Abstract
Hahnemann spent 12 years of intensive study relating to the presence of miasms to chronic diseases. Dr Hahnemann after years of practice reached to the conclusion that all chronic diseases were the result of the chronic miasms.
The consideration of miasms is of paramount importance in effective homoeopathic prescribing particularly in this world of multi-suppressions, where perceiving a clear picture of the disease is becoming increasingly difficult.
Psora is the mother of all miasm and is alone responsible for most of the chronic diseases of mankind and manifests itself in varying forms. Dr Kent says, “Psora is the beginning of all physical sickness. Had Psora never been established as a miasm upon the human race, the other two chronic diseases would have been impossible.”
The following case of a 57-year-old lady suffering from chronic plaque psoriasis or psoriasis vulgaris for 25 years. Lesions were widespread on the whole body chiefly on both limbs and trunk. She was treated very effectively with antipsoric medicine sulphur after thorough case taking.
Keywords: Miasm, Psora, Psoriasis, Antipsoric, Homoeopathy.
Introduction
Dr Hahnemann after years of practice reached to the conclusion that all chronic diseases were the result of the chronic miasms, 7/8th of which he termed Psora (conditions arising from the suppression of ‘itch-like eruptions’ by non-homoeopathic means) and the remaining 1/8th being divided between Sycosis (a past suppression of gonorrhoea) and Syphilis (a past suppression of the venereal chancre).[1]
Dr J.H. Allen later added the fourth miasm, Tubercular (conditions arising from the suppression of tuberculous affections by non-homoeopathic means) and it is recognised that many of the manifestations of this tubercular miasm are reflected as a combination of psora and syphilis.[1]
The consideration of miasms is of paramount importance in effective homoeopathic prescribing particularly in this world of multi-suppressions where perceiving a clear picture of the disease is becoming increasingly difficult.[1]
A Historic Review
Hahnemann spent 12 years of intensive study relating to the presence of miasms to chronic diseases. He had already discovered and was employing the principles of the Law of Similia and the doctrine of drug dynamisation to great effect.
However, he became perturbed by the seeming recurrence of certain conditions, which appeared previously to have been successfully treated with suitable homoeopathic remedies.
Dr Hahnemann wrote, “What was the reason for the thousands of unsuccessful endeavours to heal the other diseases of a chronic nature so that lasting health might result? Might this be caused, perhaps, by the still to the small number of Homoeopathic remedial means that have so far been proved as to their pure action?”
But this excuse or so-called consolation never satisfied the founder of homoeopathy – particularly because even the new additions of proved valuable medicines increasing from year to year, did not advance the healing of chronic diseases by a single step, while acute diseases were not only passably removed, by means of a correct application of Homoeopathic remedies, but with the assistance of the never-resting, preservative vital force in our organism found speedy and complete cure.
The answer to this question which is so natural inevitably leads me to the discovery of the nature of these chronic diseases.”[2]
The answer was the ‘ Chronic Miasms,’ which are the fundamental cause of all chronic diseases and need to be taken care of to achieve cure.
Importance of Miasmatic Diagnosis
Dr Hahnemann had said that homoeopathic physician in cases of chronic diseases, has not only to combat the disease presented before his eyes but that he has always to encounter some separate fragment of a more deep-seated original disease i.e the chronic miasm. He also called them primitive maladies.
Dr Hahnemann further instructs, “He, therefore must first find out as far as possible the whole extent of all the symptoms belonging to the unknown primitive malady before he can hope to discover medicines. By this method, he may then be able to heal and wipe out the malady in its whole extent.”[2]
A thorough dissection and incorporation of miasm in each case will help a homoeopathic prescriber in many ways:
⦁ A deep-acting anti-miasmatic medicine by virtue of its centrifugal action will open up such cases (bring to the surface the suppressed symptoms) where the totality of symptoms cannot be framed due to a scarcity of symptoms (i.e. one-sided cases), and those cases with conjoint or contaminated pictures due to various physical, emotional or iatrogenic suppressions.
⦁ Also of importance is the value of selecting an anti-miasmatic medicine, which covers the psychic essence, nature and character of the individual in the absence of any recognizable totality.
⦁ To evaluate the necessity of a change in the plan of treatment or a change of remedy; when few symptoms have disappeared after the first remedy has been administered, yet the miasmatic totality shows the preponderance of the same miasm on the surface as that which was originally covered by the initial remedy. It indicates that the prescriber can stay with that initial remedy.
⦁ To evaluate the homoeopathic prognosis of the case, as removal of layers of suppression are manifested as clarity of symptoms and also reflected by a quantum jump in the sense of well-being.
⦁ Anti-miasmatic medicines help to clear up the suppressions (in relation to the past); clear up the presenting symptoms from their root or origin (in relation to the present), and clear up the susceptibility to get the infection and thereby strengthening the constitution (in relation to the prophylactic aspect or future).
The proper miasmatic diagnosis of each case can uproot the underlying cause and miasmatic prescribing is, therefore, both curative and preventive.[1]
Psora: Mother of all diseases
Dr Hahnemann explains “Psora is the most ancient, most universal, most destructive and yet most misapprehended chronic miasmatic disease which for many thousands of years has disfigured and tortured mankind, and during the last centuries has become the mother of all the thousands of incredibly various acute and chronic (non-venereal) diseases by which the whole civilized human race on the inhabited globe is being more and more afflicted. It is the most infectious most general of all the three chronic miasms.[2]
Dr Kent says, “Psora is the beginning of all physical sickness. Had Psora never been established as a miasm upon the human race, the other two chronic diseases would have been impossible, and susceptibility to acute disease would have been impossible. All the diseases of man are built upon Psora; hence it is the foundation of sickness. All other sickness came afterwards.”[3]
Dr Allen J. H. states that one specific cause (outside of venereal disease) lay at the bottom of all, chronic as well as acute expressions of disease; and this unknown, devitalizing principle named as Psora. Today we understand Psora to be a basic miasm, not confined to any special form of eruption upon the skin of the individual, but that is the parent of a multitude of functional and pathological changes that take place in the human organism.[4]
Dr Robert H. A. says, “The vast majority of the diseases on the earth came under this great classification, which has been called the mother of all diseases; and Hahnemann found that there was a traceable relationship between these chronic manifestations and the many various plagues which had troubled the people on the earth since the most ancient times, manifesting themselves in various ways. Hahnemann became convinced that these recurring symptoms owed their existence to this chronic miasm, he called psora, and that of itself, this condition could never be cured.”[5]
Manifestations of Psora
Psora is an imbalance due to deficiency; to insufficiency, inhibition, to an alteration in rhythm in the sense of less, all the organs and their cells producing an insufficiency.
In the mental realm, inhibition cannot make the individual smaller or reduce him in any way, it cannot lessen his will or diminishes his understanding, but it can cause them to remain stationary, bind or anchor them, benumb them, make him less aware of them, limiting his mental life to the contemplative, imaginative conceptual. This is the mental process of the psoric person.
The psoric will appear timid or reserved, lax or indifferent; any possible irritation or transient excitement will sooner or later leave him drained, cold and sensitive, delicate because of his natural resistance.
Anxiety in many diverse forms. Very fearful that others will observe his apprehension, fearful of suffering some misfortune.[6] Uneasy, frightful, vivid dreams.
Physically psoric patients have unhealthy, cracked skin. Dry skin on limbs, arms. Here or there a rough, scaling spot on the skin, which causes at times a voluptuous itching.
Frequent one-sided headaches, flushes of heat and redness of the face. Long continued obstruction of one or both nostrils. Frequent fluent coryza. Much phlegm in throat. Bad smell from the mouth, slightly sour, also putrid.
Sensation of emptiness in the abdomen. Repugnance to milk. Cutting pains in the abdomen. Hard stools, delaying usually more than a day. Passing of mucus from the anus with faeces.
Predisposition to strains, even from carrying or lifting a slight weight. Cracking of one or more joints on moving.
Most of the ailments come on at night and are increased with a low barometer, in winter, and towards spring.[2]
Psoriasis
Psoriasis is a chronic non-infectious inflammatory skin disorder, characterized by well-defined erythematous plaques bearing large adherent silvery scales. It can start at any age but is rare under 10 years, and appears most often between 15 and 40 years. It is a long-lasting autoimmune disease. These skin patches are typically red, dry, itchy, scaly varying in shape and size and may coalesce to form geographical patterns.[7]
Clinical appearance
There are various presentations of psoriasis, the main are following –
⦁ Plaque (Psoriasis vulgaris) – This is the most common type and affects 85%–90% of people with psoriasis. [7]
⦁ Guttate – Consists of widespread small pink macules that look like drops of paint.[8]
⦁ Pustular psoriasis – Characterized by sterile, neutrophil-derived pustules in a generalized or localized pattern. [7]
⦁ Erythrodermic – This is also rare and can be sparked off by the irritant effect of tar or dithranol, by a drug eruption or by the withdrawal of potent topical or systemic steroids. The skin becomes universally and uniformly red with variable scaling.[7] The main characteristics of psoriatic lesions are:
⦁ Plaques
⦁ Scaling
⦁ Erythema
⦁ Pustules
Diagnostic Features
Psoriasis is largely a clinical diagnosis, though a careful review of contributing factors and screening for psoriatic arthritis is important. Psoriasis must be differentiated from other papulosquamous disorders including seborrheic dermatitis, and chronic eczema.
Sharp demarcation and thick, scaly, red plaques characteristic of psoriasis help to differentiate psoriatic lesions from those of seborrheic dermatitis, which are less well-demarcated.
Chronic eczema may produce scaly plaques, but they are frequently less well-demarcated and less erythematous, allowing differentiation from psoriasis. [9]
Causes
The exact cause of psoriasis is not known but is believed to have a genetic component. HLA-Cw6 is the phenotype most strongly associated with psoriasis, particularly the early-onset variety in which hereditary factors seem to play the greatest part. Factors that may aggravate psoriasis include stress, excessive alcohol consumption, smoking, climatic changes, etc. [7]
Management
Therapy is directed at effectively managing acute flares and maintaining a limited or disease-free maintenance phase. Both topical and systemic medications are enlisted. Topical medications comprise first-line therapy for limited disease.[8]
Case
A female patient aged 57 years comes on 2nd Jan. 2019 with the chief complaints of red, inflamed, scaly, itchy eruptions on extremities and abdomen (Fig.1, Fig.2). It was pre-diagnosed as Psoriasis and she was suffering from it for the last 25 years. It was previously treated as eczema and fungal infection with topical steroids unsuccessfully. She had also taken various other herbal and ayurvedic treatment. The patient also had received Beta-blockers during the period of remission. Examination revealed hyperkeratotic plaques on extremities and abdomen.
The itching was severe and was aggravated by scratching, which resulted in burning, still was unable to control it and had the desire to scratch constantly. It aggravated at night, especially after lying on the bed.
Lesions were widespread chiefly on both limbs and abdomen. The complaint had started 25 years back, first on lower limbs then they gradually spread on other areas. The patient has taken various other treatments all over the years for Psoriasis including topical steroids and oral steroids but with only temporary relief.


Past history
She was suffering from joint pains esp. knees since 7 years. Taking physiotherapy for the same.
Family history
Patient’s mother and one sister also had a history of psoriasis as well. Her father had died 5 years back due to COPD.
Personal history
The patient is thermally hot and cannot tolerate the summer season. She is vegetarian by diet and had a good appetite and not able to tolerate hunger for long. She has an extreme liking for sweets, mangoes and spicy food. She also complained of unsatisfactory stools with thirstlessness. She perspires profusely. Sleep is also disturbed due to itching which is aggravated at night.
Mentals
Patient belongs to a middle-class family. During the conversation, she revealed that she gets angry easily when someone does not work properly. She said, ‘it irritates me when someone doesn’t listen to my instructions and become careless in their work; I need everything clean and properly arranged.’
Her son revealed that she was in habit of always finding faults and criticizing them for their work. She says, ‘I can do all the household chores myself and wants that everyone does their work properly. If I can do such hard work at this age then why can’t the young ones.’
She is very religious. Spends most of her morning in religious rituals. Doesn’t eat until she performed morning prayers. When asked about her fears, she revealed a marked fear of snakes.
Diagnosis
Differential diagnosis – Eczema, Dermatitis, Psoriasis
Final diagnosis – Psoriasis Vulgaris (ICD-10 classification – L40.0) [10]
Miasmatic Diagnosis –
The miasmatic diagnosis was made after a thorough analysis of the case and considering presenting complaints, past complaints, patient’s mental & physical symptoms as well as family history.[1], [2]
| Sr.No | Symptom | Psora | Sycosis | Syphilis |
| 1 | Red, inflamed, scaly, itchy eruptions | +++ | ||
| 2 | Itching aggravated at night | ++ | ++ | |
| 3 | Voluptuous Itching | +++ | ||
| 4 | History of Suppression of Eruptions | +++ | ||
| 5 | Joint pains; osteoarthritis | ++ | ++ | |
| 6 | Family history of Psoriasis, eczema | ++ | ||
| 7 | Desire sweets | +++ | ||
| 8 | Desire Spicy food | +++ | ||
| 9 | Unsatisfactory Stools, constipated | +++ | ||
| 10 | Angers easily/irritability | + | +++ | |
| 11 | Hard working | +++ | ||
| 12 | Fear of snakes | +++ | ||
| 13 | Religious | +++ | ||
| 14 | Fastidious | ++ | ||
| 15 | Criticizing nature | ++ |
The above analysis clearly indicates the predominance of Psoric miasm. Nature of the disease is also significant in miasmatic diagnosis. As the pathology is on the surface in the form of dry psoriatic lesions, it also confirms the miasmatic diagnosis as Psora.
Analysis and Evaluation of Symptoms
| Mental general | Physical general | Physical particular uncommon | Physical particular common |
| Gets angry easily | not able to tolerate hunger for long.2+ | Itching aggravated at night on lying on bed.3+ | red, inflamed, scaly, itchy eruption on extremities and abdomen.3+ |
| need every thing clean and properly arranged.2+ | She likes sweets3+, mangoes and spicy food.2+ | Itching resulted in burning, still she is unable to control it and likes to scratch3+ | Itching was severe and was aggravated by scratching, which resulted in burning.3+ |
| habit of always finding faults and criticizing2+ | unsatisfactory stool | ||
| Very religious Spends most of her morning in religious rituals.3+ | thirstless | ||
| Very hardworking2+ | Sleep is also disturbed due to itching.3+ | ||
| Fear of snakes2+ | Profuse perspiration2+ |
A thorough analysis of symptoms clearly indicates that the case has got characteristic mental and physical general symptoms. Hence, mental and physical generals of the case were given more importance in the totality.
Totality of Symptoms
Totality was formed as per Dr Kent’s method i.e. from ‘generals to particulars’ where mental symptoms of the case were given prior importance followed by physical generals and last physical particulars, as follows–
⦁ Religious
⦁ Fear of snakes
⦁ Hard-working – Industrious
⦁ Finding fault in others and criticizing – censorious
⦁ Fastidious
⦁ Desire sweets, spicy food
⦁ Sleep – disturbed
⦁ Thirstlessness
⦁ Constipation
⦁ Perspiration – profuse
⦁ Itching – voluptuous
⦁ Itching – aggravation at night
⦁ Itching – aggravation in bed
Repertorisation
Repertorisation was done with Synthesis repertory using RADAR 10 software (figure 3) on the basis of totality with the following rubrics:
| Sr.No. | Rubric | Chapter |
| 1 | Religious Affections – too occupied with religion | Mind |
| 2 | Fear – snakes of | Mind |
| 3 | Industrious(=mania for work) | Mind |
| 4 | Censorious | Mind |
| 5 | Fastidious | Mind |
| 6 | Food & Drinks – Sweets – desire | Generals |
| 7 | Food & Drinks – Spices – desire | Generals |
| 8 | Sleep – Disturbed | Sleep |
| 9 | Thirstless | Stomach |
| 10 | Constipation | Rectum |
| 11 | Perspiration – Profuse | Perspiration |
| 12 | Itching – voluptuous | Skin |
| 13 | Itching – night | Skin |
| 14 | Itching – warm – bed; on becoming warm in | Skin |
Figure 3
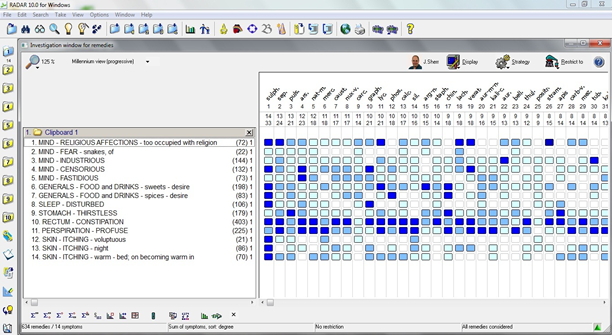
Result of reportorial analysis gives the following remedies:
⦁ Sulphur – 33/14
⦁ Sepia – 24/13
⦁ Pulsatilla Nigricans – 21/13
⦁ Arsenicum Album – 23/12
⦁ Natrum Muriaticum – 18/12
Treatment
On comparing the remedies from the reportorial result Sepia, Pulsatilla and Arsenicum Album were eliminated on the basis of thermals as the patient is hot, while these remedies are predominantly more suited to chilly patients.
Sulphur was selected over Natrum mur, as it not only covers the mental and physical generals but also acts as an anti-psoric remedy.
Following indications of Sulphur from materia medica justifies the selection–
⦁ This is a great Hahnemannian anti-psoric.
⦁ It is a medicine often called for in the suppression of eruptions from cold and from drugs.
⦁ There are vesicular, pustular, furuncular, scaly eruptions, all attended with much itching.
⦁ Many complaints come on from becoming warm in bed.
⦁ As to time aggravations, nightly complaints are a feature.
⦁ Religious melencholy[11]
⦁ Great desire for sweets[12]
⦁ Disposition to criticize[13]
So, Sulphur 30 single dose was prescribed followed by placebo for 15 days.
Follow – up
The patient was advised to stop all the other medications including the topical creams and lotions. Initially, follow-ups didn’t show a marked improvement but the only general well-being was noticed. Subsequently, the patient started showing a gradual reduction in redness and itching. Detailed follow-ups are as follows –
| Follow-up | Date | Complaints | Prescription |
| Follow-up 1 | 16/01/2019 | No improvement in itching. Constipation better. No other significant change. | Placebo was prescribed for 15 days |
| Follow-up 2 | 31/01/2019 | Itching reduced , with reduction in redness of the eruptions. Stools – satisfactory | Placebo was prescribed for 30 days |
| Follow-up 3 | 05/03/2019 | Itching reduced with marked reduction in eruptions. Sleep – refreshing Stools – satisfactory | Placebo was prescribed for 30 days |
| Follow-up 4 | 03/04/2019 | Eruptions reappear with intense itching. Stools – satisfactory No other complaint | Sulphur 200 was given in single dose as on reassessment Sulphur was again verified, so there was increase in potency rather than changing the remedy. Placebo for 30 days. |
| Follow-up 5 | 06/05/2019 | Relief in itching, reduction in eruptions and scales. Stools – satisfactory Sleep – good | Placebo was prescribed for 30 days |
| Follow-up 6 | 04/06/2019 | Most of the eruptions disappear, with only occasional itching.(Fig. 4 & 5) No other complaint. General condition – good. | Placebo was prescribed for 30 days |


Discussion
Successful results in chronic diseases always require a correct anti-miasmatic prescription. For that purpose, Case should be analyzed diligently to make a correct miasmatic diagnosis.
Selection of correct anti-miasmatic remedy paves way for the successful future course of treatment. Careful study of the case and judicial use of repertory are helpful in this manner.
Repertorisation of the above case of psoriasis gave us Sulphur, Sepia, Pulsatilla Nigricans, Arsenicum Album and Natrum Muriaticum as leading indicated remedies.
Sulphur was selected after a thorough differentiation of the leading remedies which can be discussed below.
Sepia – more suited in herpes, chloasma. Itching not better by scratching. Mentally patient is very sad, indifferent to loved ones.[12] Sepia is more suitable to chilly persons, but the patient is thermally hot.
Pulsatilla – It is pre-eminently a female remedy, especially for mild, yielding disposition, which is opposite to the patient’s constitution. Suited in urticaria after rich food, acne at puberty. [12]
Arsenicum Album – Itching with burning which is aggravated by scratching. Mostly all complaints are better by heat, but in this case, heat is intolerable. Unquenchable thirst of arsenic is absent.[12] Suitable to chilly patients.
Natrum Muriaticum – Skin oily, greasy especially in hairy parts. Itching after exertion. Ill effects of grief, fright, anger etc.[12] Characteristics of the chief complaints which are voluptuous itching and aggravation at night are missing.
Sulphur – got an elective affinity for the skin, where it produces heat and burning with itching; made worse at night and also by the heat of bed. Religious melancholy. No regards for others. Great Hahnemannian anti-psoric.[11]
Result of the case reaffirmed the efficacy of homoeopathy in cases of psoriasis as reported by various homoeopathic physicians around the globe.
Conclusion
Psora is the mother of all miasm and is alone responsible for most of the chronic diseases of mankind and manifests itself in varying forms. Timely treatment of Psora with suitable anti psoric treatment prevents the patient from developing more severe forms of diseases of sycosis and syphilis.
Moreover from the above case, we can also conclude and reconfirm that anti miasmatic treatment is proved beneficial in chronic cases like psoriasis if given after proper case taking and analysis as per the laws of homoeopathy.
References
⦁ Banerjea Subrata Kumar; Miasmatic prescribing; Second edition; New Delhi, India; B.Jain Publishers (P) Ltd.; 2010; P. 1, 4, 6
⦁ Hahnemann Samuel; The chronic diseases, their peculiar nature and their homoeopathic cure; Rearranged and Augmented edition; New Delhi, India; B.Jain Publishers (P) Ltd.; 2017; P. 5, 11,
⦁ Kent James Tyler; Lectures on Homoeopathic Philosophy; Reprint Edition; New Delhi, India; B.Jain Publishers (P) Ltd.; 1999; P.126
⦁ Allen J. Henry; The Chronic Miasms; Student Edition; Volume I II; New Delhi, India; B.Jain Publishers (P) Ltd.; 2004
⦁ Roberts H.A; The Principles and Art of Cure by Homoeopathy; Third edition; New Delhi, India; B.Jain Publishers (P) Ltd.; 2005
⦁ Ortega P.S; Notes on The Miasms; First English edition (translated by Dr Harris Coulter); New Delhi, India; National Homoeopathic Pharmacy; 1980; P. 63, 64
⦁ Hunter J., Savin J. and Dahl M; Clinical Dermatology; Third edition; Massachusetts 02148-5018, USA; Blackwell Publishers; 2003; P. 48
⦁ Buxton P.K.; ABC of dermatology; Fourth edition; Tavistock Square, London; BMJ Publishing Group Ltd.; 2003; P. 8-9
Council M.L., ⦁ Sheinbein D., ⦁ Cornelius L.A.; The Washington manual of dermatology diagnostics; first edition; ⦁ Philadelphia, Pennsylvania, United States; Wolters Kluwer Health publishers; 2015; P. 42-43
⦁ World Health Organisation website; ⦁ https://icd.who.int/browse10/2016/en#/L40; International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10)-WHO Version; 2016
⦁ Kent J.T; Lectures on Homoeopathic Materia Medica; Reprint edition; New Delhi, India; B.Jain Publishers (P) Ltd; 2005
⦁ Boericke W.; New Manual of Homoeopathic Materia Medica & Repertory; Augmented edition based on Ninth edition;New Delhi, India; B.Jain Publishers (P) Ltd.; 2001; P. 598-599
⦁ Clarke J.H.; A Dictionary of Practical Materia Medica vol.III; Reprint edition; New Delhi, India; B.Jain Publishers (P) Ltd.; 2004; P.1308
Author:
Dr Siddharth Saurabh, M.D.( Hom.), MUHS, Nashik
Reader & H.O.D, Dept. of Repertory,
Ahmedabad Homoeopathic Medical College, Ahmedabad
Dr Shilpi Agrawal, M.D. (Hom.)
R.M.O, Sainath Hospital,
Ahmedabad Homoeopathic Medical College, Ahmedabad