Abstract
Children’s upper respiratory tract infections are a persistent global threat. The frequency of adenoid hypertrophy and its associated problems is very high and primarily affects the paediatric population. Whether enlarged by viral or non-infectious reasons, adenoids undoubtedly result in feeding issues, nasal discharge, mild to severe nasal obstruction, and associated facial traits that are easy to identify. Surgery is nearly usually required to treat severe cases of adenoid hypertrophy, however homoeopathy can control and lessen the problems brought on by the hypertrophy in less severe cases. This article examines homeopathy’s function in treating adenoid hypertrophy, emphasising its holistic tenets and customised therapeutic approaches.
Keyword –Adenoid Hypertrophy; Homoeopathy; Paediatrics;
Introduction
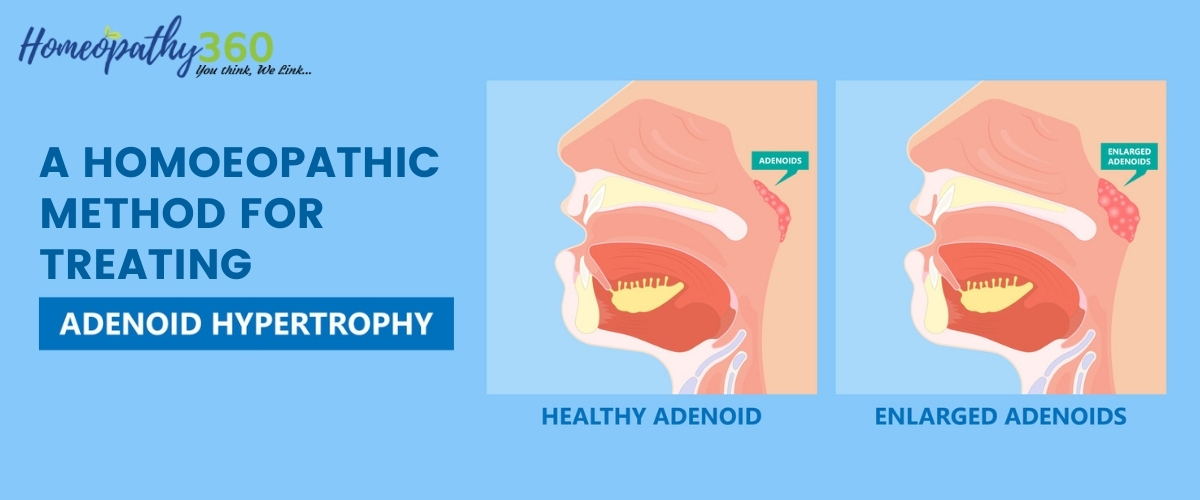
Adenoids are little tissue lumps situated above the roof of the mouth near the rear of the nose. As a component of the immune system, they shield us from bacterial and viral illnesses. Only children have adenoids, which begin to grow at birth and reach their maximum size between the ages of three and five. They start to shrink around the ages of 7 and 8, and by late adolescence, they are typically invisible, having vanished entirely by adulthood.
Anatomy and Physiology Of Adenoids
The adenoids, which are lymphoid tissues located beneath the mucous membrane at the intersection of the nasopharynx’s posterior wall and roof, are essential to the immune system, especially in the early stages of life. They have a quadrilateral form with rounded corners and develop between weeks 12 and 14 of pregnancy. The pseudostratified ciliated columnar epithelium lines the folds that enlarge the surface area of the adenoids. The adenoids include lymphoid follicles made up of B cells, T cells, and dendritic cells, and this surface epithelium is crucial for immune responses.
These lymphoid follicles, which have crypts bordered by stratified squamous and reticulated epithelium, are embedded in mucosal folds. Because they house lymphocytes, plasma cells, macrophages, and dendritic cells, the adenoids contribute to the first line of immunological defence against eaten and inhaled antigens.
Important immune cells include natural killer (NK) cells, which hunt down aberrant cells; T cells, which can be classified as either cytotoxic or helper; and B cells, which make antibodies. The nasal-associated lymphoid tissue (NALT) system includes the adenoids and other lymphoid tissues in the nasopharynx.
Etiology
It can be generally divided into causes that are contagious and those that are not.
Infectious causes:
- Viral pathogens: Adenovirus, Coronavirus, Coxsackievirus, Cytomegalovirus (CMV), Epstein-Barr virus (EBV), Herpes simplex virus (HSV), Parainfluenza virus, and Rhinovirus are among the viruses that can cause adenoid hypertrophy.
- Bacterial pathogens: Anaerobic bacteria (such as Fusobacterium, Peptostreptococcus, and Prevotella species) and aerobic bacteria (such as alpha-, beta-, and gamma-hemolytic Streptococcus species, Haemophilus influenzae, Moraxella catarrhalis, Staphylococcus aureus, Corynebacterium diphtheria, and Mycoplasma pneumoniae) can both cause adenoid hypertrophy.
Non-infectious causes
- Gastroesophageal reflux: The adenoid tissue may get irritated by acid reflux. • Allergies: Hypertrophy and inflammation can result from allergic responses. • Cigarette smoke exposure: Smoke exposure can lead to long-term adenoidal irritation and hypertrophy.
- Adenoid hypertrophy in adults may be linked to more severe illnesses including lymphoma, HIV infection, or sino-nasal cancer.
Epidemiology
Because the adenoids naturally shrink and retreat during puberty, adenoid hypertrophy is more common in children than in adults. A recent meta-analysis found that about 34.46% of children and adolescents have adenoid hypertrophy. The clinical and radiological results showed a prevalence of 83.87% and 79.03%, respectively.
Clinical Features
The signs and symptoms of hypertrophied adenoids can be divided into two groups: infection-related and hypertrophy-related.
Hypertrophy-related symptoms
In Infants:
feeding difficulties brought on by sporadic breathing interruptions.
Failure to thrive, increased exhaustion, and inadequate food intake
breathing loudly and making a frothy, wet nasal sound.
In Older Children:
- Nasal obstruction leading to mouth breathing.
- Children of all ages, from neonates to teenagers, can develop obstructive sleep apnoea, which affects 1–4% of them. Its prevalence peaks between the ages of 2 and 8.
- Voice changes to a nasal tone.
- subsequent chronic rhinitis and mechanical obstruction-induced nasal discharge.
Symptoms due to Infection
- Nasal Discharge – sinusitis and rhinitis with purulent discharge. 2. Epistaxis– infections that cause nosebleeds.
- Throat Issues: Frequent upper respiratory tract infections, such as cough, tonsillitis, pharyngitis, and post-nasal discharge.
- Ear Problems: Chronic otitis media, acute otitis media, and recurrent inflammation of the Eustachian tube. The youngster is at risk for otitis media due to mechanical obstruction caused by the adenoids in the nasopharynx being close to the middle ear and the eustachian tube. Otitis media and eustachian tube dysfunction are caused by local inflammation and mucosal oedema brought on by the regional spread of a bacterial biofilm.
- Lymphadenitis: higher deep cervical lymph node infection.
- Respiratory Issues: worsening of bronchitis and bronchial asthma. 7.
General Symptoms: Nocturnal enuresis (bedwetting) and night terrors due to suffocation.
Diagnosis
Since the adenoid tissue is located in an area that is difficult to see, the diagnosis of adenoid hypertrophy is based more on clinical characteristics than examination results. Children typically exhibit halitosis, a persistent cough, mucopurulent posterior nasal drip, and a stuffy nose. When hyperplastic adenoids intrude on the posterior nasal choanae, causing a buildup of secretions in the nose, they develop a nasal intonation of speech and sometimes snort.
- X-ray imaging – A 25%, 50%, or 75% reduction in the amount of air column available in front of the adenoids is categorised as mild, moderate, or severe adenoid hypertrophy, respectively. The basic plain lateral X-ray of the neck is still a great tool for screening and identifying the adenoids.
- CT Scan– In addition to giving a better picture of the nasopharynx and adenoids, a CT scan can identify the kind and nature of lesions that may be causing bone damage, which could indicate the presence of a malignant tumour. A CT scan is also helpful in the diagnosis of chronic sinusitis.
- Nasopharyngoscopy– The degree of adenoid hypertrophy can be more accurately estimated by examining the adenoids with a nasopharyngoscopy. The most severe condition, where the adenoid tissue is in direct contact with the palate at rest (Grade 4), is ranked from Grade 1, where the adenoids are not in contact with other structures.
- Finding the adenoid-to-nasopharyngeal (AN) ratio is the most accurate method. It is the ratio of the nasopharyngeal aperture (measured by the distance between the posterior edge of the hard palate and the spheno basiocciput) to the measurement of the adenoid tissue (measured by the distance between the basiocciput region and the most convex area of the adenoid pad).
Differential Diagnosis
- Endonasal Foreign Bodies: Because younger children are more likely to put objects in their noses, these can result in nasal blockage, discharge, and occasionally infection.
- Incomplete Choanal Atresia: a congenital disorder that causes obstruction of the choanae, the channel at the back of the nose, which can cause nasal congestion in older children and respiratory discomfort in infants.
- Infectious or Allergic Rhinitis: Because of the inflammation and irritation of the nasal mucosa, these disorders result in nasal congestion, discharge, and sneezing. •
Neoplasms: Consideration should be given to both benign and malignant tumours, especially in patients whose symptoms do not go away after therapy.
Homoeopathic Management
- Baryta Carb
Chronic tonsil hypertrophy and suppuration following a mild cold or after suppressing perspiration on the feet. Particularly appropriate for elderly individuals with dwarfism, scrofulous children, and those with acute or chronic inflammations from colds. Increased infiltration is more likely to result from the inflammation.
- Calcarea Carb
tonsil swelling and trouble swallowing. stopping of the nose when you wake up in the morning; offensive nasal odour, similar to that of eggs; gets cold once the weather changes;
- Bacillinum
persistent propensity to get chilled; suggested in children having a history of consumptive family members; The neck’s glands are sensitive and swollen; Effective as a concurrent treatment
- Thuja
tonsil and throat swelling. painful swallowing, particularly when it involves empty or salivary swallowing; mucus buildup in the back of the nares; persistent catarrh following measles; smelt in the nose like brewing beer or fish brine.
- Tuberculinum
All youngsters and young students who have inherited tuberculosis may be immune from their inheritance and their resilience will be restored if they receive two doses of tuberculinum at long intervals. It comes in 10M, 50M, and 100M potencies. The majority of adenoids and neck tuberculous gland cases are cured by it.
References
1) Gupta Piyush, Menon PSN, Ramji Siddarth and Lodha Rakesh, PG Textbook of Pediatrics, Volume 2, 1st edition, ISBN: 978-93-5152-955-2, New Delhi: Jaypee Brothers Medical Publishers (p) Ltd. 2015Ghai O.P., Essentials Pediatrics, 6th Edition, 1 A, Narainall,, New Delhi
2) Phatak SR. Materia Medica of Homoeopathic Medicines: Revised and Enlarged Edition. New Delhi, India: B Jain; 2003.
3) Boericke, W. Pocket Manual of Homoeopathic Materia Medica & Repertory (Second Revised and Reaugmented edition).
4) Kent JT, Lectures on Homoeopathic Materia Medica, B Jain Publishers 5) John Henry Clarke, A Dictionary of Practical Materia Medica, 22nd edition,
Author
Dr. Prasoon Choudhary – Professor (HOD)
Dr. Kamal Nainawat PG Scholar,
Department of Paediatrics, Dr. MPK Homoeopathic Medical College, Hospital and Research Centre, Homoeopathy University, Jaipur (Rajasthan)