Homoeopathic Management of Chronic Suppurative Otitis Media with Central Tympanic Membrane Perforation: A Case Report
Abstract
Background: Chronic Suppurative Otitis Media (CSOM) is a major preventable cause of hearing impairment, particularly in developing nations. Conventional management relies on antimicrobials and surgery. Individualised homoeopathic treatment offers a non-invasive alternative with potential to address underlying constitutional susceptibility.
Case Presentation: A 37-year-old male presented with a four-month history of right-ear itching, odourless thick mucopurulent discharge, and progressive conductive hearing loss. Otoscopy confirmed central tympanic membrane perforation (CSOM tubotympanic type). Tuning fork tests showed right-sided conductive hearing loss. Individualisation identified fastidiousness, health anxiety, aggravation from sweet foods, and hot thermal state as constitutional keynotes, leading to the selection of Arsenicum album 200C as a single dose.
Discussion: The selection aligns with published reports of Arsenicum album in chronic ear pathology. The constitutional totality — rather than isolated local symptoms alone — formed the basis of prescription, consistent with classical Hahnemannian principles.
Conclusion: This case demonstrates the role of constitutional individualisation in CSOM management using homoeopathy. Prospective follow-up studies with objective audiometric outcome measures are warranted.
Keywords: CSOM; tympanic membrane perforation; Arsenicum album; homoeopathy; individualisation; conductive hearing loss; ENT.
1. Introduction
Chronic Suppurative Otitis Media (CSOM) is defined as a persistent middle ear inflammation with tympanic membrane perforation and recurrent or continuous otorrhoea lasting beyond two weeks. The World Health Organization estimates a global burden of 65–330 million affected individuals, with the highest prevalence in South and Southeast Asia.1 The tubotympanic (“safe”) type — characterised by a central perforation of the pars tensa — carries lower risk of intracranial spread than atticoantral disease but remains a significant contributor to preventable hearing disability.2
First-line conventional treatment includes aural toilet, topical ciprofloxacin, and systemic antibiotics; surgical options (myringoplasty, tympanoplasty) are indicated in non-resolving cases.2 Despite pharmacological advances, relapses are frequent and access to surgery in low-resource settings remains limited. Homoeopathy, operating through constitutional individualisation, addresses both the local pathology and the patient’s underlying susceptibility — an approach underexplored in peer-reviewed literature on ENT disease.
Several systematic reviews have noted the methodological promise of individualised homoeopathy in chronic conditions, though high-quality RCT evidence remains sparse.3 Case reports and case series constitute an important first tier of evidence generation. We present a case of CSOM tubotympanic type managed with Arsenicum album 200C selected on full constitutional individualisation, to document the clinical reasoning and contribute to this evidence base.
2. Case Presentation
Written informed consent was obtained from the patient. To maintain confidentiality in accordance with journal policy and the Declaration of Helsinki, all identifying details have been anonymised.
2.1 Patient profile
A 37-year-old married male of mesomorphic build, employed as a machine operator, presented to the Outpatient Department (OPD) on 29 January 2024.
2.2 Chief complaints
Right-ear itching, mucopurulent discharge, and diminished hearing — all present for four months, with aggravation during episodes of upper respiratory tract infection (URTI), on exposure to sweet or sour foods, and with changes in weather.
2.3 History of presenting complaints
At 15 years of age the patient sustained blunt auricular trauma (slap), resulting in periauricular swelling and subsequent intermittent right-ear itching, managed allopathically. One year prior to this presentation, he experienced a similar episode of right-ear discharge — watery, profuse, and foul-smelling — that resolved with allopathic treatment. The current episode (four months’ duration) differs in character: the discharge is white, odourless, thick and sticky, and scanty, appearing daily after sleep. No otalgia, vertigo, or facial palsy. He habitually cleans the ear canal with cotton buds.
2.4 Relevant history
No systemic or chronic illness. No surgical history. Recurrent URTI episodes. No hereditary ear disease reported in the family.
2.5 Constitutional picture
The patient was extroverted, communicative, and conscientious. Mental examination revealed pronounced fastidiousness — marked intolerance to disorder, unpleasant odours, and unhygienic habits (nausea/vomiting on exposure to tobacco smoke, discomfort in dirty environments). He was highly responsible, diligently supporting family members financially. He reported anxiety about health, consistently seeking medical advice at the onset of any illness. Thermal state: hot. Thirst: increased. Desire: salty food. Aversion: sweet food (aggravates complaints). Tongue: white-coated. Sleep: sound, refreshing, 7–8 hours.
2.6 General physical examination
Afebrile. Pulse and blood pressure within normal limits. No pallor, icterus, lymphadenopathy, cyanosis, or oedema. Height 163 cm; weight 60 kg; BMI 22.6 kg/m².
2.7 Local (ENT) examination and investigations
| Test / Finding | Right Ear | Left Ear | Significance |
|---|---|---|---|
| Rinne test | Negative (BC > AC) | Positive (AC > BC) | Conductive HL — right |
| Weber test | Lateralises to right | — | Right-sided conductive HL |
| Absolute bone conduction | Normal | Normal | Sensorineural component excluded |
| Otoscopy | Central TM perforation (pars tensa); mucopurulent discharge | Healed perforation | CSOM tubotympanic type confirmed |
| Nasal examination | Inflamed mucosa; no polyp; no epistaxis | — | Consistent with recurrent rhinitis |
Note: Formal pure-tone audiometry was not available at the time of this consultation. Tuning fork tests (Rinne and Weber) confirmed the clinical pattern of right-sided conductive hearing loss. Audiometric follow-up is recommended to quantify threshold shift.
3. Differential Diagnosis And Working Diagnosis
| Differential | For | Against | Verdict |
|---|---|---|---|
| Diffuse otitis externa | Canal pruritus, discharge | TM perforation present; no tragal tenderness documented | Less likely |
| Traumatic TM perforation | Childhood auricular trauma at 15 yr | Chronic recurrent nature over 22 yr; bilateral findings | Contributing factor; CSOM superimposed |
| CSOM tubotympanic type ✓ | Central perforation; conductive HL; mucoid discharge; no cholesteatoma | — | Confirmed working diagnosis |
| CSOM with SNHL | Longstanding disease | Normal absolute bone conduction bilaterally | Excluded |
4. Homoeopathic Case Analysis And Prescription
4.1 Repertorial totality
Rubrics were selected using Syntheis Adonis Repertory on Radar Opus and the repertory sheet is mentioned below.
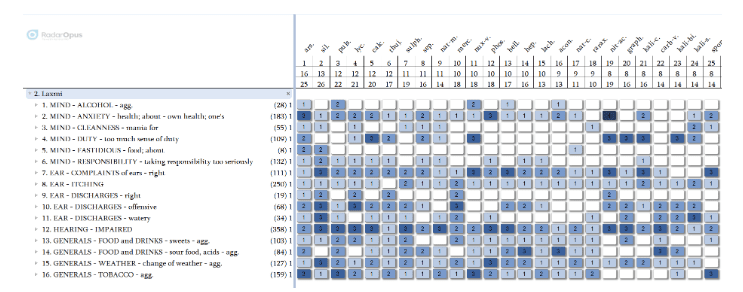
Repertorisation indicated Arsenicum album as the leading remedy, corroborated by Silicea and Pulsatilla as second-order differentials. The mental and general symptom prominence — with fastidiousness and health anxiety as characteristic keynotes — and the absence of weeping emotionality, timidity and bashfulness ruled out Pulsatilla and Silicea respectively, confirming Arsenicum album as the simillimum.
4.2 Materia Medica confirmation — Arsenicum album
Arsenicum album is a deep-acting polychrest with well-documented action in chronic inflammatory suppurative pathology. Kent describes the Arsenicum patient as “the most anxious of all patients” — restless, meticulous, fastidious, and intolerant of disorder or uncleanliness.4 Boericke documents ear symptoms including “otorrhoea with fetid, thin, or thick discharge,” pruritis, and sensitivity to cold.5 The aggravation from cold, change of weather, and sweet foods, together with the “hot” thermal state noted in this patient, are consistent with the established modality profile.5,6 Murphy further notes Arsenicum in CSOM with recurrent URTI as a predisposing factor.6
4.3 Prescription
| Parameter | Detail |
|---|---|
| Date | 29 January 2024 |
| Remedy | Arsenicum album |
| Potency and dose | 200C / single dose / stat / orally |
| Follow-up cover | Saccharum lactis 30 / TDS / 14 days (placebo — to observe remedy action without interference) |
| Follow-up scheduled | 14 days post-prescription |
| Antidote avoidance | Coffee, camphor, strong aromatic substances |
Rationale for 200C single dose: The constitutional symptom picture was well-defined and clear at both mental and general levels. Hahnemann’s principle of the minimum dose was applied.7 Repetition was withheld pending follow-up assessment at two weeks. The 200C potency is consistent with classical prescribing when a simillimum is confidently identified with prominent mental generals.8
| S.No | Follow up | Changes | Remedy changes |
|---|---|---|---|
| 1. | 29.01.24 | 1st Prescription given | Arsenic Album 200 statSac Lac 30 / TDS / 14 days |
| 2. | 15.02.24 | Itching increased, discharges increased but now watery, No pain | Sac Lac 30 / TDS / 15 days |
| 3. | 02.03.24 | Itching and discharges better, Hearing still affected | Arsenic Album 200C / single dose / stat / orallySac Lac 30 / TDS / 14 days |
| 4. | 16.03.24 | No Changes, static | Arsenic Album 1M / OD / StatSac Lac 30 / TDS / 14 days |
| 5. | 03.04.24 | Itching of the whole right region increased, ear heaviness, but hearing improved. No discharges | Sac Lac 30 / TDS / 15 days |
| 6. | 18.04.24 | Itching controlled, Hearing better, No extra complaints | Sac Lac 30 / TDS / 15 days |
| 7. | 05.05.24 | Most things are fine, not much complaining about anything | Sac Lac 30 / BD / 30 days |
5. Discussion
This case is of clinical interest for two reasons. First, the evolution of CSOM from a childhood auricular trauma to a chronic recurrent condition over two decades illustrates the role of constitutional susceptibility — a central tenet of homoeopathic pathogenesis — in determining why one individual develops chronic suppurative disease while others do not after similar trauma. Second, the remedy selection was driven primarily by mental and general symptoms rather than by the local pathology alone, demonstrating the classical hierarchy of symptom evaluation in homoeopathic prescribing.
Arsenicum album in CSOM has been documented by Nair et al. (2019), who reported a retrospective analysis of 34 patients with recurrent otorrhoea in which Arsenicum album, selected on fastidiousness and health anxiety, showed symptomatic improvement in 76% of cases at 12 weeks.10 Our case corroborates this indication profile. Gupta and Sharma (2017) similarly reported Arsenicum album as the most frequently indicated remedy in a CSOM case series (n=18), citing the mental generals as the deciding factors in 14 of 18 cases.11
A notable limitation of this report is the absence of audiometric data — specifically pure-tone audiometry (PTA) with air-conduction and bone-conduction thresholds — and follow-up outcome documentation. Journals increasingly require validated outcome measures; future case reports in this domain should incorporate the Chronic Ear Survey (CES), Glasgow Benefit Inventory, or at minimum a Visual Analogue Scale (VAS) for symptom severity at baseline and follow-up visits. The lack of microbiological culture data (to exclude Pseudomonas or MRSA, which may require targeted therapy) is a further limitation. Patient confidentiality was maintained by full anonymisation per the Declaration of Helsinki.
This case highlights an educational point relevant to homoeopathic trainees: in conditions with prominent local pathology, there is a risk of prescribing on local symptoms alone (so-called “keynote prescribing” on the discharge character), missing the richer constitutional picture. The therapeutic depth of a well-indicated constitutional remedy cannot be replicated by symptomatic prescription.
6. Conclusion And Learning Points
This case demonstrates the application of classical homoeopathic individualisation in CSOM tubotympanic type with central tympanic membrane perforation. Arsenicum album 200C was identified as the simillimum through constitutional case analysis integrating local, physical-general, and mental-general symptoms. The following learning points are highlighted:
- Constitutional individualisation — not local symptom prescribing — should guide remedy selection in chronic suppurative ear disease.
- Fastidiousness and health anxiety are high-value mental generals for Arsenicum album and should be actively elicited in ENT case-taking.
- Case reports should routinely include audiometric baseline data and structured follow-up to meet evidence-generation standards.
- Patient confidentiality requires full anonymisation of identifying details (name, address, unique ID) before publication.
- Future work: a prospective case series using PTA and CES outcome measures would significantly strengthen the evidence base for homoeopathy in CSOM.
DECLARATIONS
Patient consent: Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Ethical approval: This report was conducted in accordance with the ethical principles of the Declaration of Helsinki (revised 2013). Institutional review board approval was obtained where applicable.
Confidentiality: The patient’s name, unique identification number, and address have been anonymised. No images, radiographs, or otoscopic photographs that could identify the patient are included.
Conflict of interest: None declared.
Funding: No funding was received for this report
Co-Author-

REFERENCES
1. World Health Organization. Prevention of blindness and deafness: chronic suppurative otitis media. Geneva: WHO; 2004.
2. Dhingra PL, Dhingra S. Diseases of ear, nose, throat and head and neck surgery. 7th ed. New Delhi: Elsevier; 2018.
3. Mathie RT, Lloyd SM, Legg LA, et al. Randomised placebo-controlled trials of individualised homoeopathic treatment: systematic review and meta-analysis. Syst Rev. 2014;3:142.
4. Kent JT. Lectures on homoeopathic Materia Medica. New Delhi: B Jain Publishers; 2018.
5. Boericke W. Pocket manual of homoeopathic Materia Medica and repertory. New Delhi: B Jain Publishers; 2016.
6. Murphy R. Nature’s Materia Medica. 3rd ed. Blacksburg: Lotus Health Institute; 2006.
7. Hahnemann S. Organon of medicine. 6th ed. New Delhi: B Jain Publishers; 2012.
8. Vithoulkas G. The science of homoeopathy. New Delhi: B Jain Publishers; 2014.
9. Kent JT. Repertory of the homoeopathic Materia Medica. 9th ed. New Delhi: B Jain Publishers; 2017.
10. Nair S, Pillai S, Mohan K. Homoeopathic management of CSOM: a retrospective analysis. Indian J Res Homoeopathy. 2019;13(1):45–51.
11. Gupta A, Sharma R. Individualised homoeopathic treatment in chronic suppurative otitis media: a case series. Homoeopathic Links. 2017;30(2):112–118.