Inflammatory Bowel Disease (IBD): Understanding Symptoms, Cause and Management
Definition: Inflammatory Bowel Disease (IBD) refers to a group of chronic conditions characterized by inflammation of the gastrointestinal (GI) tract. The two main types of IBD are Crohn’s disease and ulcerative colitis.
Types:- IBD is mainly of 2 TYPE
- Crohn’s Disease
- Ulcerative colitis
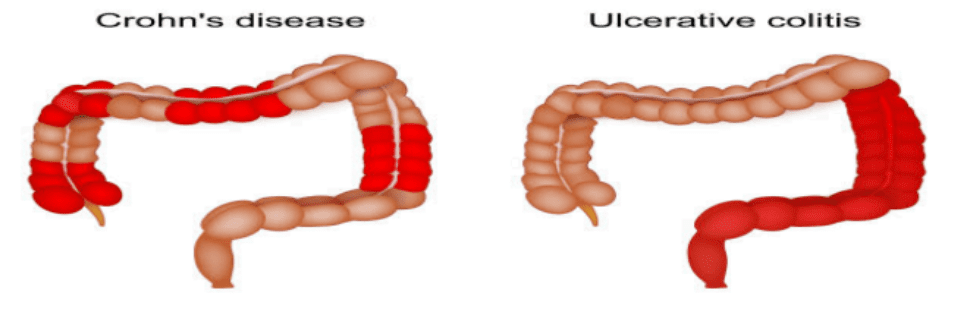
- Crohn’s Disease:- that is a chronic inflammatory condition that affects the GI tract. It is a type of inflammatory bowel disease characterized by transmural, non caseating,granulomatous inflammation.
Inflammation that can occur anywhere along the GI tract, from the mouth to the anus, but most commonly affects the ileum and the colon.
- Ulcerative colitis :-Ulcerative Colitis is a chronic inflammatory bowel disease characterized by inflammation and ulceration of the innermost lining of the colon and rectum, resulting in symptoms such as bloody diarrhea, abdominal pain, and urgency to defecate.
Etiology:-
The etiology of Inflammatory Bowel Disease is multifactorial, involving a complex interplay between genetic predisposition, immune system dysregulation, environmental triggers, and alterations in the gut microbiome. Below is a explanation of each contributing factor:
1. Genetic Factors
Familial Risk:
First-degree relatives of individuals with IBD have a significantly increased risk (up to 10 times higher).
Genetic susceptibility is more pronounced in Crohn’s Disease than Ulcerative Colitis. Specific Genes:
Over 200 genetic loci have been identified in association with IBD through genome-wide association studies (GWAS).
2. Immune System Dysregulation
Innate Immune System: Defective recognition of gut microbes by pattern recognition receptors leads to an exaggerated inflammatory response. Impaired autophagy disrupts bacterial clearance, contributing to chronic inflammation.
Adaptive Immune System: T-helper cells (Th1, Th2, and Th17) are overactivated, leading to increased pro-inflammatory cytokine production.
Crohn’s Disease: Predominantly Th1 and Th17-mediated inflammation.
Ulcerative Colitis: Associated with Th2-like cytokines (e.g., IL-5, IL-13).
3. Environmental Factors
Smoking: Increases the risk of Crohn’s Disease but is protective in Ulcerative Colitis.
Diet: Diets high in refined sugars, fats, and processed foods may alter the gut microbiome, promoting inflammation. Low dietary fiber may impair intestinal barrier function.
Infections: Prior infections, such as those caused by enteric pathogens, may disrupt gut homeostasis, triggering IBD in genetically predisposed individuals.
Antibiotics: Repeated or early-life use of antibiotics is linked to an increased risk, possibly due to disruption of the gut microbiome.
Stress: Although not a direct cause, stress can exacerbate symptoms and alter immune regulation.
Geographic and Lifestyle Factors :Higher incidence of IBD in developed countries suggests a role for urbanization, hygiene, and Westernized diets .
4. Intestinal Barrier Dysfunction : The intestinal epithelial barrier is a critical defense mechanism in IBD.
5.Other Contributing Factors:
Vitamin D Deficiency: Low vitamin D levels may impair immune regulation and increase the risk of IBD.
Hormonal Factors: Hormonal changes (e.g., during pregnancy) can influence disease activity. :-
Clinical Features :
The symptoms of InflammatoryBowel Disease (IBD), which includes Crohn’s Disease (CD) and Ulcerative Colitis (UC), can vary depending on the type and severity of the disease. Common symptoms include:
1. Abdominal Pain and Cramping , Often occurs due to inflammation in the intestines, and can vary from mild to severe.
In Crohn’s Disease, the pain is usually in the lower right side of the abdomen, while in Ulcerative Colitis, it’s more common in the lower left side.
2. Diarrhea : Chronic, often watery diarrhea.
In Ulcerative Colitis, diarrhea may be accompanied by blood, mucus, or pus due to the involvement of the colon and rectum.
In Crohn’s Disease, diarrhea may also occur with the presence of undigested food, as it can affect the small intestine.
3. Rectal Bleeding: Blood in the stool or on the toilet paper, particularly in Ulcerative Colitis. In Crohn’s Disease, bleeding may also occur but is typically less frequent than in UC.
4. Weight Loss:Unexplained weight loss due to malabsorption, poor appetite, or nutrient deficiencies.
More common in Crohn’s Disease, especially if it affects the small intestine.
5. Fatigue: Chronic tiredness and lack of energy due to the body’s ongoing inflammation or anemia (due to blood loss).
6. Fever: Low-grade fever is common during flare-ups, indicating the body’s immune response to inflammation.
7. Urgency to Defecate: Astrong, often uncontrollable urge to have a bowel movement, especially in Ulcerative Colitis due to rectal inflammation.
8. Tenesmus: A feeling of incomplete evacuation after a bowel movement, which is common in Ulcerative Colitis.
9. Nausea and Vomiting: Occurs due to inflammation or blockage, particularly if Crohn’s Disease affects the small intestine.
10. Anemia: Fatigue, dizziness, and weakness caused by a reduction in red blood cells due to chronic blood loss or poor absorption of iron and other nutrients.
11. Joint Pain and Inflammation: Joint pain or swelling (arthritis) can occur in both Crohn’s Disease and Ulcerative Colitis as extra-intestinal manifestations of IBD.
12. Mouth Sores: Sores or ulcers in the mouth can appear, especially in Crohn’s Disease
13. Skin Problems: Rashes or sores (such as erythema nodosum or pyoderma gangrenosum) can develop due to systemic inflammation.
Investigations:-
The investigation of Inflammatory Bowel Disease (IBD) involves a comprehensive approach that includes clinical evaluation, laboratory tests, endoscopy, imaging studies, and sometimes biopsy to diagnose and assess the severity of the disease. The aim is to differentiate between Crohn’s Disease (CD) and Ulcerative Colitis (UC), establish the extent of disease involvement, and identify complications.
1. Clinical Evaluation
History: Collecting detailed information about symptoms (e.g., diarrhea, abdominal pain, rectal bleeding), family history of IBD or autoimmune diseases, and any extra-intestinal symptoms (e.g., joint pain, skin rashes).
Physical Examination:
Assess for signs of anemia (e.g., pallor), malnutrition, abdominal tenderness, or perianal disease (fistulas or abscesses).
Rectal examination to check for blood or mucous in the stool.
2. Laboratory Tests
Complete Blood Count (CBC): To assess for anemia (due to chronic blood loss or malabsorption) and signs of inflammation (e.g., leukocytosis, thrombocytosis).
(CRP): A marker of systemic inflammation. Elevated levels are common during disease flares. Erythrocyte Sedimentation Rate (ESR): Another inflammation marker, often elevated in active IBD.
Iron Studies: To assess for iron deficiency anemia, a common complication of chronic blood loss or malabsorption.
Vitamin and Mineral Deficiency Tests: Testing for deficiencies in B12, folate, Vitamin D, calcium, etc., is important due to malabsorption in IBD.
Liver Function Tests: Elevated liver enzymes may indicate complications like primary sclerosing cholangitis (especially in UC).
Stool Tests:
Stool cultures to rule out infections.
Fecal Calprotectin: Astool marker that helps assess the degree of intestinal inflammation. Serological Tests:
Anti-Saccharomyces cerevisiae Antibodies (ASCA): Often elevated in Crohn’s Disease.
Perinuclear Anti-Neutrophil Cytoplasmic Antibodies (p-ANCA): Commonly elevated in Ulcerative Colitis.
3. Endoscopy
Endoscopic procedures allow direct visualization of the GI tract and provide essential tissue samples (biopsies) for diagnosis.
Colonoscopy: The gold standard for diagnosing IBD. It allows visualization of the colon and rectum to detect characteristic features of Ulcerative Colitis (e.g., continuous inflammation starting from the rectum) and Crohn’s Disease (e.g., segmental inflammation with skip lesions).
Biopsy samples are taken to confirm diagnosis and differentiate between CD and UC.
Upper GI Endoscopy (Gastroduodenoscopy): Recommended if Crohn’s Disease affects the upper GI tract (e.g., stomach, duodenum).
Flexible Sigmoidoscopy: This is useful for examining the distal colon and rectum, particularly for diagnosing Ulcerative Colitis.
4. Imaging Studies
Imaging is used to evaluate disease extent, complications (e.g., strictures, fistulas), and disease activity.
Abdominal X-rays: To identify complications such as toxic megacolon or bowel perforation.
CT and MRI Enterography:
CT Enterography: Provides a detailed view of the small intestine and is especially useful for detecting complications like fistulas, abscesses, and strictures, more commonly in Crohn’s Disease.
MRI Enterography: Preferred in younger patients and those requiring frequent imaging due to less radiation exposure. It is effective in visualizing perianal disease and fistulas.
Barium Studies: Barium Enema and Small Bowel Barium X-ray can be used for visualizing the colon and small intestine. However, these are less commonly used today due to advancements in CT and MRI.
5. Biopsy
Biopsy samples obtained during endoscopy are vital in confirming the diagnosis and differentiating between Crohn’s Disease and Ulcerative Colitis:
Crohn’s Disease: Granulomas, transmural inflammation, and deep ulcers are often seen.
Ulcerative Colitis: Inflammation is restricted to the mucosa and submucosa, with crypt abscesses and distortion of the crypts.
6. Disease Activity Monitoring
Fecal Calprotectin: This stool marker is used to monitor disease activity and inflammation levels. Elevated levels indicate active inflammation and can help assess disease severity.
7. Other Specialized Tests
Capsule Endoscopy: This procedure involves swallowing a small camera (capsule) that takes pictures of the small intestine. It is useful in detecting Crohn’s Disease in the small bowel, particularly when endoscopic visualization is difficult.
Double Balloon Enteroscopy: A procedure that allows for deep visualization and biopsy of the small intestine, useful for diagnosing Crohn’s Disease in the small bowel.
Treatment:-
The treatment of InflammatoryBowel Disease (IBD), including both Crohn’s Disease (CD) and Ulcerative Colitis (UC), aims to control inflammation, manage symptoms, maintain remission, and prevent complications. The treatment approach involves a combination of medications, nutritional therapy, surgical interventions, and lifestyle modifications. The specific treatment plan depends on the disease type, severity, location, and patient factors.
1. Medications
a. Aminosalicylates (5-ASAs)
Examples: Mesalamine, Sulfasalazine.
Indication: Mainly used in Ulcerative Colitis (UC) to control mild to moderate inflammation. Mechanism: Reduce inflammation in the gut by inhibiting pro-inflammatory cytokines.
b. Corticosteroids
Examples: Prednisone, Budesonide.
Indication: Used for short-term flare-ups to rapidly reduce inflammation in both UC and CD.
Mechanism: Suppress immune response and inflammation, but long-term use is avoided due to side effects.
Side Effects: Weight gain, osteoporosis, increased risk of infections.
c. Immunosuppressive Drugs
Examples: Azathioprine, 6-Mercaptopurine (6-MP), Methotrexate.
Indication: Used for moderate to severe disease or when steroid use needs to be minimized. Mechanism: Suppress the immune system to reduce inflammation.
Side Effects: Increased risk of infections, liver toxicity, bone marrow suppression.
Interleukin Inhibitors:Ustekinumab (Stelara).
Indication: Used for moderate-to-severe Crohn’s Disease and Ulcerative Colitis. Mechanism: Targets interleukin-12 and interleukin-23, which are involved in inflammation. f. Antibiotics
Examples: Metronidazole, Ciprofloxacin.
Indication: Used in Crohn’s Disease for complications like abscesses, fistulas, or perianal disease. 2. Nutritional Therapy
Nutritional therapy is essential, particularly in Crohn’s Disease and severe Ulcerative Colitis. a. Exclusive Enteral Nutrition (EEN)
Indication: Often used in pediatric Crohn’s Disease to induce remission without steroids.
Mechanism: Aliquid diet rich in nutrients but free from fiber, which helps reduce gut inflammation. b. Parenteral Nutrition (PN)
Used in severe cases of Crohn’s Disease or Ulcerative Colitis when oral intake is not possible.
c. Micronutrient Supplementation
Iron, vitamin B12, folate, and vitamin D supplements are common due to malabsorption in IBD patients.
3. Surgical Treatment
Surgery may be required for patients who do not respond to medications or develop complications.
a. Surgery for Crohn’s Disease
Resection of affected bowel segments may be necessary, especially in cases of strictures or fistulas.
Surgery does not cure Crohn’s Disease, and recurrence of disease can occur at other sites.
b. Surgery for Ulcerative Colitis
Proctocolectomy: Removal of the colon and rectum, which is curative for UC.
Ileal Pouch-Anal Anastomosis (IPAA): Creates a new rectum from the small intestine, allowing normal defecation.
Ileostomy: In some cases, a permanent stoma is created if pouch surgery is not possible.
4. Lifestyle Modifications and Supportive Care
a. Stress Management and Support
Psychosocial support and stress management are important, as stress can exacerbate symptoms.
Support groups and therapy can help manage the emotional impact of IBD. b. Smoking Cessation
Crohn’s Disease is aggravated by smoking, so quitting is essential for disease control. c. Regular Exercise
Exercise can help reduce fatigue and improve overall well-being.
d. Dietary Adjustments
Avoiding trigger foods (e.g., spicy, fatty, or high-fiber foods) may alleviate symptoms. Low-residue diet may be recommended during active disease to reduce bowel irritation.
Complications
Inflammatory Bowel Disease (IBD), which includes both Crohn’s Disease (CD) and Ulcerative Colitis (UC), can lead to a variety of complications that affect the gastrointestinal tract, extra-intestinal organs, and overall health. These complications can arise due to the chronic inflammation associated with IBD or as a result of treatments used to manage the disease.
1. Gastrointestinal Complications
a. Strictures
Chronic inflammation in Crohn’s Disease can lead to the formation of strictures (narrowing of the bowel).
b. Fistulas
Abnormal connections between different parts of the intestines, or between the intestine and other organs
c. Abscesses
Collection of pus due to infection or inflammation.
d. Toxic Megacolon
A severe and potentially life-threatening condition where the colon becomes massively dilated. e..Perianal Disease
Inflammation or infection around the anus, common in Crohn’s Disease.
f. Colorectal Cancer (CRC)
Patients with longstanding Ulcerative Colitis or Crohn’s Disease have an increased risk of developing colorectal cancer, particularly after 8-10 years of disease.
2. Extra-intestinal Complications
a. Arthritis
: Joint inflammation, often seen in IBD patients.
Immune system dysfunction can lead to joint pain and inflammation.
b. Ocular Complications
Inflammation of the eyes, including uveitis (inflammation of the middle layer of the eye) and episcleritis (inflammation of the tissue covering the eye).
d. Primary Sclerosing Cholangitis (PSC)
A liver disease where the bile ducts become inflamed and scarred, often seen in patients with Ulcerative Colitis.
Chronic inflammation of bile ducts, leading to liver damage.
e. Kidney Stones
Formation of stones in the kidneys due to malabsorption of calcium and oxalate.
3. Systemic Complications
a. Malnutrition
Inflammation, diarrhea, and malabsorption can lead to nutrient deficiencies.
Decreased nutrient absorption from the intestine due to inflammation, as well as reduced food intake.
b. Blood Clots (Thrombosis)
Patients with IBD, particularly those with severe disease or active inflammation, have an increased risk of deep vein thrombosis (DVT) and pulmonary embolism (PE).
4. Other Complications
a. Growth Retardation in Children
Cause: Chronic inflammation, malnutrition, and steroid use in pediatric IBD patients can impair growth and development.