Abstract:
Background: Psychogenic pruritus is characterized by itching with a psychological rather than dermatological origin, often manifesting as a somatic expression of anxiety disorders. This case report examines the effectiveness of an integrative treatment approach—combining individualized homeopathy with Cognitive Behavioral Therapy (CBT)—in a rare case of chronic
palmar itching induced by social anxiety.
Case Presentation: A 24-year-old female presented with a 1.5-year history of severe itching localized to her palms, aggravated by social interactions and crowded environments. Notably, there were no primary dermatological lesions, persistent scratching leading to skin soreness. The Liebowitz Social Anxiety Scale (LSAS-SR) indicated significant social anxiety (Total Score: 76).
Management: The patient received a single dose of the homeopathic remedy Silicea 200C, based on her constitutional picture highlighting nervous hypersensitivity. This was complemented by CBT, focusing on cognitive restructuring of her fears and habit reversal training to address the itch-scratch cycle.
Results: Within ten days, the patient reported reduced itching intensity and improved emotional regulation, with a decrease in LSAS-SR score from 76 to 70. Although the WHO-5 Well-being Index initially declined, this was interpreted as an emotional “unmasking” phase typical of early stage therapy.
Conclusion: The integrative approach combining Silicea and CBT effectively addressed both the underlying miasmatic susceptibility and the behavioral symptoms of social anxiety in this patient.
Keywords: Social Anxiety Disorder; Psychogenic Pruritus; Homeopathy; Silicea; Integrative Medicine; Case Report.
Introduction: Social Anxiety Disorder (SAD), or social phobia, is a debilitating mental health condition marked by a fear of being watched and judged in social situations, leading to great psychological distress that drives individuals to avoid social interactions.
Unlike mere shyness, individuals with SAD experience profound psychological distress, leading to avoidance behaviors and heightened autonomic nervous system arousal. This intense fear can trigger the “fight-or-flight” response, manifesting physically as sensations in the skin, particularly when the individual feels emotionally “invaded.” In some cases, this intense anxiety can manifest physically as Psychogenic Pruritus, a condition characterized by chronic itching without an underlying dermatological cause or underlying skin pathology. The itching episodes are typically paroxysmal, occurring suddenly and intensely during emotional stress or anxiety. The resultant skin damage, such as redness and soreness, is primarily due to the patient’s own scratching rather than an underlying rash or infection.
The Brain-Skin Axis:
The brain-skin axis represents a profound bidirectional communication network linking the central nervous system (CNS) with the integumentary system, specifically the skin. This connection has its origins in embryological development, as both the brain and skin arise from he ectoderm, establishing a deep-rooted relationship that persists throughout life. As individuals navigate emotional landscapes, such as those experienced in social anxiety, the brain’s hypothalamus becomes activated, triggering the Hypothalamic-Pituitary-Adrenal (HPA) axis. This activation leads to the release of stress hormones, primarily cortisol, and
neuropeptides like Substance P, which circulate through the body and reach the skin. Upon arrival in the dermal layers, these chemical messengers engage mast cells, specialized immune cells that play a pivotal role in inflammatory responses. The activation of mast cells results in the release of histamine and other inflammatory markers, which irritate nerve endings within the skin. This process can produce sensations such as itching, even in the absence of external allergens or irritants. Thus, the brain-skin axis illustrates how emotional stress can manifest as tangible skin sensations, underscoring the intricate interplay between our mental and physical well-being.
The Psychosomatic Mechanism
Our hands facilitate greetings, touch, and connection; however, for someone like Manju, who perceives the act of a handshake —social encounters as encroachment upon her personal space, her brain interprets this as a threat, sending urgent signals to the nerves in her palms. This response manifests as an “anxiety-itch,” a somatic expression of her distress. Thus, the connection between social fears and palmar itching becomes strikingly evident, illustrating the profound interplay between mind and body. Here an unexpected proximity or a probing question leads to emotional turmoil—anxiety entwined with suppressed anger. This internal heat prompts the release of neuropeptides in the skin, intensifying the sensation of itching, in a bid for relief, Manju ends up in scratching, which provides only a fleeting distraction from her social anxiety temporarily masks the mental anguish of anxiety which often resulting in physical pain and redness.
This interplay between psychological distress and physical symptoms underscores the complex relationship between mind and body in mental health disorders, emphasising the need for comprehensive integrated treatment approaches that address both psychological and physical aspects.
Case History
Chief Complaints: A 24-year-old Hindu female homemaker from Bhopal presented with a 1.5-year history of persistent, localized pruritus of the palms. The intense, paroxysmal itching, primarily triggered by social interactions and crowded environments, has led to a compulsive urge to scratch, resulting in redness and soreness, despite the absence of primary dermatological lesions.
History of Present Illness
Her psychological symptoms began at age 16, with a gradual onset of social anxiety gettingprogressively worst. The somatic manifestation of palmar pruritus emerged alongside increased social stress, with symptoms worsening during the evening and night, significantly impacting her daily life and interactions.
Aggravating factors include:
● Physical contact (e.g., shaking hands).
● Over crowed places.
● social gatherings, even social interactions
Ameliorating factors include:
● Social withdrawal and isolation.
● Cognitive distraction.
● Local application of cool substances.
Past medical history : conventional treatment provided symptomatic relief, leading the patient to seek an integrated therapeutic approach.
Medical and Personal History
The patient has a significant pediatric history of typhoid at age 12.
Family history is notable for maternal depression.
Personal history reveals a nervous, chilly temperament (thermally sensitive to cold) with a “psoro-sycotic” miasmatic background.
Psychologically, she exhibits internalized anger, high irritability, and a profound sense of being “invaded” or misunderstood during social discourse.
Physical and Clinical Findings
On examination, the patient appeared tense and anxious, demonstrating frequent scratching of
the palms and hesitant speech patterns.
● Skin: Generalized dryness; palms showed redness , no vesicles, papules, or burrows were found
● Vitals: Stable (BP 110/70 mmHg, Pulse 76 bpm).
● Systemic Examination: No abnormalities detected (NAD).
● Laboratory Investigations: CBC within normal limits. Further investigations (LFT, KFT, HbA1c) were advised to rule out metabolic causes of pruritus. But patient didn’t take these tests.
Diagnostic Reasoning
Based on the DSM-5 criteria, a provisional diagnosis of Social Anxiety Disorder (SAD) with associated Psychogenic Pruritus was established. The absence of dermatological symptoms / infestation and the direct correlation between social stressors and itching episodes support the psychosomatic nature of the condition.
Methodology
This study explains a single-case, integrated therapeutic design combining Individualized Homeopathy with Cognitive Behavioral Therapy (CBT). The objective was to address the patient’s condition at both the constitutional (miasmatic) and behavioral levels.
The homeopathic treatment followed the principles of classical homeopathy, Constitutional Approach) focusing on the “totality of symptoms.”
Repertorization: Symptoms were analyzed using a standardized repertory.
A structured Cognitive Behavioral Therapy (CBT) program was started along with homeopathic medicine. It includes changing negative thoughts about social situations, gradually facing social fears, managing compulsive scratching with alternative techniques, and practicing deep breathing to reduce stress that leads to skin itching.
Prescribing totality
● Itching mainly on palms, scratch until skin becomes red and sore.
● no visible skin lesion.
● Itching becomes worse after shaking hands or in crowded places.
● Intense discomfort with physical proximity-feels invaded if someone comes too close or touches her.
● itching worsens during or after social contact. Symptoms worsen in the evening.
● Dry, rough texture localized to the palmar surfaces.
● oversensitive
Repertorial Totality
The following rubrics were selected for repertorization to capture the psychosomatic nature of
the case:
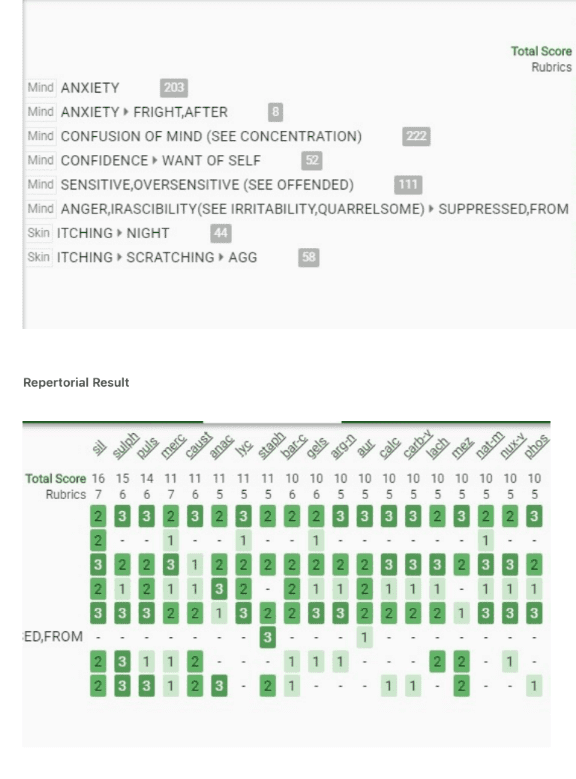
Clinical Reasoning for Remedy Selection
Silicea had highest repertorial score and deep constitutional affinity. The patient’s chilly disposition, dry skin, and the worsening of symptoms in the evening/night are hallmark indicators for Silicea.
Analytical study of Silicea based on specific modality of “better by cool application on palms” (often seen as a local relief for Silicea’s nervous heat) where paradoxically, patient being easily chilled, highly chilly patient.
Suppressed Anger: While Staphysagria is often considered for suppressed anger, hereSilicea covered the “nervous disposition” and the specific modality of “better by cool application on palms” (often seen as a local relief for Silicea’s nervous heat).
Silica is sensitive both physically and emotionally (“the senses are morbidly keen”: Farrington).
In his lecture on Silicea, E.A. Farrington: in Clinical Materia Medica describes the “erethism” of the nervous system, explains that Silicea patients feel cold but can suddenly experience hot sensations in their limbs due to an overactive nervous system. He relates this to the “scrofulous and nervous” constitution.
Catherine R coulter in her book Portraits of Homoeopathic medicines, vol II psychophysical analysis of selected constitutional Types. States – Silica often gets worried of the unknown and the world and leading to a dull and repetitive routine. But paradoxically, despite being easily chilled, the silicea patient likes the feel of cool air or cold water (Hepar Sulphuris, Tuberculinum) and is aggravated by heat.
Want of “grit” moral or physical , is a leading indication of silicea in Homoeopathic practice.
J.H. Clarke: A Dictionary of Practical Materia Medica
Coulter’s psychological analysis of Silicea is perhaps the most famous modern reference for the remedy’s lack of “grit.” Portraits of homoeopathic medicines:
In Volume II, under the chapter for Silica, Coulter explores the “want of grit” both physically (the limp spine, weak connective tissue) and morally (the shy, yielding, but secretly stubborn nature).
Prescription
● Remedy: Silicea 200 ● Dosage: Single Dose (S.D.) – 4 pills
● Follow-up Plan: Evaluation after 10 days to assess changes in the LSAS-SR score and the intensity of the palmar pruritus.
Assessment and Monitoring
To ensure objective measurement of progress, the following validated tools were utilized at
baseline and follow-up:
● Liebowitz Social Anxiety Scale (LSAS-SR): To analyse the changes in anxiety and avoidance behaviors.
● WHO-5 Well-being Index: To monitor the patient’s subjective quality of life and emotional health.
● Clinical Observation: Physical examination of the palms during each follow-up to monitor for reduction in secondary skin changes.
Results
Discussion
The Role of Integrated Therapy
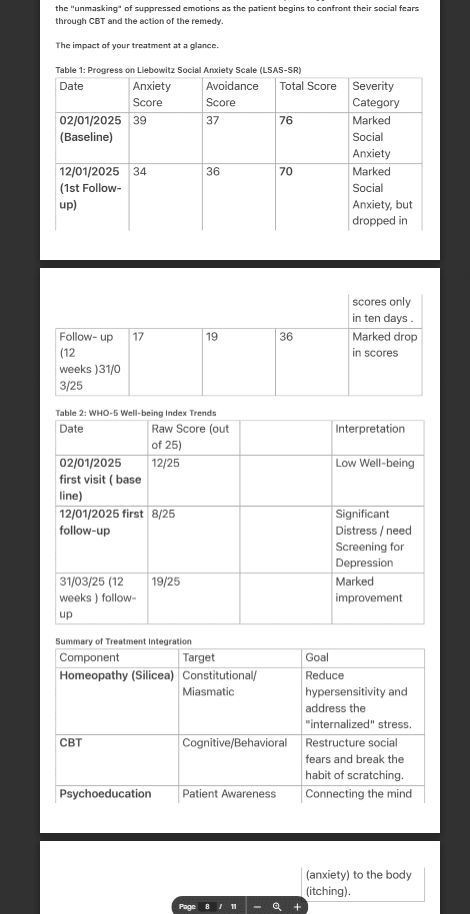
The integration of Cognitive Behavioral Therapy (CBT) alongside the homeopathic prescription was vital. The use of the Liebowitz Social Anxiety Scale (LSAS-SR) helps us to gauge the severity of her avoidance and anxiety. The baseline score (76 total) indicated “marked social anxiety,” which showed a downward trend (70 total) within the first 10 days.
The decline in the WHO-5 Well-being Index from 12/25 to 8/25 during the first follow-up is a critical observation. this case doesn’t represents a “homeopathic aggravation” . It could be the “unmasking” of suppressed emotions as the patient begins to confront their social fears through CBT and the action of the remedy.
The impact of your treatment at a glance.
Miasmatic Analysis
In Homeopathy, the miasmatic diagnosis explains the depth and progression of the pathology. In this case, the diagnosis is Psoro-sycotic.
● Psoric Component: the primary symptom of functional itching and the high degree of nervous sensitivity. Psora represents the “struggle” and the physiological sensitization to social environments.
● Sycotic Component: Reflected in the fixed ideas (the feeling of being “invaded”), the progressive worsening over years, and the internalized, suppressed anger. Sycosis represents the “defense” and the structural buildup of anxiety that has become a part of her personality.
The 10-day follow-up showing a dip in well-being (WHO-5). Why ?
Note: The 10-day follow-up showing a dip in well-being (WHO-5) suggests the remedy is pushing the “suppressed” sycotic anxiety back into the psoric (functional/expressive) plane, which is a positive sign of healing according to Hering’s Law of Cure? More in-depth research is needed to better understand and explain these responses, allowing for clearer insights and interpretations of the findings.
My question was. “ Why the Palms?”
The palms are full of nerve endings and are thought of as our main way to connect with others. For someone with social anxiety, the conflict between the need to interact and the fear of interaction manifests in the palms as a “nervous itch.”
We asked her: “How did you feel about the connection between your social fears and the itchingon your palms?” In first visit she didn’t realise there was any connection. But when we asked her same question in her first follow-up . She expressed…
Drafting the Patient Perspective:
“For more than a year, it felt like my skin was reacting to people before I even said a word. Shaking hands felt uncomfortable, and the intense itching in my palms consumed my thoughts in crowded places. Till today I believed it was just a skin issue, but now talking about my problem , I discovered that my palms were ‘screaming’ because of my deep anxiety. After starting
medication and talking through my feelings, the urge to scratch has lessened. Now, I feel little ease and in control , allowing me to connect with others, discomfort also has lessened “.
Generally follow-ups are scheduled every weekly, fortnightly or monthly, whereas comparative assessments are scheduled at 4-week intervals to 6-month period to ensure the stability of the clinical response.
But in this study , we have taken the first follow-up on tenth day for comparative assessments because of following reasons :
●The first follow-up was conducted at 10 days to capture the acute phase of the brain-skin response . This interval is consistent with clinical standards for evaluating the initial response to high-potency (200C) remedies in hypersensitive patients Vermeulen, 1997).”
● In psychodermatological cases, the sensory nerve endings in the skin often respond rapidly to shifts in autonomic nervous system arousal. A 10-day interval was used for the assessment of whether the combined approach of Silicea 200 and CBT-based relaxation had an immediate impact on the patient’s “itch threshold” during social triggers.
● The 10-day interval was strategically chosen to-observe the Primary Action (Hahnemann, 842/1996). The observed dip in the WHO-5 Well-being score (from 12 to 8) at this stage serves as objective evidence of this internal shift.
● Since the patient was instructed to use Habit Reversal Training and Mindfulness, a 10 day check-up was necessary to ensure she was applying these techniques correctly before maladaptive scratching patterns could reinforce themselves further.
●With patient’s “psoro-sycotic” nature and high sensitivity, early monitoring was essential to check the intensity of the “raw skin” (secondary to scratching) was decreasing.
Conclusion
This case study highlights the effectiveness of a combined therapy approach in treating complex skin conditions linked to emotional issues. The patient’s chronic itching in her palms was not just a skin problem; it stemmed from deep social anxiety and feelings of personal violation. The reduction in her anxiety score over ten days shows that the homeopathic remedy Silicea 200 helped her emotional sensitivity, while Cognitive Behavioral Therapy enabled her to manage her itch-scratch habit. Initial feelings of decreased well-being remind us that addressing hidden emotions is crucial for true healing. This case encourages more research into combining homeopathy and CBT for better treatment outcomes.
Key Takeaways for Clinicians
● Social Anxiety Disorder (SAD) manifesting as Psychogenic Palmar Pruritus.
● The “Brain-Skin Axis,” where social stress triggers neurogenic itching via the HPA axis.
● Suppressed Anger: While Staphysagria is often considered for suppressed anger, but in this case Silicea covered the “nervous disposition” and the specific modality of “better by cool application on palms” (often seen as a local relief for Silicea’s nervous heat). Coulter’s psychological analysis of Silicea
● CBT Integration: Habit reversal training and cognitive restructuring are essential to break
the chronic itch-scratch cycle.
● The first follow-up was conducted at 10 days interval to capture the acute phase of the brain-skin response and was used to compare with base line scores .
● Using scales like LSAS-SR and WHO-5 are important for proving clinical efficacy.
● Catherine R coulter in her book Portraits of Homoeopathic medicines, vol II psychophysical analysis of selected constitutional Types. Explains why the silicea patient likes the feel of cool air or cold water (Hepar Sulphuris, Tuberculinum) and is aggravated by heat. where paradoxically, patient being easily chilled, highly chilly patient.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
https://doi.org/10.1176/appi.books.9780890425596
Hahnemann, S. (1996). Organon of the medical art (W. B. O’Reilly, Ed.; 6th ed.). Birdcage Books.
(Original work published 1842)
Vermeulen, F. (1997). Concordant materia medica. Emryss Publishers.
Yosipovitch, G., & Samuel, L. S. (2008). Neuropathic and psychogenic itch. Dermatology Therapy, 21(1), 32–41.
https://doi.org/10.1111/j.1529-8019.2008.00167.x
Boericke, W. (1927). Pocket manual of homoeopathic materia medica (9th ed.). Boericke & Runyon. (Original work published 1901).
Clarke, J. H. (1902). A dictionary of practical materia medica (Vol. 3). The Homoeopathic Publishing Company.
Coulter, C. R. (1986). Portraits of homoeopathic medicines: Psychophysical analyses of selected constitutional types(Vol. 2). Ninth House Publishing.
Farrington, E. A. (1887). A clinical materia medica: Being a course of lectures delivered at the Hahnemann Medical College of Philadelphia (C. Bartlett, Ed.). Sherman & Co.
Kent, J. T. (1905). Lectures on homoeopathic materia medica. Boericke & Tafel.
Co-Author:
Dr. Bhupinder Singh
Prof. & Head Dept. of Psychology Barkatullah University. Bhopal