
Abstract
Psoriasis is classified as an immune-mediated illness, meaning that it affects the immune system and results in inflammation throughout the body.
Indications of inflammation could include skin scales and the rising plaque, which resembles a variety of skin tones.
This occurs as a result of an overactive immune system stimulating the proliferation of skin cells, which normally grow to maturity and then shed entirely in less than a month.
Skin cells in psoriasis complete this task in three to four days.
On the skin’s surface, skin cells accumulate rather than shed. Though they can occur anywhere on the body, plaques and scales are most frequently observed on the scalp, knees, and elbows. While homoeopathic therapy can offer a true “cure” for psoriasis through a constitutional similimum, conventional modern medicine only attempts to palliate the symptoms of the disorder.
Keywords: Psoriasis , Homoeopathy, Cure, Similimum
Introduction
Between the ages of 20 and 30 and 50 and 60 are the two primary peaks for the beginning of psoriasis, which affects 2% to 3% of adults overall. Thirty percent of cases of psoriasis start in childhood, with the age range of seven to ten years being the median starting age. Psoriasis is a genetically transmitted disease, affecting at least 10% of the population who inherit one or more genes that might cause the condition. An early age of onset is predicted by a family history of psoriasis. The illness is incurable and is marked by physically and psychologically crippling remissions and persistent, repeated exacerbations.
The abnormal activation of cutaneous dendritic cells (DCs), which produces TNF and IL-23, is the mechanism underlying psoriasis. These DCs induce the migration of autoimmune Th17 and Tc17 cells into the epidermis, where they generate the Th17 cytokines IL-17 and IL-22 and identify epidermal autoantigens. Th17 cytokines cause aberrant keratinocyte hyperproliferation and activate keratinocytes to create chemokines and antimicrobial peptides (AMP), which are hallmarks of the epidermal phenotype of plaque psoriasis.
It seems that a key role in the pathophysiology of chronic plaque psoriasis is played by the TNF–IL-23–Th17 pathway. By examining early stages in the pathophysiology of psoriasis, a different inflammatory route has been identified. This pathway is mediated by plasmacytoid dendritic cells (pDCs), which produce significant quantities of type I IFNs. In acute psoriasis types like erythrodermic psoriasis, the pDC–IFN pathway is predominant.Last but not least, examination of pustular psoriasis has demonstrated that IL-17-induced neutrophil infiltration is essential for the cleavage and activity of IL-36, which in turn causes DCs to produce IL-1 and further encourage Th17 polarization. Pustular psoriasis appears to be dominated by the IL-36–IL1 pathway.
Comorbidity, or the coexistence of several illnesses with one main illness, has been linked to psoriasis. Psoriasis sufferers are more likely to develop concomitant conditions such as arthritis, heart disease, diabetes, cancer, and hypertension than the general population. The prevalence of comorbidities rises with age. Two thirds of psoriasis patients over 65 have two or more comorbidities, and nearly half have at least three comorbidities.
| Predisposing Factors2 | Clinical Presentations2 |
1. Immune system and Genetics play key roles in causing psoriasis. 2. Smoking , Alcohal. 3. Injury to skin – Koebner [KEB-ner] phenomenon, where scratches, sunburns, bug bites, and vaccinations can all trigger psoriasis flares.. 4. Illness – ear infection, bronchitis, tonsillitis, or respiratory infection. There is a connection between streptococcus infection (strep throat) and guttate psoriasis, as it often triggers the first onset of guttate psoriasis in children.. 5. Weather .- Cold weather can often cause psoriasis flares due to less sunlight and humidity, heated and drier indoor air, 6. Stress. 7. Allergy. | 1. Variations in the morphology of psoriasis • Chronic plaque psoriasis • Guttate psoriasis (acute eruptive psoriasis) • Pustular psoriasis • Erythrodermic psoriasis • Light-sensitive psoriasis • HIV-induced psoriasis • Keratoderma blennorrhagicum (Reiter syndrome) 2. Variations in the location of psoriasis • Scalp psoriasis • Psoriasis of the palms and soles • Pustular psoriasis of the palms and soles • Pustular psoriasis of the digits • Psoriasis inversus (psoriasis of flexural areas) • Psoriasis of the penis and Reiter syndrome • Nail psoriasis • Psoriatic arthritis |
Common Therapeutic Treatment
Allopathic Methods:
- To alleviate symptoms of psoriasis, antimetabolites, immunosuppressant, retinoid, phosphodiesterase, and tnf blockers may be recommended.
•Medications such as immunomodulators, agonists and antagonists of interleukin-12 and 23 and blockers of interleukin-23 are also recommended for adult patients who have associated complications.
Case Study:
A male patient Mr RY of age 19 years came to me on 25/5/2024 in OPD with a pre- diagnosed case of psoriasis with a complaint of scaly Plaque with itching on the left gluteal region since 2 years . Plaque scaly , silvery peeling of skin , redness with small bump on left gluteal region .
HOPC: Gradual progression, allopathic treatment taken with temporary palliation.
F/H: Nothing significant
Past History:
Skin ailments during childhood (unspecified by patient)
Personal History:
Occupation: student
Hobbies: likes listening to old songs
Physical Generals:
Appetite: 3meal/day
Thirst: 1 L/day.
Desire: Sweet (2+)
Stool: constipation.
Urine: normal
Sweat: Profuse , sour smelling .
Sleep: increased 10-12 hrs/day; Restless, Turning and twisting all night
Dreams: nothing specific
Thermals: Hot
Mental Generals
Answer slowly
Think he has everything
Ability for philosophy .
Prescribing Totality:
Answering slowly
Think he has everything .
Ability for phillosophy .
Restless sleep, twisting and turning all night
Scaly eruption with itching
Itching amelioration by scratching .
Sweat profuse , sour smelling .
Repertorial Analysis:
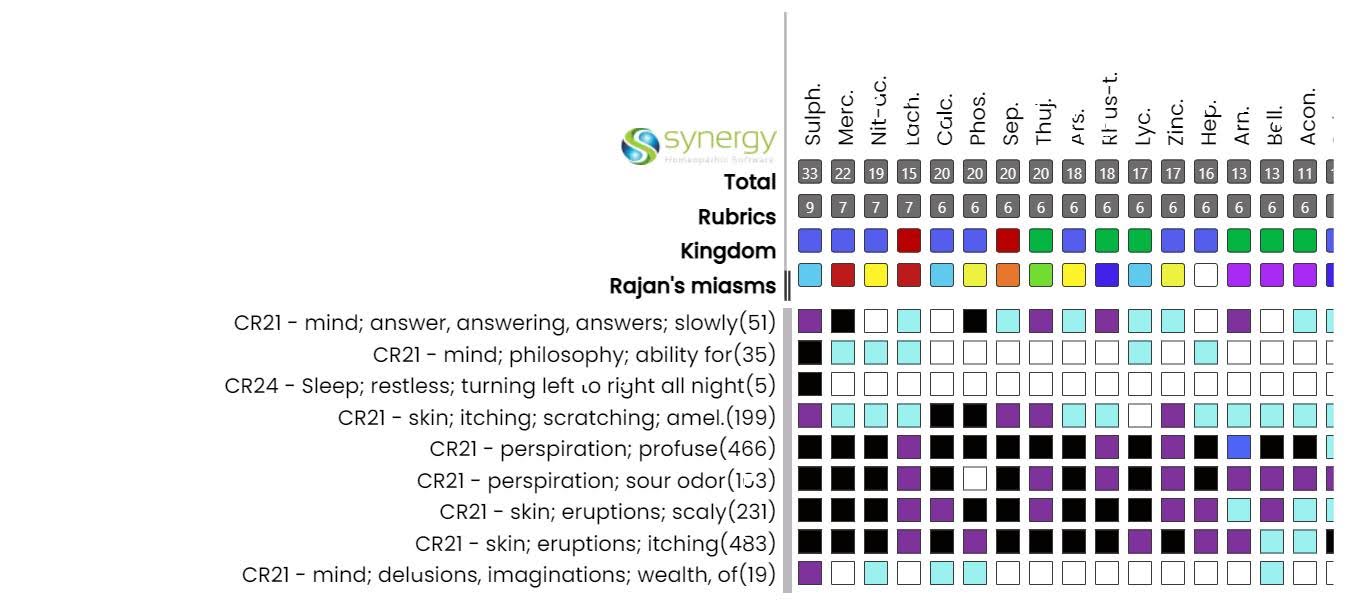
Prescription:
Sulphur 200/OD/ 3 days followed by placebo for 7 days
Follow up:
| 06/06/2024 | Relief for 5 days followed by aggravation | Sulphur 200/OD/2 days Placebo/OD/15 days |
| 30/06/2024 | Other complaints better | Placebo/BD / 30 days |
| 30 /07/2024 | Complete resolution of scaly plaque . | Placebo for 30 days |
| 24/08/2024 | No new complaints | Placebo for 30 days |
Investigations:
BEFORE – 25/05/2024 AFTER 24/08/2024

Conclusion:
| Before treatment | After treatment |
|
. |
Modern medicine is relatively unsuccessful in the cure of Chronic Psoriasis while such cases can easily be cured through Homoeopathic principles.
References
- Habif’s Clinical Dermatology: A Color Guide to Diagnosis and Therapy [7th Edition] 9780323612692, 9780323612708, 9780323612715 – DOKUMEN.PUB [Internet]. dokumen.pub. dokumen.pub; 2020 [cited 2024 Aug 29]. Available from: https://dokumen.pub/habifs-clinical-dermatology-a-color-guide-to-diagnosis-and-therapy-7th-edition-9780323612692-9780323612708-9780323612715.html.
- National Psoriasis Foundation. About Psoriasis [Internet]. www.psoriasis.org. 2021. Available from: https://www.psoriasis.org/about-psoriasis/
