
“PITYRIASIS VERSICOLOR: A CASE REPORT DEMONSTRATING THE EFFICACY OF HOMOEOPATHIC TREATMENT”
ABSTRACT- Pityriasis versicolor (PV) is a frequently occurring superficial cutaneous fungal disorder resulting from excessive proliferation of Malassezia species. It presents clinically as hypopigmented or hyperpigmented, finely scaly macules, most commonly involving the trunk, neck, and upper extremities. Although the condition is benign, its chronic and recurrent nature often leads to cosmetic concern, psychological distress, and reduced quality of life. Conventional management primarily focuses on antifungal therapy, which may provide temporary relief but is frequently associated with recurrences, whereas individualized homeopathic treatment aims to address the root cause and promote holistic healing.
KEYWORDS: Pityriasis versicolor, superficial skin infection, homoeopathy, individualized treatment, Malassezia.
DEFINATION:
Synonyms
• Tinea versicolor
• Dermatomycosis furfuracea
• Tinea flavea
• Liver spots
• Chromophytosis
Tinea versicolor is a superficial fungal infection caused by Malassezia furfur, a non-dermatophytic dimorphic fungus that normally resides on human skin. Its pathogenic manifestation is favoured by conditions such as heat and humidity. Clinically, it presents as oval, finely scaly macules, papules, or patches, predominantly involving the chest, shoulders, and back, while the face and distal extremities are infrequently affected. In individuals with darker skin tones, the lesions commonly appear hypopigmented, whereas in those with lighter skin, they tend to be mildly erythematous or hyperpigmented.
The area’s most often affected by pityriasis versicolor include the:
• Back
• Chest
• Upper arms
• Neck
• Proximal extremities
EPIDEMIOLOGY: Tinea versicolor has a worldwide prevalence of up to 50% in the hot and humid environments and as low as 1.1% in colder climates. Incidence of tinea versicolor is the same in all races, no sex predominance is apparent. Tinea versicolor is most common among adolescents and young adults, in whom lipid-producing sebaceous glands are more active.
CAUSES: Pityriasis versicolor is caused by the overgrowth of lipophilic yeasts belonging to the genus Malassezia, which form part of the normal cutaneous flora. Earlier classified under the genus Pityrosporum, these organisms are now recognized as a complex group of genetically distinct species. Advances in molecular taxonomy have identified more than twelve Malassezia species, of which M. globosa, M. sympodialis and M. furfur are most commonly associated with human skin and pityriasis versicolor.
CLINICAL FEATURES:
- A person is likely to notice tinea versicolor only when spots start to appear on the skin. These spots may be lighter or darker than the surrounding skin, and are often more noticeable when the surrounding skin is tan.
- Though most common around the trunk and neck, these spots may appear anywhere on the body.
- Itchy patches of spots.
- Spots that grow slowly over time, potentially forming into patches.
- Symptoms may disappear or become reduced in cooler weather and may return when the weather becomes hot and humid.
- Clinical findings: red scratchy scabs over back, nape of neck.
- Patients with pityriasis versicolor present with multiple, well-demarcated, oval, finely scaling patches or plaques.
- Skin lesions may be hypopigmented, hyperpigmented, or erythematous and occasionally become confluent and widespread.
- Patches of skin may be darker or lighter than your normal skin colour.
- Patches can also be red, brown or pink.
DIAGNOSIS: Pityriasis versicolor can be clinically diagnosed by its characteristic skin lesions (erythematous, hyperpigmented or hypopigmented, finely scaling, thin plaques). the fine scale on the affected skin is not easily seen but becomes more apparent when the skin is stretched or scraped (the “evoked scale sign”). This sign is helpful in confirming a diagnosis of pityriasis versicolor. Microscopic confirmation is helpful when there is uncertainty about the diagnosis. It is not useful diagnostically after the patient is treated since it will be negative in most cases. Pretreatment diagnosis can be confirmed by microscopic examination of skin scrapings treated with potassium hydroxide or stained with Swartz Lamkin or chlorazol black. Using stains allows for easier identification of fungal forms and can be helpful for clinicians who infrequently examine slides. Alternatively, scrapings can be sent to a laboratory with a request for fungal microscopy. examination of prepared slides reveals numerous spores and hyphae that resemble “spaghetti and meatballs.
DIFFERENTIAL DIAGNOSIS- Pityriasis versicolor may be confused with various conditions:
• Pityriasis rosea
• Tinea corporis
• Vitiligo
• Pityriasis alba
• Post inflammatory hypo- and hyperpigmentation
HOMOEOPATHY APPROACH FOR PITYRIASIS VERSICOLOR
Homeopathy aims to address the underlying factors that contribute to conditions like pityriasis versicolor, such as imbalances in the body’s internal environment. Homeopathic remedies are selected based on individual symptoms, overall health, and constitutional factors. The holistic approach of homeopathy can help in managing symptoms, preventing recurrence, and improving overall skin health.
Following are the few homeopathic medicines used in PV:-
1. SULPHER
2. PSORINUM
3. BACILLINUM
4. NATRUM MURITICUM
5. TELLURIUM
6. SEPIA
7. ARSENIC ALBUM
8. MEZEREUM
9. GRAPHITES
10. KALI SULPH
11. THUJA
CASE HISTORY
A 28 old female patient presented with complaints of
- Hypopigmented scaly patches around the neck for 3 months
- mild itching < night & after sweating
- recurrence in every summer
- Treated repeatedly with topical steroid ointments
- Temporary relief followed by recurrence
HISTORY OF PRESENT ILLNESS
The patient reported gradual onset of whitish patches around the neck, spreading slowly to the chest. The lesions were mildly itchy and worsened after perspiration. No history of systemic illness.
PHYSICAL GENERALS
- Appetite: Normal
- Desires/ craving: spicy food
- Aversions /intolerance: Not specific
- Bowels: constipated/hard stool
- Micturition: Normal
- Perspiration: profuse
- Sleep: Disturbed.
- Dreams: Not significant
- Thermal: Hot pt.
MENTALS
- irritable over small matters.
- Negligent of hygiene, dislikes bathing.
- Heat intolerance, becomes mentally uncomfortable in warmth.
- Egotistical, slight intellectual pride.
- Lazy / low motivation for routine tasks.
- Oversensitive to criticism, easily hurt.
- Introverted, prefers solitude.
OBS/GYNAE HISTORY
- Age at Menarche: 13 years
- Cycle Pattern: Regular
- Cycle Length: 28–30 days
- Duration of Flow: 3–4 days
FAMILY HISTORY
- Father: Diabetes
- Mother: Hypothyroidism
GENERAL EXAMINATION
- General Development and Nutrition: Normal
- Tongue: Slightly coated
- BP -120/80 mm/hg
- Respiration:16/min
- Pulse: 82bpm
- Spo2: 99% on RA
- Temperature (oral): Afebrile
- Weight: 51kg
SYSTEMIC EXAMINATION:
- CVS: S1S2+,
- CNS: Conscious & Oriented
- RS: BLAE+
Dermatological Examination
- Skin: Dry
- Skin Lesion Morphology:
- Lesion Type, Size: Scaly hypopigmented
- Configuration/Shape: irregular
- Colour, Texture: whitish
- Distribution: neck
TOTALITY OF SYMTOMS:
- Irritability
- Fear of ghosts
- Anxiety in the evening
- Profuse perspiration
- Sensation of heat / intolerance to heat
- Constipation with hard stool
- Discoloration of skin with white spots
- Scaly eruptions
- Itching < in bed, especially on becoming warm
REPERTORISATION:
- MIND – irritability
- MIND – fear -ghosts -of
- MIND- anxiety -evening
- MIND -impatience
- SKIN – discoloration – white spots
- SKIN – eruptions – scaly
- SKIN – itching – warm – worse in bed- on becoming
- PERSPIRATION – profuse
- STOOL – hard
- GENERALITIES – heat – sensation of
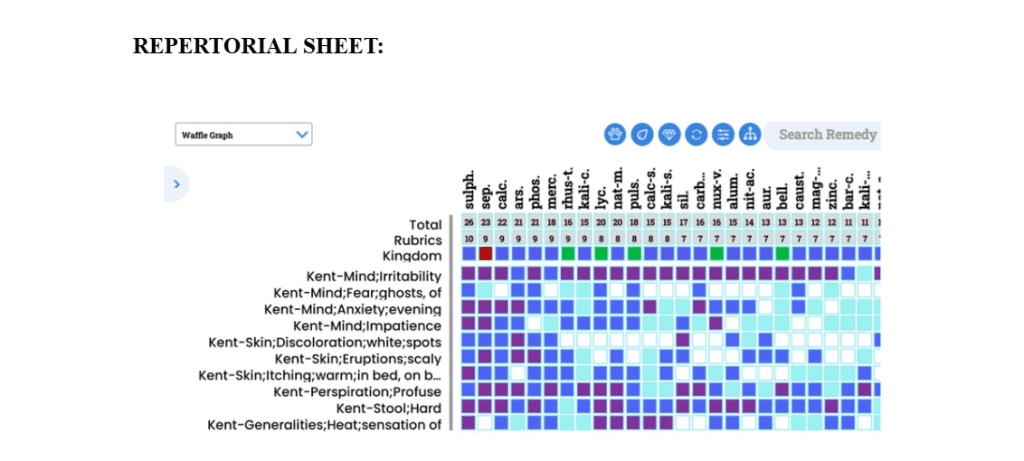
After repertorizing from synergy repertory, the medicine containing higher grade and covering maximum symptom was sulphur.
First Prescription (10/12/2025): -Based on the repertorial result and symptoms similarity Sulphur 30, OD for 2 days and sac lac 30-BD For 15 days. Follow up assessment was done for every 15 days.
Diet and Regime: Restrict Spicy, oily food, meat. Take high fiber foods and adequate amount of water.
FOLLOW UP:
| DATE | OBSERVATION | PRESCRIPTION |
| 27/12/25 | Relived 30% in itching | SAC LAC 30 BD FOR 15 DAYS |
| 12/01/26 | Patches size reduced | SULPHUR 30 OD for 2 DAYS |
| 28/01/26 | Patches size reduced | SAC LAC 30 BD FOR 15 DAYS |
| 16/02/26 | improved | SULPHUR 200 SINGLE DOSE |
| 05/03/26 | All patches disappear | SAC LAC 200 FOR 15 DAYS |

COMMENT:
The patient showed gradual improvement during the 3 months of treatment. Itching reduced first, and the hypopigmented patches slowly faded. By the end of 3 months, all symptoms had completely disappeared. Sulphur 30/200 helped in relieving the skin complaints effectively. During the follow-up period, Sac lac was given to maintain improvement. Preventive advice was explained to the patient to avoid recurrence. The treatment was successful, and normal skin was restored by the end of the follow-up period.
CONCLUSION:
Homoeopathy offers an effective and holistic approach in the management of Pityriasis Versicolor by enhancing the body’s natural healing mechanisms, minimizing recurrence, and improving the patient’s overall well-being. Further clinical studies and case-based evidence can strengthen the role of homoeopathy in dermatological conditions like Pityriasis Versicolor.
REFERENCES:
- Longo D, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J. Harrisons Manual of Medicine. 18th ed. New York, NY: McGraw-Hill Medical; 2012.
- Goldsmith LA, Katz SI, Gilchrest BA, Paller A, Leffell DJ, Wolff K. Fitzpatrick’s dermatology in general medicine, eighth edition, 2 volume set. 8th ed. New York, NY: McGraw-Hill Medical; 2012.
- Burns T, Breathnach SM, Cox NH, Griffiths C, editors. Rook’s textbook of dermatology. 8th ed. Chichester, England: Wiley-Blackwell; 2010
- Khanna N. Illustrated synopsis of dermatology & sexually transmitted diseases-ebk. 6th ed. New Delhi, India: Elsevier; 2019.
- Boericke W. Pocket manual of homeopathic materia medica & repertory. New Delhi, India: B Jain; 2023.
- Shannon SF. A complete repertory of the tissue remedies of Schussler. Legare Street Press; 2022.
- Allen HC. Allens’ keynotes: Rearranged & classified. New Delhi, India: B Jain; 2024.
- Kent JT. Lectures on homoeopathic materia medica: Together with Kent’s “new remedies” incorporated & arranged in one alphabetical order. New Delhi, India: B Jain; 2023.
- Clarke JH. Grand Characteristics of Materia Medica. New Delhi, India: B Jain; 2001.
Author:
Dr. Hemant Masar , MD Scholar
Dept. Of Practice of Medicine – Govt. Homoeopathic Medical College & Hospital Bhopal (MP)
Guided By –
Dr. Praveen Jaiswal, M.D., PhD (Hom.)
Professor & HOD – Govt. Homoeopathic Medical College & Hospital Bhopal (MP)

