependence/ withdrawal symptoms. This article aims to shed light as to how homoeopathy may act as a safer option without any complexities or any adverse effects, addressing both physical and psychological aspect of the patient.
Case Summary: This article shows a case of generalised anxiety disorder in a 61 year old female, complaining of anxiety symptoms along with physical symptoms, responded commendably with three doses of LYCOPODIUM 200. Hamilton Anxiety Rating Scale (HAM-A) was used to assess the severity of anxiety.
Keywords: Anxiety, Generalised Anxiety Disorder, Cortisol, Homoeopathy, Miasm, Fear, Worry, DSM-V-TR, Lycopodium
INTRODUCTION
The Oxford Handbook of Psychiatry defines Generalized Anxiety Disorder (GAD) as “excessive worry” (generalized, free-floating, persistent anxiety) and feelings of
apprehension about ordinary events or problems. Symptoms of GAD include mental strain and muscle tightness, which lead to significant stress and functional difficulties[3].
The Diagnostic Criteria according to Diagnostic and Statistical Manual (DSM-V-TR) for GAD is as follows:
A. Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities (such as work or school performance).
B. The individual finds it difficult to control the worry.
C. The anxiety and worry are associated with three (or more) of the following six symptoms (with at least some symptoms having been present for more days than not for the past 6 months): Note: Only one item is required in children.
1. Restlessness or feeling keyed up or on edge
2. Being easily fatigued
3. Difficulty concentrating or mind going blank
4. Irritability
5. Muscle tension
6. Sleep disturbance (difficulty falling or staying asleep, or restless, unsatisfying sleep)
D. The anxiety, worry, or physical symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. E. The disturbance is not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication) or another medical condition (e.g., hyperthyroidism). F. The disturbance is not better explained by another mental disorder (e.g., anxiety or worry about having panic attacks in panic disorder, negative evaluation in social anxiety disorder, contamination or other obsessions in obsessive compulsive disorder, separation from attachment figures in separation anxiety disorder, reminders of traumatic events in posttraumatic stress disorder, gaining weight in anorexia nervosa, physical complaints in somatic symptom disorder, perceived appearance flaws in body dysmorphic disorder, having a serious illness in illness anxiety disorder, or the content of delusional beliefs in schizophrenia or delusional disorder).[4]
EPIDEMIOLOGY
A prevalence of 1.2% to 7.3% is reported for Generalised Anxiety Disorder (GAD), which is one of the most prevalent anxiety disorder in old age, yet it remains underdiagnosed and undertreated. Older adults with GAD worry more about a range of issues than their younger counterparts, such as memory loss, health, finances, grief in case of loss, how to take care of themselves, dependence on others and fear of falling. This kind of anxiety is highly situational, and frequently accompanies concomitant medical illness.[5][6]
ETIOLOGY
1. Biological Causes:
In old age, Generalized Anxiety Disorder (GAD) can stem from changes in brain structure and function. An overactive amygdala heightens fear responses, while a smaller hippocampus and weak prefrontal cortex control reduce the ability to manage stress. These changes make it harder to distinguish real threats from imagined ones.[1][7][8]
2. Neurochemical Factors:
Imbalances in brain chemicals like serotonin, dopamine, and GABA contribute to anxiety. Overactivity of the HPA axis leads to high cortisol levels, causing ongoing stress. Low GABA and high glutamate levels disturb emotional regulation, while excess norepinephrine heightens arousal and panic. [1][7][8]
3. Environmental Stressors:
Older adults often face chronic illnesses, the loss of loved ones, financial strain, and caregiving burdens. These life challenges increase feelings of vulnerability and worry, making them more prone to developing or worsening anxiety symptoms. [1][7][8] 4. Psychological Aspect:
Psychological factors play a crucial role in the development and maintenance of Generalized Anxiety Disorder (GAD). Individuals with GAD often exhibit maladaptive thought patterns such as catastrophizing, intolerance of uncertainty, and excessive worry. Personality traits like low self-esteem, and perfectionism further increase vulnerability. Additionally, people with GAD often struggle with poor coping mechanisms and problem-solving skills, which reinforces their anxiety. Coexisting psychological conditions such as depression or obsessive-compulsive traits may further intensify symptoms and hinder recovery.[1]
HOMOEOPATHIC APPROACH IN GENERALISED ANXIETY DISORDER Dr. Samuel Hahnemann, discussed Anxiety in §225 of the Organon of Medicine (5th and 6th edition), where he said that these emotional disorders, though not always the result of physical diseases, can slowly damage the corporeal state if not addressed.[9] There are three fundamental types of miasms present in our times that may describe GAD: Psora, Syphilis and Sycosis, and they also have some signs and symptoms. Individual with a Psoric Miasm will be more mentally active, rapid, anxious, restless, shy with extreme nervousness, fear that is expressed in anxiety; Individual with Sycotic Miasm will be more perverted, fear predominantly at night, melancholy, fear that is expressed by anguish; Individual with a Syphilitic Miasm will be more suspicious, fear of being misunderstood, insecure, fear that is expressed by external manifestation.[10]
IMPORTANT HOMOEOPATHIC REMEDIES FOR GENERALISED ANXIETY DISORDER
1. Aconitum Napellus – Best for sudden, intense panic or fear, often after a shock or trauma. Symptoms include palpitations, restlessness, fear of death, and heightened imagination.
2. Argentum Nitricum – Indicated for anticipatory anxiety about future events (exams, performances). Patients may feel hurried, impulsive, and expect failure, with diarrhoea and palpitations.
3. Arsenicum Album – Suitable for those with anxiety about health, safety, and control. They are restless, especially at night, fear being alone, and show compulsive organization.
4. Calcarea Carbonica – Used for overwhelming anxiety due to responsibilities, especially in those who fear breakdown, disease, or change. Symptoms include confusion, fatigue, and low confidence.
5. Kalium Phosphoricum – Indicated for anxiety from exhaustion or overwork. These individuals feel sensitive, irritable, and mentally drained, with difficulty sleeping. 6. Lycopodium Clavatum – Effective for performance-related anxiety with fear of failure. Patients appear confident but feel insecure, often with digestive issues and aversion to new things.
7. Phosphorus – For sensitive, affectionate individuals who fear being alone and seek reassurance. Anxiety worsens in unfamiliar settings or under stress.
8. Pulsatilla – For clingy, emotionally dependent individuals with mood swings and a need for company. They improve in open air and are prone to weeping. 9. Gelsemium Sempervirens – Best for stage fright or anticipatory anxiety, presenting with trembling, weakness, and diarrhoea due to nervousness.
10. Ignatia Amara – Indicated for grief- or shock-induced anxiety, with mood swings, sighing, and a “lump in the throat.” Can lead to phobias and obsessive thoughts. 11. Natrum Muriaticum – Suited for deep-seated emotional anxiety, especially from grief or past emotional trauma. Individuals are withdrawn and sensitive but hide their emotions.
12. Silicea Terra – Helpful for low self-confidence and fear of public exposure, particularly in shy individuals who avoid conflict or attention due to fear of criticism.[11][12]
CASE REPORT:
A 61 years old female, retired as a teacher, residing in urban area came at OPD on 25 April 2025 (6576/36) with anticipatory anxiety, anxiety about her health, anxiety when being in crowd which was chronic in nature. When enquired further, she stated the following complaints:
1. Anxiety from anticipation, from going to new places
2. Anxiety about her own health
3. Anxiety when being in crowd
4. Fear of height
5. Weakness of memory for dates
6. Headache [Frontal region, <sunlight, since 1 week]
7. Abdominal flatulence <night [since 1 month]
8. Sour eructation with fullness of abdomen <eating after, leading to easy satiety [Since 1 month]
9. Burning bilateral soles on and off
10. Stiffness of fingers
11. Disturbed sleep because of abdominal flatulence
12. Involuntary urination
While taking the history, the patient mentioned that she is a known case of Type 2 Diabetes Mellitus since 10 years [HbA1C: 7% (30/12/2024)] and is on allopathic medications for DM.
In her family history, father had both hypertension and diabetes mellitus. Both her parents are expired. She does not remember any episode of anxiety in her parents. Her husband suffers from Hypertension since 10 years. There is nothing significant in her siblings and her children. The patient is married and has 2 children. Her relations with her husband are satisfactory. There are no financial issues as such in the family.
The important findings in Physical Generals are as follows:
| Mouth | Dryness in mouth |
| Tongue | Dry |
| Thermal Reaction | Hot |
| Appetite | Decreased, easy satiety, eating causes abdominal fullness |
| Taste in mouth | Sour in mouth due to eructation |
| Stool | Unsatisfactory, Hard, D2N0 |
| Urine | D5-6N1-2, Cannot control |
| Sleep | Disturbed due to abdominal complaints |
| Restlessness and weakness | Present |
Mental Generals:
Patient often thinks a lot and experiences anxiety when going to new places; since patient is unable to sleep and experience a lot of abdominal complaints, she is anxious about her health, thinking what will happen if these symptoms continue; she often feels uneasiness and discomfort when in crowd; since the patient was a teacher, she cares a lot about welfare of others and is engaged in many societal welfare programmes; She fears height; She often faces difficulty in remembering dates; She wept easily when asked about her ailments and is engrossed in religious activities, often goes to religious trips for days and sits in temple for hours.
On Observation:
• Behaviour: Anxious
• Mode of Talking: Appropriate, Answers according to questions asked; Rate, volume and tone was appropriate. There was no jumping of thoughts.
• Complexion: Fair
• Appearance: Appropriate
• Built/ Nutrition: Thin
• Colour of face, eyes & skin: Brown eyes
• Decubitus: Sitting
• Expression/ Facies: Anxious
Examination of Abdominal System revealed:
• Inspection: Abdominal shape: Distended; No scars present; Umbilicus at place • Palpation: No pain on light and deep palpation; No guarding or rigidity present • Percussion: Tympanic sounds heard
• Auscultation: Normal bowel sounds heard
Examination of Stiffness of Fingers: Movement well, can grasp things well without pain Laboratory investigations advised: HbA1C, Serum Calcium, Serum Vitamin D3
Provisional Diagnosis: GENERALISED ANXIETY DISORDER (In this case, Hamilton Anxiety Rating Scale is used to assess the severity of anxiety)
Justification of the diagnosis as per DSM-V-TR
A) Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities (such as work or health).
• Anticipatory anxiety when going to new places; Anxiety about her own health; Anxiety when in crowd which is chronic and progressive, the patient is restless and fears height.
B) The individual finds it difficult to control the worry.
• Patient is often restless, feels weak, anxious when going to new places, about her own health and when in crowd which is persistent. Fears height.
C) The anxiety and worry are associated with three (or more) of the following six symptoms (with at least some symptoms present more days than not for the past 6 months):
• Restlessness: Present
• Being easily fatigued: Present
• Difficulty concentration or mind going blank: Weakness of memory for dates
• Irritability: Absent
• Muscle Tension: Weakness, Burning bilateral soles, Stiffness fingers
• Sleep disturbance: Present
D) The anxiety, worry, or physical symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. • Weakness of memory for dates, anxiety regarding health, anxious when in crowd and anticipatory anxiety along with abdominal complaints (since no pathological cause can be elicited from examination) and involuntary urination may impair important areas of functioning.
E) The disturbance is not attributable to substance/medication/medical condition. • Though the patient is diabetic, the symptoms are not solely due to diabetes. F) Not better explained by another mental disorder (e.g., panic disorder, OCD, PTSD).
Miasmatic diagnosis: Predominantly Psora with sycotic traits.
1. Anticipatory anxiety from going to new places: Psora
2. Anxiety about her own health, thinking what will happen if these symptoms continue: Psora
3. Anxiety when in crowd: Psora
4. Cares a lot about others’ welfare: Psora
5. Fear of height: Psora
6. Weakness of memory for dates: Sycosis
7. Religious disposition: Psora
8. Taste sour in mouth due to eructation: Sycosis
9. Appetite decreased; Easy satiety, eating causes fulness of abdomen: Psora 10. Sleep disturbed due to abdominal complaints: Psora
11. Involuntary urination: Sycosis
12. Flatulence of abdomen at night: Sycosis
13. Forehead pain <sunlight: Psora
14. Burning bilateral soles: Psora
15. Stiffness fingers: Sycosis
Analysis and Evaluation of Symptoms:
| Mental Generals | Anticipatory anxiety from going to new places Anxiety about her own health, thinking what will happen if these symptoms continue Anxiety when in crowd Cares a lot about others’ welfare Fear of height Weakness of memory for dates |
| Religious disposition | |
| Physical Generals | Taste sour in mouth due to eructation Appetite decreased; Easy satiety, eating causes fulness of abdomen Sleep disturbed due to abdominal complaints Involuntary urination |
| Particulars | Flatulence of abdomen at night Forehead pain <sunlight Burning bilateral soles Stiffness fingers |
Repertorial Totality: Repertorisation of this case was done using the Synthesis Repertory by Dr Frederik Schroyens.[13]
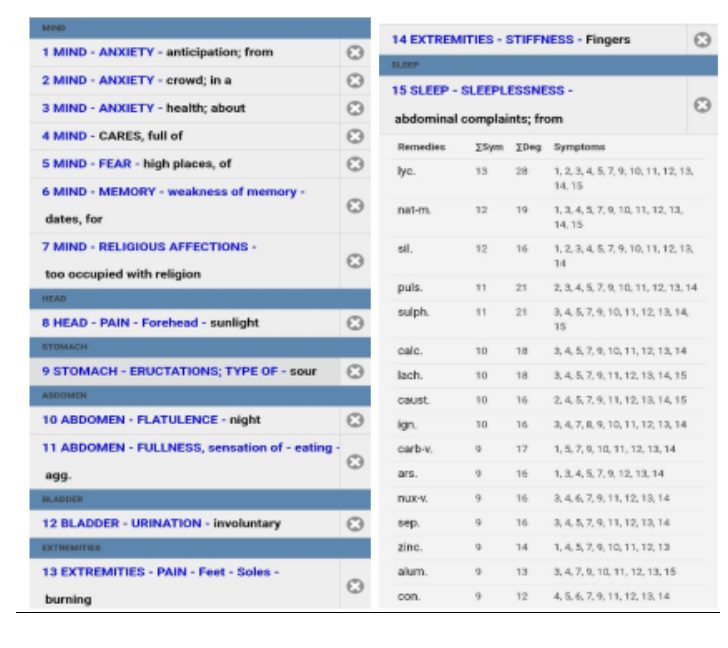
| REMEDY | Lyc | Nat-m | Sil | Puls | Sulph |
| TOTALITY/SYMPTOM SCORED | 28/13 | 19/12 | 16/12 | 21/11 | 21/11 |
Final selection of medicine with comments regarding selection of medicine: After considering repertorial analysis and consulting with Materia Medica, the final selection medicine is LYCOPODIUM CLAVATUM.
Prescription: LYCOPODIUM CLAVATUM 200/ OD/ 2 DAYS
PLACEBO 200/ TDS/ 10 DAYS
General management and auxiliary measures: Try to lead a stress free life, practice Yoga or meditation and consume nutritious food and adequate amount of water.
FOLLOW UP:
| DATE | SYMPTOM PROGRESS | PRESCRIPTION |
| 2/05/2025 | Abdominal complaints better, Burning soles better, Stiffness in fingers same, Sleep slight better Anxious mood slight better; Headache same | Lycopodium 200/OD/1 day Placebo 200/TDS/ 15 days |
| 30/05/2025 | Anxious mood same as previous visit, Weakness slight reduced, Sleep same as previous visit, Abdominal complaints better, Control on urge to urinate better; Headache better | Placebo 200/ BD/ 15 days |
| 14/06/2024 | Anxious mood improved from previous visit, Feels energetic than before, Can eat well, Abdominal complaints reduced, Stiffness fingers same, Can control the urge to urinate, Dryness of mouth better; Headache better; Burning soles better | Placebo 200/ BD/ 15 days |
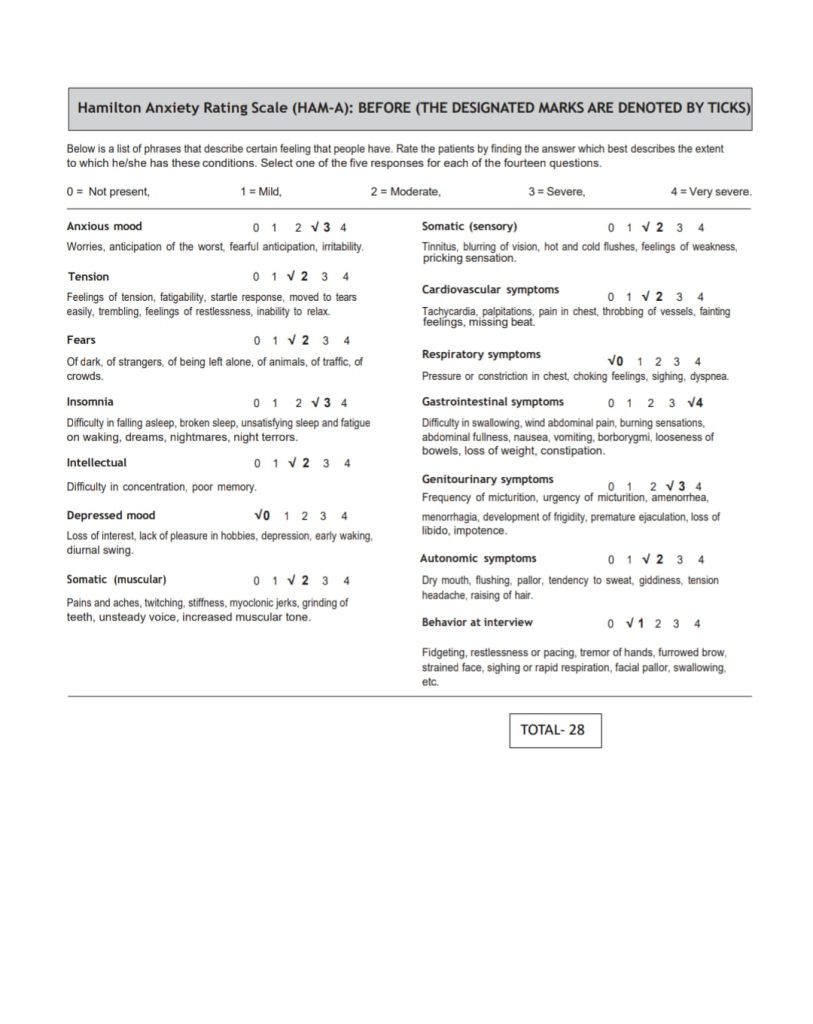
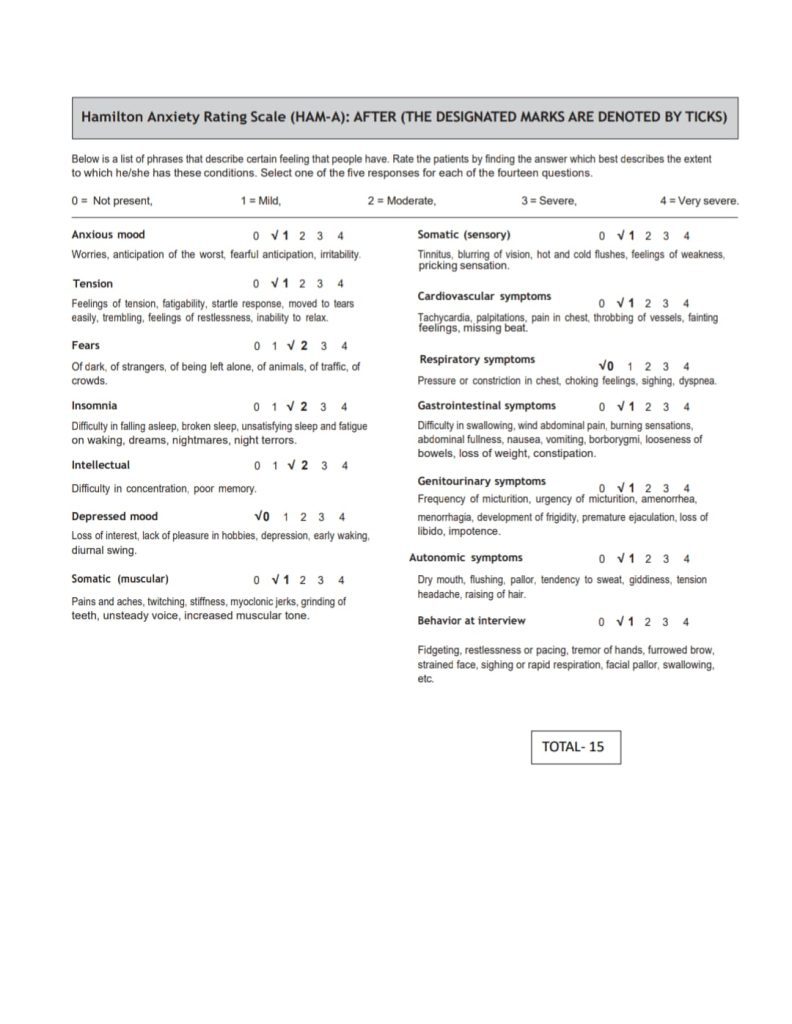
HAM-A SCORE BEFORE AND AFTER TREATMENT
| DATE | HAM-A SCORE |
| 25/04/2025 | 28 (MODERATE TO SEVERE) |
| 2/05/2025 | 24 |
| 30/05/2025 | 20 |
| 14/06/2025 | 15 (MILD) |
Conclusion:
Homoeopathy treats the person as a whole, thus following holistic approach. In this case, LYCOPODIUM CLAVATUM 200 was selected based on the similimum. This case also signifies the role of LYCOPODIUM CLAVATUM in the cases of generalised anxiety disorder. The patient religiously followed all the instructions given to her. Her complaints got better than before. This also shows that Generalised Anxiety Disorder can be managed with carefully selected homoeopathic medicine without any side-effects.
DECLARATION BY THE CORRESPONDING AUTHOR
ACKNOWLEDGEMENT: None
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
References:
1. Boland R, Verduin M, Ruiz P, Shah A, Sadock B. Kaplan & Sadock’s synopsis of psychiatry. 11th ed. Wolters Kluwer India Pvt. Ltd.
2. World Health Organization. International Classification of Diseases, 11th Revision (ICD-11). Geneva: World Health Organization; 2019. Available from: https://icd.who.int/
3. Semple D, Smyth R. Oxford handbook of psychiatry. 4th ed. Oxford ; New York, Ny: Oxford University Press; 2019
4. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5-TR. 5th ed., text rev. Arlington (VA): American Psychiatric Association; 2022
5. Wolitzky‐Taylor KB, Castriotta N, Lenze EJ, Stanley MA, Craske MG. Anxiety disorders in older adults: a comprehensive review. Depression and anxiety. 2010 Feb;27(2):190-211.
6. Bassil N, Ghandour A, Grossberg GT. How anxiety presents differently in older adults. Current Psychiatry. 2011 Mar;10(3):65-71.
7. Manipal Hospitals. The science behind anxiety: What happens in your brain & how to manage it. Manipal Hospitals; 2024 Mar 20. Available from: https://www.manipalhospitals.com/delhi/blog/anxiety-effects-on-brain/
8. NeuroLaunch Editorial Team. Biological causes of anxiety disorders: Understanding the role of biological factors. NeuroLaunch. 2024 Jul 11. Available from: https://neurolaunch.com/biological-causes-of-anxiety-disorders/
9. Dudgeon. R.E, ‘Organon of Medicine by Samuel Hahnemann, Aude Sapere’, Translated from fifth edition, with an Appendix. 2005
10. Tyler G. Miasms – Understanding and classifying miasmatic symptoms. Hpathy. 2005 Apr 15. Available from: https://hpathy.com/organon philosophy/miasms-understanding-and-classifying-miasmatic-symptoms/
11. Boericke W. Pocket Manual of Homoeopathic Materia Medica & Repertory. Reprint. 9th Ed. New Delhi: B. Jain Publishers (Pvt.) Ltd.; c2002. 12. Bailey PM. Homeopathic psychology : personality profiles of the major constitutional remedies. Berkeley, Calif.: North Atlantic Books; 1995. 13. Schroyens F. Synthesis Repertory Version-9.1 Repertorium Homeopathicum Syntheticum.
About the Author:
Dr. Chhavi Gupta1, Dr. Santosh Hande2
1MD Scholar, Department of Psychiatry, Government Homoeopathic Medical College and Hospital, Bhopal, Madhya Pradesh
2Head of the Department, Department of Psychiatry, Government Homoeopathic Medical College and Hospital, Bhopal, Madhya Pradesh