Beyond Percentiles: Rethinking Growth Monitoring in Children with Neuro-Developmental Disorders (NDDs) as well as Enumerating the Viewpoint of Individualized Homoeopathic Management in this Spectrum
ABSTRACT:
Standard paediatric growth charts are widely used for assessing child health. However, their rigid application may be misleading in children with Neuro-Developmental Disorders (NDDs). Such charts primarily emphasize anthropometric indices and often fail to account for the complex neurobiological, metabolic, and functional variations inherent in this population.
Objective:
To reinterpret growth assessment in children with NDDs by moving beyond percentile-based valuation toward a functional, individualized framework while highlighting the potential role of Individualized homoeopathic intervention as a supportive therapeutic approach.
Discussion:
Children with NDDs including Autism Spectrum Disorder, Cerebral Palsy, Down Syndrome, and Attention Deficit Hyperactivity Disorder frequently exhibit growth patterns that differ from neurotypical norms due to altered feeding behavior, assimilation, metabolism, and genetic or inherited predispositions. Strict adherence to conventional growth percentiles may
lead to misdiagnosis of ‘Failure to Thrive’, unnecessary nutritional interventions, and increased caregiver anxiety. A shift from quantity-based measures (weight and height) to quality-based indicators such as functional well-being, immunity, energy levels, and developmental progress is therefore warranted. Given the multifactorial nature of NDDs, Individualized Homoeopathic treatment, grounded in constitutional assessment and miasmatic considerations, seeks to address underlying assimilation and metabolic disturbances rather than isolated anthropometric deviations.
Conclusion:
Growth monitoring in children with Neuro-Developmental Disorders should prioritize functional health and individualized developmental potential over rigid percentile conformity. Integrating Individualized Homoeopathic treatment with growth assessment may offer a holistic, child-centred approach that supports optimal assimilation, development and overall
well-being, thereby redefining ‘Normal growth’ within this unique paediatric population.
KEYWORDS: Beyond Percentiles, Neuro-Developmental Disorders (NDDS), Growth Monitoring in Children, Individualized Homoeopathy.
I. Introduction:
Growth monitoring and promotion (GMP) follows the growth of children by periodic, frequent anthropometric measurements that are compared with an appropriate standard to assess the adequacy of the child’s growth. The measurements are visualized by plotting them on a growth chart and used for promotion activities in the form of tailored, individual counselling for parents. Although there is no generally accepted set of GMP purposes, the literature identifies 3 of them, broadly, stated as: i) Diagnosis of or Screening for inadequate individual child growth ii) Growth promotion activities, population-level monitoring and surveillance & iii) Promotion of the use of other health and nutrition services such as immunization and family planning.1
Although growth monitoring and GMP programs have been widely implemented for many decades, their appropriateness and effectiveness have been questioned and challenged repeatedly since the 1980s. Key controversial points relate to the lack of clarity on what growth monitoring and particularly promotion in GMP should entail, divergence of opinion about the specific purposes and hypothesized paths of impact of GMP, poor quality measurements potentially leading to incorrect diagnostics and other implementation constraints including in high-income countries and low coverage2,3.
Neurodevelopmental Disorder or Neuro-Disability, encompasses a broad spectrum of congenital or acquired long-term conditions arising from brain or neuromuscular impairment and resulting in functional limitations. Although some of these conditions correspond to well-defined diagnostic categories, many overlap or lack clear boundaries, and a substantial number of children experience functional challenges that do not neatly fit any specific diagnostic label. Systems of care that rely on diagnosis-based eligibility for services and funding often fail to meet the needs of children with neurodevelopmental disabilities, as such frameworks prioritize categorical diagnoses rather than the actual support requirements of the child and their family.4,5
Children with Neuro-developmental disorders (NDDs) need growth monitoring, but conventional Diagnosis-Agnostic Protocols and Generic Charts often misclassify risk and miss important problems in this group. Rethinking growth monitoring in this context requires a paradigm shift from narrow Anthropometric surveillance to an Individualized, Function Informed Model that embeds growth assessment within broader developmental, nutritional, and family-centred care. Such a model recognizes that for children with NDDs, meaningful outcomes extend beyond centiles on a chart to include safe feeding, prevention of secondary complications, participation in daily activities, and improved quality of life (QoL).
Ii. Reviewing Neuro Developmental Disorders:
“The Interplay of Biology, Behaviour and Environment”:
Neurodevelopmental disorders (NDDs) comprise a diverse group of conditions that arise from atypical brain development, leading to challenges in cognitive, social, emotional, and behavioural functioning. The most widely recognized NDDs include Autism Spectrum Disorder (ASD) and Attention Deficit Hyperactivity Disorder (ADHD) although many other neurodevelopmental conditions remain comparatively under-recognized and insufficiently studied. These disorders typically emerge during early developmental periods, most often becoming evident in infancy, toddlerhood, childhood, or adolescence. While symptoms persist into adulthood for many individuals, some remain undiagnosed until later life due to subtle manifestations or compensatory mechanisms. In certain cases, children may experience a reduction or resolution of specific symptoms over time, although the underlying neurodevelopmental vulnerability often remains. 6,7
Prevalance Of NDDs: Neurodevelopmental disorders (NDDs) show a clear sex-based disparity, with prevalence consistently higher in males than in females. This difference is thought to arise from a complex interplay of genetic, biological and environmental risk factors. Although conditions such as autism spectrum disorder (ASD) occur more frequently in males, research indicates that the core symptom profiles do not differ substantially between boys and girls.
Genetic susceptibility, Hormonal influences, atypical neurobiological processes (form the underlying predisposition), external risk factors (stress, illness or trauma), Epigenetic mechanisms (environmental influences modify gene expression without altering the DNA sequence), Prenatal factors (maternal infections, psychological stress and nutritional imbalances influencing long-term outcomes in offspring), Perinatal complications (including traumatic or instrumental deliveries like forceps delivery along with maternal dietary patterns), Consanguinity (risk of NDDs by approximately 50% , while males are about 2.2 times more likely to be affected than females – p < 0.05) play a pivotal role triggering or exacerbating these vulnerabilities. Comorbidity is another defining feature of NDDs. Individuals diagnosed with one neurodevelopmental condition are at heightened risk of having an additional NDDs or another mental health disorder.6-10
As per a latest survey by Smith and Doe (2022), the COVID-19 pandemic, caused by the SARS-CoV-2 virus, has profoundly affected populations worldwide where Children have been particularly vulnerable to the consequences of prolonged lockdowns, restricted social interaction and disruptions in routine developmental environments imparting detrimental effects on children with existing developmental challenges, comorbid medical conditions, or mental health disorders. Emerging research indicates that reduced access to educational and therapeutic services, increased screen exposure and social isolation during the pandemic have pivotal roles.11
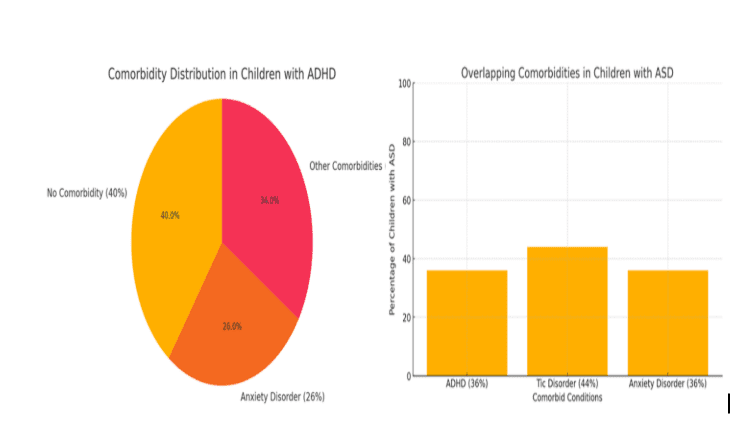
In a study of children aged 7–12 years with mental health conditions by Hansen et al., 55% were found to have at least one neurodevelopmental disorder. Among 181 children with ADHD, nearly 40% had no comorbid conditions, while 26% had an anxiety disorder, and the remainder presented with various other co-occurring conditions.14 Further,the study identified only 18 children with ASD;.Among these participants, 36% had comorbid ADHD, 44% had a Tic disorder (TD), 36% had an Anxiety disorder, and the rest had either other comorbidities or none at all. This pattern highlights the high heterogeneity and overlapping nature of NDDs.12
Major Types Of Ndds And Their Symptoms: Neurodevelopmental disorders (NDDs) encompass a diverse set of conditions characterized by impairments in brain development and neurological functioning. They often lead to challenges in cognition, behaviour, communication, motor skills, learning and adaptive functioning.Below are major types of NDDs and their typical clinical presentations5-12:
| Category | Key Focus | Example Conditions | Common Symptoms/Signs |
| ADHD | Attention, behaviour regulation | ADHD subtypes | Inattention, impulsivity |
| ASD | Social & communication deficits | Autism spectrum | Social difficulty, repetitive behaviour |
| ID | Cognitive & adaptive functioning | ID due to various etiologies | Low IQ, limited independence |
| Communication Disorders | Speech/language difficulties | Stuttering, language disorder | Speech clarity issues, language delay |
| Learning Disorders | Academic skill deficits | Dyslexia, dyscalculia | Reading/math impairment |
| Motor Disorders | Motor coordination & control | DCD, Tourette syndrome | Clumsiness, tics |
| Genetic NDDs | Chromosomal/monogenic | Down syndrome, Fragile X | ID, growth differences |
| Neuromuscular disorders | Motor weakness & delayed development | DMD, congenital muscular dystrophies | Muscle weakness, delayed milestones |
Co-Occurrence Of NDDS: NDDs frequently present together like ASD with ADHD, ASD with ID, ADHD with ID, Hearing loss with vision impairment, requiring comprehensive and multidisciplinary approaches to assessment and intervention tailored to each child’s unique strengths and challenges.5-12
Impact On Family Members Of A Child With NDDs: Evidence consistently shows that parents of children with NDDs experience significantly higher levels of stress compared with parents of typically developing children. This heightened stress can adversely affect the mental health and emotional well-being of caregivers, particularly mothers, and may increase the risk of anxiety, depression and caregiver burden. Furthermore, the challenges associated with providing ongoing care and behavioural management can contribute to Marital strain and Reduced family cohesion.
Consequently, Caregiver support is critical. Parents benefit from access to appropriate resources, respite options, and psychoeducation, as well as the encouragement to engage in self-care strategies that promote stress reduction, positive coping, and sustained mental health.13
Management And Treatment Approaches Of NDDs: Although there is no definitive cure for neurodevelopmental disorders (NDDs), a multidisciplinary approach can significantly improve functioning and quality of life. Management is Individualized and includes behavioural and psychosocial interventions such as cognitive behavioural therapy, speech and language therapy, developmental and social skills training and applied behaviour analysis which target communication, emotional regulation, and adaptive functioning.
Neuromodulation techniques like repetitive transcranial magnetic stimulation are emerging as promising options for selected conditions, though still largely investigational.
Pharmacotherapy is primarily used for symptom control particularly in ADHD with stimulants and non-stimulants and for associated features like anxiety, irritability, or sleep disturbances.
Additionally, lifestyle modifications and complementary approaches, including nutrition, physical activity, mindfulness and yoga may provide supportive benefits but are recommended only as adjuncts to established evidence-based treatments.5-13
III) Growth Monitoring And Promotion (Gmp) With Role Of Growth Charts In Children: A Generalized View
Definition: Growth monitoring is a continuous process of assessing and evaluating a child’s physical growth (primarily Height/Length, Weight and Head Circumference) over time, using standardized growth references in order to promote optimal health. Growth monitoring is a screening tool to diagnose nutritional, chronic systemic and endocrine diseases at an early stage. This ensures early management and optimal outcome.14,15
Key Components / Processes Of GMP: Standard Growth monitoring and promotion (GMP) comprises four sequential steps referred to as ‘The TRIPLE-A (or FOUR-A) cycle’: 1) MEASUREMENT – The regular anthropometric measurements i.e. weight for age, height/length, sometimes head circumference or weight-for-height. 2) ASSESSMENT – Plotting weight against age or weight against height on appropriate growth charts i.e. based on standards like those from World Health Organization (WHO) on a growth chart. 3) ANALYSIS – Interpreting the growth pattern of the child e.g. faltering growth, inadequate weight gain, stunting, wasting. 4) ACTION RELATED TO THE ANALYSIS -Counselling, providing nutritional supplements or examining the child for disease, health education, follow-up, supplementation, disease screening/treatment, referral if needed.13-16
Purpose Of Growth Monitoring Via Growth Charts: Growth charts are essential tools in paediatric practice used to13-16.
- Track a child’s growth trajectory over time
- Compare growth with standardized reference populations.
- Detect early deviations such as growth faltering undernutrition or excessive weight gain.
- Guide nutrition counselling, medical evaluation and intervention decisions.
What Growth Charts Present: Growth charts graphically represent13-16:
- Weight-for-age
- Height/Length-for-age
- Weight-for-height/weight-for-length
- BMI-for-age
- Head circumference-for-age (Infants <2 years)
- These indicators reflect: Nutritional status (Acute and Chronic), Health and Disease risk and Brain, Neurological and Skeletal development.
Reference Standards Used: Different standardized growth charts may be used depending on age and setting16:
| Organization | Age Range | What They Represent |
| WHO Growth Standards | 0–5 years | Optimal growth of breastfed children under ideal environmental conditions |
| WHO Growth References | 5–19 years | International reference of growth patterns |
| CDC Growth Charts | 2–20 years | Growth patterns from U.S. population data |
| National/Regional Charts (e.g., IAP India) | School age children | Adaptation to local population growth trends |
| Condition specific Charts | Genetic disorders | Tailored growth expectations (e.g. Down syndrome) |
Brief Idea About Various Indicators And Their Interpretation In Growth Charts:
- Anthropometric Indicators And Interpretation16
| INDICATOR | DETECTS | EXAMPLES |
| Weight-for-age | Under/overweight trends | Low → Undernutrition |
| Height-for-age | Chronic malnutrition | Low → stunting |
| Weight-for-height | Acute malnutrition | Low → wasting |
| BMI-for-age | Thinness/obesity | > 85th percentile → overweight |
| Head circumference | Brain growth | Micro/macrocephaly |
- Z-Score Cutoffs Used In Growth Monitoring16
| INDICATOR | MODERATE(Z < −2 SD) | SEVERE (Z < −3 SD) | HIGH (Z > +2 SD) |
| Weight-for-age | Underweight | Severe underweight | Risk of overweight |
| Height-for-age | Stunting | Severe stunting | Not typically used for excess |
| Weight-for-height / BMI-for-age | Wasting | Severe wasting | Overweight/Obesity |
| Note– SD= Standard Deviation | |||
IV) Growth Monitoring Gaps In Neurodevelopmental Disorders:
Growth charts and conventional Growth monitoring have important limitations in children with neurodevelopmental disorders (NDDs), leading to frequent misclassification of nutritional status and under-detection of both undernutrition and obesity. These limitations arise from how charts are constructed (reference vs standard), the atypical body composition and growth patterns in NDDs and practical measurement challenges.24,25,30-40.
The various limitations are:
- ‘Reference Populations’ Do Not Represent Ndds Or Disabilities16-18,20:
- Growth charts such as World Health Organization (WHO) or Centres for Disease Control and Prevention (CDC) are derived from healthy, typically developing children.
- In children with neurodevelopmental or neuromotor impairments (e.g., Cerebral Palsy CP), growth trajectories (height, weight, body composition) often differ systematically from the reference population. As a result, using standard charts can lead to misclassification of nutritional status.
- A 1996 study by Stevenson et al. noted that for children with developmental disabilities, “the range of normal growth … remains to be defined.”17
- Implication– Standard percentiles or Z-scores may not reflect ‘normal’ or ‘expected growth’ for a child with an NDD and the comparisons might be biologically inappropriate.
- Growth Charts May Mis-Estimate Nutritional Status-Overestimating Malnutrition In Some As Well As Underestimating In Others16-20:
- A study by Araújo et al. found that when children with CP were assessed on standard (CDC/WHO) growth curves, a large proportion fell below low percentiles (i.e. classified as underweight), but when CP-specific charts were used, fewer were classified as undernourished.19
- This suggests standard charts may overestimate malnutrition (e.g. underweight, wasting) in NDD children.
- Conversely, standard growth charts may fail to detect abnormal body composition (e.g., low muscle mass, fat distribution) or other forms of undernutrition because anthropometry (weight or height) does not capture body composition changes, important in NDDs with altered muscle tone or mobility issues.
- Implication: Nutritional assessment based solely on standard growth curves risks both false positives and false negatives in children with NDDs.
- Difficulty In Accurate Anthropometric Measurement16-20:
- Many children with NDDs have physical disabilities like contractures, joint deformities, scoliosis, inability to stand which make standard height or length measurement unreliable or unfeasible using regular equipment.
- Alternate measurement methods (segmental measures, tibial length, arm span, etc.) are often used; but these require validation and their correspondence with standard growth charts is uncertain.
- Even in NDD-specific growth charts, measurement reliability may vary, especially for children with severe disabilities, limiting their clinical utility.
- Implication: Poor measurement reliability undermines the validity of growth monitoring in NDD children and can lead to misleading growth trajectories.
- Lack Of Unified Condition-Specific Growth Standards & Limited Generalizability16-21:
- Although growth charts have been developed for subpopulations (e.g., children with Down syndrome, CP), these are not universally available or validated across ethnicities, severity levels, or functional categories.
- For children with NDDs in resource-limited or non-Western settings, condition-specific charts may not exist, making growth assessment dependent on ill-fitting standard charts.
- For NDDs with highly heterogeneous phenotypes (e.g., varying motor impairment, feeding ability, comorbidities), even condition-specific charts may not capture individual variability.
- Implication: There is no “One Size Fits All” chart for NDDs, Individual Assessment and Possibly Customized Growth Monitoring strategies are needed.
- Genetic Potential, Rare Genetic Syndromes, Family Background, Ethnic And Regional Variability Not Accounted For16-18,20,22,23:
- Growth potential is highly influenced by genetics, parental height, ethnicity, socioeconomic, environmental and nutritional factors.
- A recent review argues that applying “universal” growth standards can lead to misclassification when genetic and population-specific growth patterns diverge from the reference dataset.
- For certain syndromes (e.g., chromosomal anomalies, metabolic conditions, congenital disorders) specialized growth charts have been developed. Because growth patterns in those conditions diverge significantly from the general population
- Implication: Standard charts ignore individual or family-level variation or Rare Genetic syndromes.
- Weak Evidence Base For Effectiveness Of Growth Monitoring In Ndd Populations16-23:
- Studies on growth monitoring and promotion (GMP) in general populations show mixed evidence regarding impact on long-term nutritional and health outcomes.
- In NDD children, the multifactorial determinants of growth (neurological impairment, feeding issues, metabolic differences) mean that conventional GMP may not effectively prevent malnutrition or monitor real health status.
- Implication: Relying solely on growth monitoring may offer false reassurance or fail to detect clinically significant issues in NDD children. Experts and guidelines for neurologically impaired children recommend this approach.
V)Reconceptualizing Growth Monitoring: The Imperative For An Integrative, Child-Centred Framework In Special Populations:
Given these constraints detailed above, there is a growing consensus that growth monitoring for special populations must evolve into a multidimensional and integrative framework. In 2026, the paradigm for growth monitoring in special populations including children with developmental disabilities or neurodevelopmental disorders is shifting from rigid anthropometric tracking to an integrative, child-centred framework. This reconceptualization addresses the limitations of standard growth charts and emphasizes holistic well-being.
- Components Of The Integrative Framework24-26:
- Individualized Growth Patterns: Standardized reference curves often fail to distinguish between healthy individual variation and actual growth faltering in children with special needs. A child-centred approach prioritizes the child’s own longitudinal trajectory over rigid adherence to population norms.
- Multidimensional Assessment: Modern frameworks integrate physical anthropometry (weight, height, MUAC) with developmental milestones, nutritional quality and psychological development.
- Family-Centred Participatory Support: There is a move away from deficit-based models toward participatory support that empowers caregivers through enhanced communication and shared decision-making.
- IMPERATIVE FOR SPECIAL POPULATIONS24-26:
- Diagnostic Precision: Children with conditions like Down syndrome or autism often exhibit unique, sometimes “erratic” growth patterns that require specialized expertise to interpret correctly without causing unnecessary parental anxiety.
- Addressing Health Inequities: Global reports in 2026 highlight that children with developmental disabilities frequently receive lower-quality care and face systemic barriers to participation; an integrative framework acts as a tool for health equity.
- Early Intervention Entry Points: Growth monitoring and promotion (GMP) platforms are increasingly leveraged as “light-touch” entry points for broader interventions, such as screening for suboptimal development and providing parenting programs.
- IMPLEMENTATION STRATEGIES FOR 202624-26:
- Digital Integration: Utilizing mobile applications that store longitudinal health history, anthropometry and developmental achievements to provide real-time recommendations.
- Specialized Training: Transitioning frontline workers from simple measurement to a “cascade training model” that includes interpreting complex growth data and conducting observation-based assessments.
- Holistic Referral Pathways: Ensuring that deviations in growth trigger immediate access to multidisciplinary teams (nutritionists, therapists and paediatricians) and facilitate access to holistic and integrative modes of care, rather than relying solely on nutritional supplementation or conventional treatment approaches.
VI) HOMOEOPATHIC PERSPECTIVE IN NEURO-DEVELOPMENTAL DISORDERS:
In Homoeopathy, Growth and Development are not merely mechanical outcomes of nutrition or endocrine regulation but they are expressions of the Vital Force, reflecting the dynamic equilibrium between mind, body and inherited predispositions based on the principal based on the principle of ‘Similia Similibus Curentur’.
PHILOSOPHICAL POINT OF VIEW:
- Master Samuel Hahnemann did not explicitly employ the term “Neurological disorders” in the Organon of Medicine or in his other writings. This omission reflects the historical context of the late eighteenth and early nineteenth centuries during which neurology had not yet emerged as a distinct medical specialty. Nevertheless, Hahnemann’s theoretical doctrines, philosophical principles, and numerous clinical observations clearly correspond to conditions that are presently classified as disorders of the brain, spinal cord and peripheral nerves.The Homeopathic approach is to treat the person as a whole, not the disease condition; as quoted by Master C.F Samuel Hahnemann in Organon of Medicine in Aphorism (§) 4 – “He is likewise a preserver of health if he knows the things that derange health and cause disease, and how to remove them from persons in health.”27
- According to Master Samuel Hahnemann, disease and by extension developmental deviation is a disturbance of this vital force, manifesting outwardly through symptoms as mentioned in Organon of medicine (5th and 6th Edition) in the following aphorisms “§7: Totality of symptoms is the outwardly reflected picture of internal essence of disease that is the affection of vital force.” & §11: “When a person falls ill, it is only this spiritual, self-acting (automatic) vital force everywhere present in the organism, that is primarily deranged by the dynamic influence upon it.27
- While discussing Vital Force and Dynamic Diseases (§9, §11, §15, §16), Master Hahnemann explained that all diseases including those affecting the nervous system arising from a dynamic disturbance of the vital force not from structural change alone. This directly includes conditions now called Neurological (e.g., paralysis, convulsions, epilepsy).27
- Master Hahnemann described One-sided diseases in Aphorisms §172–§178 where only few symptoms appear and many neurological diseases (like paralysis, epilepsy, facial palsy) fall in this category. §173 “The only diseases that seem to have but few symptoms, and on that account to be less amenable to cure, are those which may be termed one-sided, because they display only one or two principal symptoms which obscure almost all the others. They belong chiefly to the class of chronic diseases.”27
- Mental and Emotional Diseases (§ 210–§ 230) were considered to arise from or influence nervous system derangement. Master Hahnemann saw the mind and nerves as part of one dynamic system; this anticipates the modern Neuropsychiatric understanding as stated in §215 “Almost all the so-called mental and emotional diseases are nothing more than corporeal diseases in which the symptom of derangement of the mind and disposition peculiar to each of them is increased, while the corporeal symptoms decline (more or less rapidly), till at length attains the most striking one-sidedness, almost as though it were a local disease in the invisible subtle organ of the mind or disposition”.27
- In The Chronic Diseases: Their Peculiar Nature and Their Homoeopathic Cure (1828), Hahnemann described many conditions that today would be labelled as neurological28. Examples:
- Epilepsy, chorea, paralysis, tremors, neuralgias, vertigo, convulsions- all discussed as results of chronic miasmatic affections, especially Psora.
- He linked functional nervous disorders to deep-seated miasmatic causes. “The chronic miasms lie at the root of most nervous affections, when not the result of recent physical injury.’’28
- In Materia Medica Pura, Hahnemann and his provers recorded many neurological symptoms (e.g., tremors, spasms, numbness, paralysis, vertigo) for remedies like29:
| Remedy | Neurological Symptoms (as per Hahnemann) |
| Belladonna | Convulsions, spasms, cerebral congestion |
| Hyoscyamus | Trembling, Twitching, Delirium |
| Nux vomica | Spinal irritation, Paralysis, Convulsive attack |
| Opium | Coma, insensibility, apoplexy- like states. |
| Aconite | Numbness, Neuralgia, Anxiety with restlessness. |
These prove that Master Hahnemann recognized nerve origin symptoms and considered them part of systemic disease processes29.
MIASMATICAL POINT OF VIEW:
- Master Hahnemann states in § 81 regarding Psora that ‘The fact that this extremely ancient infecting agent has gradually passed, in some hundreds of generations, through many millions of human organisms and has thus attained an incredible development, renders it in some measure conceivable how it can now display such innumerable morbid forms in the great family of mankind, particularly when we consider what a number of circumstances one contribute to the production of these great varieties of chronic diseases (secondary symptoms of psora), besides the indescribable diversity of men in respect of their congenital corporeal constitutions……………..’27
- The diagnostic nomenclatures which modern-day psychiatry continues to expand are merely innumerable forms of the fundamental cause. The nomenclature can be necessary when talking about a patient to ordinary persons but totality of symptoms will be the final answer and not disease names. In the 19th century faulty remedies had crippled the soul, mind and body. Unfortunately, in today’s era of suppressions with strong chemicals and with the stigma of vaccination, the disease expression has been similarly forced inward affecting the highest plane of functioning ‘THE MIND’. That’s why the tentacles of Neuro Developmental Disorders gradually go on spreading in every nook and corner of the globe, mainly affecting Paediatric population.
- According to Sigmund Freud, personality develops through a sequence of psychosexual stages during childhood. Each stage is characterized by the focus of libido (psychic energy) on a specific erogenous zone and fixation at any stage may influence adult personality traits.30
| Stage | Age Range | Central Developmental Theme | Healthy Developmental Outcome | Possible Effects of Fixation | Clinical/Behavioral Relevance |
| Oral | Birth–18 months | Dependence on breastfeeding and oral gratification; transition toward autonomy | Basic trust, emotional security, early independence | Dependency, aggression, destructiveness, oral habits | Immaturity, impulsivity, substance-seeking tendencies |
| Anal | 1½–3 years | Sphincter control and toilet training; discipline and authority relations | Orderliness, self-control, responsibility | Rigidity, perfectionism, obstinacy, miserliness | Obsessive traits, control issues, stubborn behaviour |
| Phallic | 3–5 years | Attachment to opposite-sex parent; formation of psychosexual identity; ego–superego development | Gender identity, confidence, emotional balance | Vanity, excessive ambition, restlessness, emotional instability | Attention-seeking, insecurity, unstable self-esteem |
| Latency | 5 years–puberty | Relative quiescence of sexual impulses; focus on learning, peers, and socialization | Social skills, intellectual growth, moral development | Social withdrawal or poor peer integration | Academic or social adjustment difficulties |
| Genital | Puberty–maturity | Emergence of mature sexuality, responsibility, and integrated personality | Emotional maturity, stable relationships, productive adulthood | Immature relationships, emotional conflicts | Relationship instability, maladaptive coping |
- George Loukas in his ‘Unifying Theory of Constitution: Historical Development and Multidisciplinary Correlation’ proposed that Hahnemann’s miasms represent more than simple predispositions to disease and instead correspond to distinct constitutional patterns that integrate psychological development, neurophysiological temperament, and classical medical philosophy.31,32
Loukas therefore framed constitution as a multidimensional unity of miasmatic inheritance, psychological fixation and neurobiological reactivity, offering a philosophical bridge between homoeopathy, psychoanalysis, physiology and ancient medical cosmology while remaining primarily interpretative rather than empirically validated. 31,32
| MIASM | Freudian Correlation | Pavlovian Nervous Type | Hippocratic Humour | Classical Element | Paracelsian Principle | Core Personality Theme |
| PSORA | Repression / general conflict | Vigorous balanced | Blood (Sanguine) | Air | Sulphur | Striving, anxiety, functional disturbance with recovery potential |
| SYCOSIS | Anal fixation | Placid balanced | Phlegm (Phlegmatic) | Water | Salt | Rigidity, retention, control, concealment |
| SYPHILIS | Oral fixation | Weak inhibited | Black bile (Melancholic) | Earth | Mercury | Destruction, despair, withdrawal, degeneration |
| TUBERCULAR | Oedipal fixation | Strong excitable | Yellow bile (Choleric) | Fire | Composite (Psora + Syphilis) | Intensity, dissatisfaction, instability, desire for change |
K.3) REPERTORIAL POINT OF VIEW:
Kent’s Repertory provides a structured and methodical framework for identifying rubrics related to Neurological Developmental Disorders in children. Relevant neurological expressions are distributed across major chapters such as Mind, Head, Vertigo, Back, Extremities and Generalities, reflecting the homoeopathic principle of understanding disease through the totality of symptoms rather than isolated anatomical diagnosis.
The principal sections related to neurological assessment in Kent’s Repertory include33:
- Mind – representing mental and cognitive symptoms
- Head, Vertigo, Face & Mouth – indicating manifestations of the central nervous system
- Back – covering spinal and vertebral disorders
- Extremities – reflecting motor and sensory dysfunctions
- Generalities – expressing systemic neurological manifestations such as weakness or convulsions
1) CHAPTER MIND RUBRICS
- MIND- ABSENT MINDED
- MIND – APHASIA (see Speech, Mistakes, Forgetful)
- MIND- ATTENTION (See Concentration)
- MIND- BITING
- MIND- BUFFOONERY (see FOOLISH Behavior)
- MIND – CAPRICIOUSNESS
- MIND – CHILDISH behavior (see Foolish)
- MIND – CHILDREN
- MIND- CONCENTRATION
- MIND – COMPREHENSION Difficult (See Dullness)
- MIND- CONCENTRATION active
- MIND- CONCENTRATION- difficult
- MIND- CONFUSION of mind (See Concentration)
- MIND- CONCENTRATION- difficult- studying
- MIND- DANCING
- MIND – DELIRIUM
- MIND-DELUSIONS
- MIND-DULLNESS
- MIND- DISOBIDIENCE
- MIND FACES, sees (See Delusions)
- MIND- FOOLISH Behavior (see Childish)
- MIND – GESTURES
- MIND- HASTINESS (See Hurry)
- MIND- HURRY
- MIND – IDIOCY
- MIND -IMPATIENCE
- MIND- IMPETUOUS
- MIND- IMPULSIVE
- MIND- IRRITABILITY (See Anger)
- MIND -JESTING
- MIND- JUMPING
- MIND-KICKS
- MIND- LAUGHING
- MIND- MEMORY- active
- MIND- MEMORY-weakness of
- MIND- MISTAKES in Calculating
- MIND- MISTAKE, words
- MIND- OBSTINATE
- MIND- PLAYFUL
- MIND- RESTLESSNESS
- MIND- RUNS about
- MIND- SHRIEKING
- MIND- SPEECH
- MIND- STUBBORN (See Obstinate)
- MIND- TALKATIVE
- MIND- TEARS things
- MIND – WRITING Aversion to
2) CHAPTER VERTIGO RUBRICS
- VERTIGO – On turning head.
- VERTIGO – Ameliorated by lying down.
3) CHAPTER HEAD RUBRICS
- HEAD – Sensation of emptiness.
- HEAD – Heaviness and pressure in occiput.
- HEAD – Throbbing or bursting sensations.
4) CHAPTER FACE RUBRICS
- FACE- EXPRESSION
- FACE- NUMBNESS
- FACE- PARALYSIS
5) CHAPTER MOUTH RUBRICS
- MOUTH- SALIVATION
- MOUTH- SPEECH- difficult
6) CHAPTER BACK RUBRICS
- BACK – PAIN* – each rubric has some sub rubrics related to (page 894-944)
- BACK – PARALYSIS Of Muscles of Back
- BACK – PARALYSIS sensation of
- BACK – NUMBNESS
7) CHAPTER EXTREMITIES RUBRICS
- EXTREMITIES – CRAMPS.
- EXTREMITIES – CONTRACTION of muscle and elbows
- EXTREMITIES –CONSTRICTION.
- EXTREMITIES –CONVULSION
- EXTREMITIES –FORMICATION.
- EXTREMITIES – NUMBNESS.
- EXTREMITIES – PARALYSIS, upper limbs.
- EXTREMITIES – PARALYSIS, lower limbs.
- EXTREMITIES –SPASM of limbs (see Convulsion)
- EXTREMITIES – TREMBLING.
- EXTREMITIES –TWITCHING.
- EXTREMITIES – WEAKNESS walking.
7) CHAPTER GENERALITIES RUBRICS
- GENERALITIES – Cold in general agg
- GENERALITIES -CONTRADICTORY & ALTERNATING STATES
- GENERALITIES-CONVULSIONS
- GENERALITIES- DISTORTION
- GENERALITIES – DWARFISHNESS
- GENERALITIES-EMACIATION
- GENERALITIES – GRASPING OBJECTS
- GENERALITIES -JERKING
- GENERALITIES – MOTION agg
- GENERALITIES – MOTION amel
- GENERALITIES -NUMBNESS
- GENERALITIES- PERIODICITY
- GENERALITIES-RESTLESSNESS
- GENERALITIES – WARM agg
- GENERALITIES – WARM amel
- GENERALITIES-WEAKNESS, enervation (See Lassitude, Weariness)
Therapeutics Point Of View:
The constitutional remedy, selected through a comprehensive understanding of the patient’s mental, emotional, and physical characteristics, and guided by the principles of ‘Similia similibus curentur” and “Individualization”, functions as the true corrective therapeutic influence in homoeopathic practice.34-37
| MEDICINE | SPHERE OF ACTION | CONSTITUTION | SYMPTOMS |
| AETHUSA CYNAPIUM | Nervous system, Mucous membrane, GIT | Physically the child is very weak; cannot stand; unable to hold up the head. Sunkenness with face with marked linea nasalis. | Idiocy in children; incapacity to think; confused.In epileptic spasm, with clenched thumbs, red face, eyes turned downloads, pupil fixed and dilated, foam at the mouth, jaws locked; pulse small, hard, quick. |
| AGARICUS MUSCARIUS | Nerves, Mind, Brain, Circulation, Skin,Mucous membrane | Person with light hair, skin and muscle lax. | Delirium with constant raving;tries to get out of bed; in typhoid or typhusInvoluntary movements while awake, cease during sleep.Chorea from simple motions and jerks of single muscles to dancing of whole body;trembling of whole body.Every motion, every turn of body causes pain in spine.single vertebra sensitive to touch.Complaints appear diagonally; upper left and lower right side.The provings brings out four phases of cerebral excitement.Slight stimulation–shown by increased cheerfulness, courage, loquacity etc.More decided intoxication– great mental excitement, incoherent talking.Third stage– a condition of furious or raging delirium, screamimg, wants to injure himself.Fourth stage– mental depression, indifference, confusion, disinclination to work. |
| ARTEMISIA VULGARIS | Nervous system mainly | A remedy for epileptic condition and convulsive diseases of childhood and girls at puberty. | Petit mal, epilepsy without aura.Severe convulsions close together.Attacks frequently repeated then followed by a long interval of rest.Somnambulism. Gets ups at night and works, remembers nothing in the morning. |
| BARYTA CARBONICA | Affects Nutrition, Glands, Throat,Prostrate, Blood vessels, Nerves. | Scrofulous, dwarfish children who do not grow; abdomen swollen; frequent attacks of colic; face bloated; general emaciation. | Especially adapted to complaints of first and second childhood, psoric or tubercular.Children both mentally and physically weak.Memory deficient, forgetful, inattentive; child cannot be taught for it cannot remember; threatened idiocy.Very averse to meet strangers.Child does not want to play, but sits in a corner doing nothing or throwing stones at strangers. |
| CALCAREA CARBONICA | Acts on Bones, Glands, Skin, Mind. | Suited to Fair, fatty, flabby children red face, flabby muscle, who sweat easily and take cold readily in consequence. | Large head and abdomens; fontanelles and sutures open; bones soft, develop very slowly.Curvature of bones, especially spine and long bones; extremities crooked, deformed; bones irregularly developed.Diseases: arising from defective assimilation; imperfect ossification; difficulty in learning to walk or stand; children have no disposition to walk and will not try.During either sickness or convalescence, great longing for eggs; craves indigestible things; aversion to meat, Longing for fresh airDesire to be magnetised.All discharges sour. |
| CALCAREA PHOSPHORICA | Glands,Digestive systemFemale Genital organs | During first and second dentition of scrofulous children; diarrhoea and great flatulence.For persons anaemic and dark complexioned, dark hair and eyes; thin spare subjects, instead of fat. | Children emaciated, unable to stand; slow in learning to walk; sunken flabby abdomen.Rachitis, cranial bones thin and brittle; fontanelles and sutures remain open too long, or close and re-open; delayed or complicated teething.Spine weak, disposed to curvatures, especially to the left; unable to support the body; neck weak, unable to support head.At every attempt to eat, colic pain in abdomen. |
| CICUTA VIROSA | Cerebro Spinal Nervous system mainly | Subject to epileptic and choreic convulsion; spasm of teething children, or from worms. | When reading, the letters seem to turn, go up or down or disappear.Convulsions, violent, with frightful distortions of limbs and whole body; with loss of consciousness of opisthotonous; renewed from slightest touch, noise or jar.Epilepsy with swelling of the stomach as from violent spasm of the diaphragm, lock-jaw, loss of consciousness and distortion of limbs, frequent during the night; recurring, first at short, then at long interval. |
| CUPRUM METALLICUM | Alimentary canal, Nervous systems and various Nerve centres | Suited to fair haired people and carbo-nitrogenoid constitution. | Spasm and cramps: symptoms disposed to appear periodically and in groups.Constant protrusion and retraction of the tongue, like a snake.Convulsion with blue face and clenched thumbs.Epilepsy: aura begins in the knee and ascends < at night during sleep; about new moon, at regular interval. |
| HELLEBOROUS NIGER | Brain, Nervous system,meninges, Kidney, GI tract | Weakly, delicate, psoric children; prone to brain troubles; with serous effusion | Brain symptoms during dentition; threatening effusion.Unconscious; stupid; answers slowly when questioned; a picture of acute idiocy (chronic idiocy- Baryta carb)Automatic motion of one arm and leg.Meningitis; acute, Cerebro-spinal, tubercular with exudation; paralysis more or less complete; with the CRI ENCEPHALIQUE.Soporous sleep with screams, shrieks, starts. |
| HYOSCYAMUS NIGER | Nervous system,Sensorium, Muscle system | Persons of sanguine temperament; who are irritable, nervous, hysterical | Convulsion- of children, child vomits, sudden shriek, then insensible.Spasms: without consciousness, very restless; every muscle in the body twitches, from the eyes to the toes.Diseases with increased cerebral activity, but non-inflammatory in type; hysteria or delirium tremens.Delirium with restlessness, jumps out of bed, tries to escape; makes irrelevant answers; thinks he is in wrong place; talks of imaginary doings, but has no wants and makes no complaints. |
| KALIUM BROMATUM | Mind,Cerebro-spinal Nervous system,Skin | Adapted to persons inclined to obesity; to children. | Inco-ordination of muscles; nervous weakness or paralysis of motion and numbness.Night terrors of children; grinding teeth in sleep, screams, moans, cries; horrible dreams, cannot be comforted by friends. Somnambulism.Stammering; slow, difficult speech.Epilepsy: congenital, syphilitic, tubercular; headache follows attack. |
| TARENTULA HISPANIA | Nervous system specially termini of nerves, Genito-urinary system | Restlessness, could not keep quiet in any position, must keep in motion, though walking <all symptomsHyperaesthesia aggravated by touch of affected parts but relieved by rubbing the affected parts.Very sensitive to music. It relieves nearly all symptoms but sometimes it excites violently. | |
| LATHYRUS SATIVUS | Mainly on the Nervous system | Affects the lateral and anterior columns of the cord. Does not produce painReflexes always increased.Paralytic affections of lower extremities; spastic paralysis; lateral sclerosis.Excessive rigidity of legs; spastic gait.Knees knock against each other when walking.Myelitis with marked spastic symptoms.Muscle of calves very tense.Patient sits bent forward, straightens with difficulty. | |
| PLUMBUM METALLICUM | The point of action are the Neuro-axons and the Anterior horns. | Excessive and rapid emaciation with extreme weakness and anaemia. | Adapted to diseases from spinal origin.General or partial paralysis;Slow of perception; intellectual torpor, gradually increasing apathy.Progressive muscular atrophy. Infantile paralysis. Locomotor ataxia. |
| ZINCUM METALLICUM | Cerebro-spinal system, Blood, Digestive system, Kidney | Persons suffering from cerebral and nervous exhaustion; defective vitality; brain or nerve power wanting. | Incessant and violent fidgety feeling in feet or lower extremities; must move them constantly.Child repeats everything said to it.Child cries out during sleep; whole body jerks during sleep; wakes frightened, starts, rolls the head from side to side; face alternately pale and red.Automatic motion of hands and head, or one hand and head.Convulsion: during dentition, with pale face, no heat, except perhaps in occiput, no increase in temperature; rolling the eyes; gnashing the teeth.Spinal affections: burning whole length of spine; Cannot bear back touched. |
VII) Acknowledgement: The authors would like to acknowledge Prof (Dr.) Kaushik D Das, Principal in Charge, The Calcutta Homoeopathic Medical college and Hospital, Kolkata for his constant guidance and encouragement for writing this article.
Viii) Conflict Of Interest & Financial Support: Nil.
IX) References:
- Leroy JL, Brander RL, Frongillo EA, Larson LM, Ruel MT, Avula R. Perspective: Can Growth Monitoring and Promotion Accurately Diagnose or Screen for Inadequate Growth of Individual Children? A Critical Review of the Epidemiologic Foundations. Adv Nutr. 2025 Mar;16(3):100367. doi: 10.1016/j.advnut.2025.100367. Epub 2025 Jan 11. PMID: 39805485; PMCID: PMC11880696.
- Scherdel P, Dunkel L, van Dommelen P, Goulet O, Salaün J-F, Brauner R, Heude B, Chalumeau M. Growth monitoring as an early detection tool: a systematic review. Lancet Diabetes Endocrinol. [Internet] 2016;4:447–456. doi: 10.1016/S2213-8587(15)00392-7. http://www.ncbi.nlm.nih.gov/pubmed/26777129
- Roberfroid D, Kolsteren P, Hoerée T, Maire B. Do growth monitoring and promotion programs answer the performance criteria of a screening program? A critical analysis based on a systematic review. Trop. Med. Int. Health [Internet] 2005;10:1121–1133. doi:10.1111/j.13653156.2005.01498.x. http://www.ncbi.nlm.nih.gov/pubmed/16262737
- Ip A, Poon BT, Oberlander TF. Rethinking diagnosis-based service models for childhood neurodevelopmental disabilities in Canada: a question of equity. Paediatr Child Health. 2023 Mar 29;28(8):480-482. doi: 10.1093/pch/pxac131. PMID: 38638540; PMCID: PMC11022863.
- Zamora-Moratalla A, Martínez de Lagrán M, Dierssen M. Neurodevelopmental disorders: 2021 update. Free Neuropathol. 2021 Mar 24;2:6. doi: 10.17879/freeneuropathology-2021-3268. PMID: 37284629; PMCID: PMC10209888.
- Verywell Mind. Understanding neurodevelopmental disorders [Internet]. 2022 Mar 31 [cited 2025 Dec 03]. Available from: https://www.verywellmind.com/neurodevelopmental-disorders-definition-symptoms-traits-causes-treatment-5221231
- American Psychiatric Association. Neurodevelopmental Disorders [Internet]. Arlington (VA): American Psychiatric Association; [cited 2025 Dec 08]. Available from: https://www.psychiatry.org/patients-families/neurodevelopment-disorders
- May T, Adesina I, McGillivray J, Rinehart NJ. Sex differences in neurodevelopmental disorders. Curr Opin Neurol. 2019;32(4):622-626. doi:10.1097/WCO.0000000000000714
- Bale TL, Baram TZ, Brown AS, Goldstein JM, Insel TR, McCarthy MM, Nemeroff CB, Reyes TM, Simerly RB, Susser ES, Nestler EJ. Early life programming and neurodevelopmental disorders. Biol Psychiatry. 2010 Aug 15;68(4):314-9. doi: 10.1016/j.biopsych.2010.05.028. PMID: 20674602; PMCID: PMC3168778.
- Bahal M, Pande V, Salunkhe S, Dua J, Mane S, Gupta A, Kumar G, Kale S, Garlapati S, Shaligram R. Clinical Profile of Neurodevelopmental Disorders in Children at a Tertiary Care Center. Cureus. 2024 Aug 26;16(8):e67819. doi: 10.7759/cureus.67819. PMID: 39323725; PMCID: PMC11423788.
- Smith J, Doe A. The impact of COVID-19 pandemic on screen time and its effects on neurodevelopmental disorders in children. J Child Psychol Psychiatry. 2022;62:523-534.
- Hansen BH, Oerbeck B, Skirbekk B, Petrovski BÉ, Kristensen H. Neurodevelopmental disorders: prevalence and comorbidity in children referred to mental health services. Nord J Psychiatry. 2018 May;72(4):285-291. doi: 10.1080/08039488.2018.1444087. Epub 2018 Feb 28. PMID: 29488416.
- Dykens EM. Family adjustment and interventions in neurodevelopmental disorders. Curr Opin Psychiatry. 2015;28(2):121-126. doi:10.1097/YCO.0000000000000129
- Paul VK, Bagga A, editors. GHAI Essential Pediatrics. 10th ed. New Delhi: CBS Publishers & Distributors; 2023.
- Gupte S. The Short Textbook of Pediatrics. 13th ed. New Delhi: Jaypee Brothers & Co (P) Ltd; 2020.
- World Health Organization. WHO Child Growth Standards [Internet]. Available from: https://www.who.int/tools/child-growth-standards/standards
- AbilityPath. Growth and Growth Charts for Children with Special Health Care Needs [Internet]. Redwood City (CA): AbilityPath; [cited 2025 Dec 09]. Available from: https://abilitypath.org/ap-resources/growth-and-growth-charts-for-children-with-special-health-care-needs/
- Stevenson RD. Measurement of growth in children with developmental disabilities. Dev Med Child Neurol. 1996 Sep;38(9):855-60. doi: 10.1111/j.1469-8749.1996.tb15121.x. PMID: 8810718.
- Araújo LA, et al. Anthropometric assessment of patients with cerebral palsy: comparison of reference curves and implications for nutritional classification. Clin Nutr. 2013;32(5):965–71.
- Choudhary, G., Inamdar, N. R., & Mauskar, A. (2022). Cerebral palsy specific growth charts for Indian children: need of the hour. International Journal of Contemporary Pediatrics, 9(7), 663–667. https://doi.org/10.18203/2349-3291.ijcp20221610
- Khatun R, Bin Siddique MK, Khatun MR, Benzir M, Islam MR, Ahmed S, Muurlink O. Nutritional status of children with neurodevelopmental disorders: a cross-sectional study at a tertiary-level hospital in northern Bangladesh. BMC Nutr. 2024 Apr 19;10(1):61. doi: 10.1186/s40795-024-00863-9. PMID: 38641622; PMCID: PMC11027387.
- ESPGHAN (European Society for Paediatric Gastroenterology, Hepatology, and Nutrition). Recommendations for Nutritional Management of Children with Neurological Impairment (NI). 2019.
- World Health Organization. International classification of functioning, disability and health (ICF). Geneva: WHO; 2001
- World Health Organization. Monitoring children’s development in primary care services: Moving from a focus on child deficits to family-centred participatory support. Report of a virtual meeting 9–10 June 2020. Geneva: WHO; 2020. ISBN: 9789240012479.
- The DHS Program. Guide to DHS Statistics: Child Growth Monitoring. DHS Program. Available from: https://dhsprogram.com/Data/Guide-to-DHS-Statistics/Child_Growth_Monitoring.htm.
- Pelto GH, Dickin KL, Engle PL; World Health Organization. A critical link: Interventions for physical growth and psychological development: a review. Geneva: World Health Organization; 1999. WHO reference number WHO/CHS/CAH/99.3. Available from: https://www.who.int/publications/i/item/a-critical-link-interventions-for-physical-growth-and-psychological-development.
- Hahnemann S. Organon of Medicine. 6th ed. Translated by Boericke W. New Delhi: B. Jain Publishers; 2002.
- Hahnemann S. The chronic diseases: their peculiar nature and their homoeopathic cure. 2nd ed. New Delhi: B. Jain Publishers (P) Ltd.; 1995. (Originally published 1828).
- Hahnemann S. Materia medica pura. 6th ed. New Delhi: B. Jain Publishers (P) Ltd.; 1994. (Originally published 1811–1821)
- Freud S. The standard edition of the complete psychological works of Sigmund Freud. Vol. 7. Strachey J, editor. London: Hogarth Press; 1953.
- Loukas G. A unifying theory of constitution. Homoeopathic Links. 2012;25(4):241-243. doi:10.1055/s-0032-1327824.
- Lukas G. Roots: the unifying theory of constitution. Athens: I. Archangelos; 1999. Available from: https://www.modernhomoeopathy.com/constitution%20george.htm
- Kent JT. Repertory of the homoeopathic materia medica. 6th American ed. New Delhi: B. Jain Publishers (P) Ltd.; 1993.
- Lilienthal S. Homoeopathic Therapeutics. 3rd ed. New Delhi: B. Jain Publishers; 2002.
- Boericke W. Pocket manual of homoeopathic materia medica and repertory. 9th ed. New Delhi: B. Jain Publishers; 2002.Kent JT. Repertory of the homoeopathic materia medica. 6th ed. New Delhi: B. Jain Publishers; 2004.
- Allen HC. Keynotes and characteristics with comparisons. 10th ed. New Delhi: B. Jain Publishers; 2002.
- Dubey SK. Text book of materia medica including Allen’s keynote: new inclusion Indian drugs & biochemic system of medicine. 6th ed. Kolkata: Books & Allied (P) Ltd; 2021.
Authors
- Dr. ANJAN ROY; Ph.D. (HOM.), M.D (HOM.)
Associate professor & HOD, Department of Surgery, I.C, Department of Paediatrics,
The Calcutta Homoeopathic Medical College & Hospital, Kolkata. - Dr. SOUMYANATH MALLIK; B.H.M.S (WBUHS)
Post Graduate Trainee, Department of Paediatrics, The Calcutta Homoeopathic Medical
College and Hospital, Kolkata-700009.
Ex-Internee, National Institute of Homoeopathy, Salt Lake, Kolkata-700106. - Dr. RUPALI BHADURI; Ph.D. (HOM.), M.D (HOM.)
Associate professor & HOD, Department of Practice of Medicine, The Calcutta
Homoeopathic Medical College and Hospital, Kolkata - Dr. ISHIKA MANI; B.H.M.S (WBUHS)
Post Graduate Trainee, Department of Materia Medica, The Calcutta Homoeopathic
Medical College and Hospital, Kolkata.