Role of Homoeopathic Medicine in Irritant Contact Dermatitis: A Clinical Perspective with Quality of Life Assessment Using DLQI
Abstract
Irritant Contact Dermatitis (ICD) is a common inflammatory skin disorder resulting from direct chemical or physical injury to the epidermal barrier. It accounts for a significant proportion of occupational dermatoses and adversely affects physical comfort, productivity, and psychosocial well-being. Conventional treatment primarily focuses on avoidance of irritants and symptomatic control using topical corticosteroids and emollients; however, recurrence is frequent. Homoeopathy, based on the principle of individualisation, offers a holistic therapeutic approach addressing both local pathology and constitutional susceptibility. This article elaborates on etiology, pathogenesis, clinical features, homoeopathic therapeutics, miasmatic understanding, preventive aspects, and the importance of Dermatology Life Quality Index (DLQI) in assessing patient-centered outcomes. Individualised homoeopathic treatment may contribute to symptomatic improvement, reduction in recurrence, and enhanced quality of life.
Keywords
Irritant Contact Dermatitis, Individualised Homoeopathy, DLQI, Occupational Dermatitis, Materia Medica, Miasmatic Approach, Quality of Life
Introduction
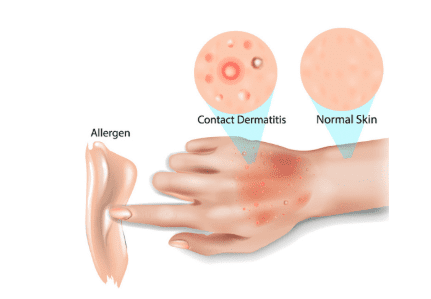
Irritant Contact Dermatitis is a non-immunological inflammatory reaction of the skin caused by repeated exposure to irritants such as soaps, detergents, acids, alkalis, solvents, disinfectants, and prolonged wet work. It constitutes nearly 80% of occupational contact dermatitis cases. Individuals working in healthcare, cleaning services, food handling, agriculture, construction, and hairdressing are particularly vulnerable.
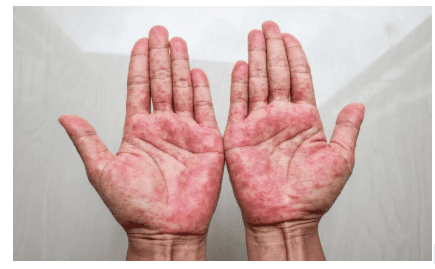
The disease predominantly affects exposed areas, especially the hands. Although often considered a local condition, ICD significantly impacts daily functioning, social interaction, and emotional stability. Visible lesions, persistent itching, and burning sensations can lead to frustration, anxiety, and decreased self-esteem.
Etiology and Risk Factors
ICD results from cumulative irritant exposure. Factors contributing include: frequency and duration of contact, concentration of irritant, environmental humidity, temperature variations, and individual susceptibility such as atopic tendency. Repeated wet-to-dry cycles damage the lipid barrier of the stratum corneum, increasing vulnerability.
Pathogenesis
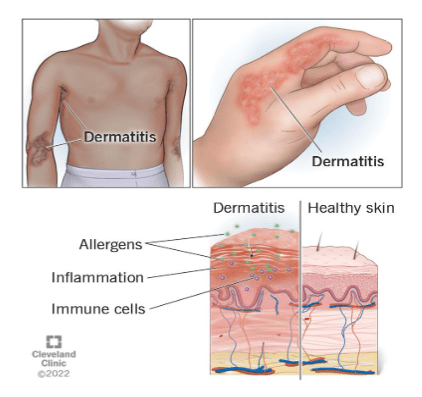
The primary event in ICD is disruption of the epidermal barrier. Damage to keratinocytes triggers release of pro-inflammatory cytokines including IL-1 and TNF-α. This initiates vasodilation, increased vascular permeability, and leukocyte infiltration. Chronic exposure leads to hyperkeratosis, scaling, fissures, and lichenification.
Clinical Features
Clinical manifestations vary from mild erythema and dryness to severe vesiculation and fissuring. Acute ICD presents with burning, stinging, and oedema, whereas chronic cases show thickened skin, cracks, and exaggerated skin markings. Subjective symptoms such as tightness and smarting often interfere with occupational duties.
Conventional Management and Limitations
Management involves avoidance of irritants, use of protective gloves, barrier creams, emollients, and topical corticosteroids. Severe cases may require systemic therapy. Though effective for short-term control, relapse is common if exposure persists. Long-term corticosteroid use may lead to skin atrophy and dependency.
Homoeopathic Approach
Homoeopathy treats ICD through individualisation, considering the totality of symptoms. Prescription is based on location, sensation, modalities, concomitants, mental state, constitutional traits, and miasmatic background. The aim is restoration of internal balance and reduction of susceptibility rather than mere suppression.
Miasmatic Understanding in ICD
From a miasmatic perspective, ICD commonly reflects a predominance of Psora, manifesting as itching, dryness, and functional disturbance. Chronic fissures and thickening may suggest sycotic influence, while ulcerative or destructive changes may point towards syphilitic tendencies. Accurate miasmatic evaluation guides long-term constitutional prescribing.
Important Homoeopathic Remedies
Anacardium orientale –
Intense itching with vesicular eruptions, marked irritability, and sensation of a plug-like feeling. Skin may show neurotic eczema tendencies with mental conflict.
Remedy selection must always be individualised according to totality rather than based solely on diagnosis.
Arsenicum album –
Burning pains better by warmth, restlessness, anxiety, and dry scaly eruptions. Suited to debilitated patients with marked prostration.
Remedy selection must always be individualised according to totality rather than based solely on diagnosis.
Causticum –
Raw, cracked, fissured skin especially on hands; burning relieved by warmth; dermatitis after exposure to detergents.
Remedy selection must always be individualised according to totality rather than based solely on diagnosis.
Mezereum –
Thick crusts with pus beneath; violent itching worse at night; useful in chronic steroid-suppressed eczema.
Remedy selection must always be individualised according to totality rather than based solely on diagnosis.
Rhus toxicodendron –
Red, swollen vesicular eruptions with intense itching better by warmth; useful in acute inflammatory dermatitis.
Remedy selection must always be individualised according to totality rather than based solely on diagnosis.
Sulphur –
Burning itching aggravated by heat and washing; tendency to recurrence; suited to chronic cases with unclean skin appearance.
Remedy selection must always be individualised according to totality rather than based solely on diagnosis.
Assessment Using Dermatology Life Quality Index (DLQI)
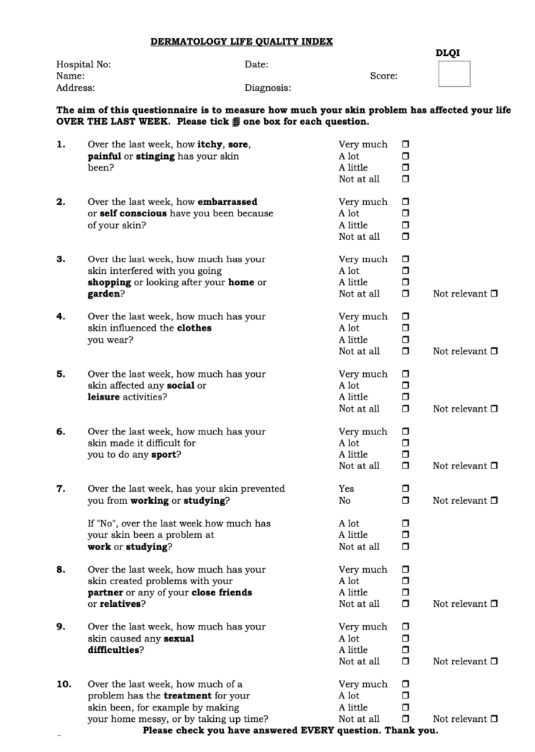
The Dermatology Life Quality Index (DLQI) is a validated 10-item questionnaire assessing impact of skin disease on symptoms, daily activities, leisure, work, relationships, and treatment burden. Scores range from 0 to 30. Reduction in score reflects meaningful improvement in quality of life. Incorporating DLQI allows objective measurement of patient-perceived benefit.
Preventive and Patient Education Aspect
Patient education plays a crucial role in preventing recurrence. Advice includes minimizing wet work exposure, using protective gloves appropriately, avoiding harsh soaps, applying moisturizers regularly, and maintaining skin hydration. Homoeopathic management combined with preventive measures enhances long-term outcomes.
Discussion
ICD significantly influences psychological and social dimensions. Individualised homoeopathic treatment addresses both constitutional susceptibility and local pathology. Integration of DLQI scoring bridges the gap between clinical improvement and patient-reported outcomes, making evaluation measurable and scientific.
Conclusion
Individualised homoeopathic management provides a holistic approach in Irritant Contact Dermatitis. By addressing the totality of symptoms and evaluating outcomes through DLQI, clinicians can assess improvement in both clinical signs and quality of life. Further large-scale studies are encouraged to strengthen the evidence base.
Co-Author:-
Dr. Vishal Shah – PG Scholar, C.D. Pachchigar College of Homoeopathic Medicine & Hospital, Surat.