ABSTRACT:
A narrative review on history of calcaneal enthesophytes with its understanding on anatomical aspect of heel, classification according to location, its prevalence over the world and in India, with the various hypothesis to justify its cause, followed by symptomatology, radiological investigation and conclusion with its general management and homoeopathic remedies.
Many people come up with the complaint of severe heel pain which alter their day-to-day activities and it alarms a patient to professionally approach the consultant. Calcaneal enthesophytes with pain and activity limitations are the point to be considered in population suffering. Calcaneal enthesophyte is an abnormal bony outgrowth at the inferior or dorsal part of the calcaneus. Some of the assessment scales are used to assess quality of life of the patients.
As some of the homoeopathic remedies are known for their cure in bony exocytosis, it has been used as source for management of calcaneal enthesophytes cases. Some helps in both relieving pain in heels due to spur and also in dissolving spurs. It is a safe and effective mode in management of the cases.
ABBREVIATIONS: calcaneal spur[CS], quality of life[ QOL], plantar calcaneal spur[PCS], dorsal calcaneal spur[DCS], International Classification of Diseases[ICD], body mass index [BMI], diabetes mellitus[DM], non-steroidal anti-inflammatory drug[NSAID], extra-corporeal shock wave therapy[ESWT], ultrasound therapy[UT], endoscopic plantar fasciotomy [EPF], visual analogue scale[VAS], american orthopedic foot and ankle society scale[AOFASS], foot function index score[FFI], aggravation[< ], amelioration[>].
INTRODUCTION:
“Walking through life, we spend most of our energy choosing the right shoes.”- Ljupka Cvetanova
Quality of life can be negatively affected if person is experiencing ongoing pain. Many people come up with the complaint of severe heel pain which alter their day-to-day activities and it alarms a patient to professionally approach the consultant. Calcaneal enthesophytes [CS] with pain and activity limitations are the point to be considered in population suffering.
HISTORY:
For the first time in 1900, A German physician named PLETTNER, discovered the bony outgrowth in routine X-ray and termed it as “KALKANEUSSPORN”.1
DEFINITION:
CS also known as enthesophytes are the abnormal bony projections from the back or underside of the heel bone [figure-1]2& that may make walking painful.3
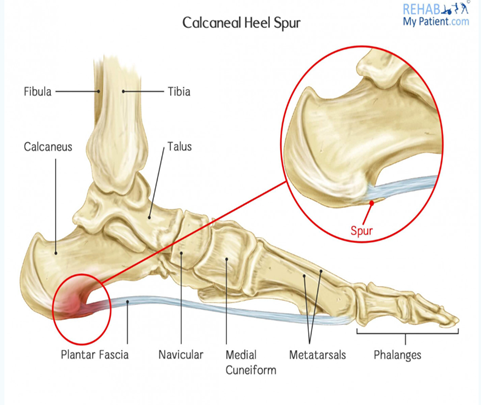
ANATOMY:
The os calcis is the largest tarsal bone amongst 7 bones, which forms prominence of the heel. Its significant role is in weight bearing, gait and posture.
Inferior aspect of heel: Plantar fascia is flat band of ligament that inserts into medial process of the inferior tuberosity, it maintains foot arch.1
Posterior aspect of heel: Achilles tendon is band of fibrous tissue that connects the gastrocnemius and soleus muscle to posterior calcaneal tuberosity. Its function is to dissipate stress exerted upon the region during motion.1

CLASSIFICATION OF HEEL SPURS:
Based on location:
1] INFERIOR/ PLANTAR CS [PCS]:Spur located in inferior aspect of heel, superior to plantar fascia [figure-2]4. Majority of PCS arise from medial process of tuberosity and commonly associated with plantar fasciitis.
2]POSTERIOR/DORSAL CS [DCS]:Spur located back of the heel [figure-2]4 at insertion of achilles tendon, commonly associated with achilles tendinopathies.3
| Figure 2: represents types of calcaneal enthesophytes.4 |
CLASSIFICATION OF CS ACCORDING TO ICD- 10:
According to International Disease Classification, calcaneal spur is classified under specific code: ICD-10-CM codes
M77.3–Calcaneal spur
- M77.30—Calcaneal spur, unspecified foot
- M77.31—Calcaneal spur, right foot
- M77.32– Calcaneal spur, left foot5
PREVALANCE:
- According to the study, PCS is prevalent at the rate of 11% in India, 13% in Ireland, 15% in Zimbabwe, 16% in Thailand, 17% in Europe, and 21% in America.6
- A Study conducted in Indian population to assess the incidence of CS was reported total of 26.5%. Incidence of 15.5% was of DCS and of PCS was 6.5%. 7
AETIOLOGY AND PATHOLOGY:
Several theories have been proposed to understand the cause:
- In 1912, Ronald hypothesized that the epiphysis of the calcaneum extends down to plantar aspect and repetitive trauma results in PCS formation.
- In 1939, Beltane conducted study of 18 patients with flatfoot [Pes Planus] resulting in 40% with spur.1
- In obesity- plantar fascia tension increases when medial longitudinal arch is lowered. Increased body weight leads to pressure during walking.
- PCS is considered as part of normal process of aging, with tendency of ligaments and tendons to ossify. Whereas in DCS it occurs as result of traction.
- 6
RISK FACTORS: A retrospective homoeopathic study conducted in India,2017 specifies about risk factors below.8
AGE: Commonly seen in age group of 40-70years with increased prevalence in older age group. Out of 76 patients suffering from heel pain with CS;18‑35 years- 10 (13.16%), 35‑50 years- 32 (42.10%]; 50‑75years- 34 (44.74%).
SEX: In younger population, female, less than 49 years of age have high incidence than men.17 males (22.37%); 59 females (77.63%).
OBESITY: Prevalence of PCS increases with weight. BMI in these people is calculated to assess obesity.Obese(>27)—5 (6.58%), overweight(>23)- 39 (51.31%), normal (17-23) -30 (39.47%), below normal(<17) –2 (2.63%).
FOOT POSITION AND GAIT:People with flat-footare prone to have PCS with heel pain. Women wearing high heeled footwear cause high arch foot, abnormal gait, continuous standing or walking, etc.
SPORTS ACTIVITY: Continuous running, i.e. in athletes or any other sports activities with repeated trauma to the heel tissue with heel pain may develop CS.
ARTHROPATHY: Includes osteoarthritis, ankylosing spondylitis, reiter’s syndrome, diffuse idiopathic skeletal hyperostosis. Osteoarthritis 8(10.53%) patients with CS.
DIABETES MELLITUS: Increased incidence in type 2 DM.4 [5.27%] DM patients were sufferers.
SYMPTOMS:
- Pain- worse on walking, running, prolonged standing, lifting heavy weight.3
DIAGNOSTIC CRITERIA:
- Clinical presentation
- Physical examination:
- Range of motion of ankle and foot
- Palpation of proximal plantar fascia attachment to rule out any tenderness or deformity
- Swelling on examination
- Evaluation of gait
- BMI evaluation in obese individuals
- RADIOGRAPHY: Lateral foot X-ray of affected side, showing osteophytes on posterior/inferior aspect of calcaneum.
- MRI study– in rare, painful cases. 3
DIFFERENTIAL DIAGNOSIS:6
- Calcaneal fractures—Aetiology–repetitive overload to the heel.3
- Baxter nerve entrapment – neuropathic heel pain with abductor digiti minimi atrophy.6
- Haglund deformity
— is in prominence of the superior aspect of the posterior calcaneus. Repeated pressure, from this deformity or from ill-fitting footwear, can cause inflammation and swelling between the calcaneus and achilles tendon, leading to retrocalcaneal bursitis.9 Severdisease (calcaneal apophysitis) — usually occurring between 5-11 years of age. Bones grow quicker than the muscles and tendons in these patients.
Diagnosis: Radiography is usually normal, may reveal a fragmented or sclerotic calcaneal apophysis.10
- Heel fat pad syndrome—atrophy or inflammation of shock absorbing fatty pad.3
MANAGEMENT:
CONSERVATIVE TREATMENT:
- Orthotic insoles, night splints, heel inserts
- Analgesics, NSAIDs.
- Cortisone injections.
- Physical Therapy:
1] Extracorporeal Shock Wave Therapy [ESWT]
2] Ultrasound Therapy [UT]
SURGICAL TREATMENT:
INDICATIONS: 1] Failure of all conservative measures.
2] Very large spur causing compression of heel structures.
- Endoscopic plantar fasciotomy [EPF] with resection of spur11
Assessment scales are used to assess scores for functional evaluation, used pre-operative and post-operative respectively.
- VISUAL ANALOGE SCALE [VAS]
- AMERICAN ORTHOPAEDIC FOOT AND ANKLE SOCIETY SCALE [AOFASS]
- FOOT FUNCTION INDEX SCORE [FFI]12
HOMOEOPATHIC REMEDIES:
Some of the commonly indicated remedies for heel spur with or without pain includes:
CALCAREA FLUORICUM:
•Loss of calcium in the system follows with a hard, knotty exudation on the surface of a bone. Osseous growth and enlargement of bone with or without carries, particularly of traumatic origin. Boring pain and heat in parts.Swelling or indurated enlargements, present in fasciae, ligaments of joints or in tendons.13
•Indurated swelling, malnutrition of bones, principally used for dispersing bone growths. Ulceration of bones, exostosis. ‘Osseous tumors, enlarged bones with or without caries’.14
RHUS TOXICODENDRON:
•Swelling, stiffness, pain on first motion after rest or on getting up in morning; >constant motion.15
•Lameness in tendons, ligaments. Ailments from cold, damp weather, sensitive to cold and > warmth.16
VALERIANA OFFICINALIS:
•Pain in heels when sitting.17
•Drawing pain in tendo-achilles when sitting, pain in heel during rest.16
AMMONIUM MURATICUM:
•Ulcerative pain in heels.17
•Pain of ulceration and pulling in heels, > – by rubbing, feet get very cold in evening in bed.Pain – stitching, tearing type, heel pain on walking, morning.15
ARENIA DIADEMA:
- Bone pains in extremities, pain in os-calcis alternating with numb feeling, sensation of swelling, periodicity, extreme sensitive to cold.17
- Boring, digging pain in os-calcis, continues on moving foot and disappears by continuous motion.15
AURUM METALLICUM:
- Exostosis with nightly pain in bones >- open air, complaints from sunset to sunrise.17
- Boring in bone, pain drives patient out of bed at night and makes him to walk.16
- Affections on bones resulting from abuse of mercury, syphilis, tearing pain in joints and bones of feet and toe.14
MEZEREUM:
- Bone pain. Bruised, weary feeling in joints, intolerable to touch.17
- Pain in periosteum <night, least touch. Violent pain in bones of feet, bones of instep< when walking.15
MIASMATIC UNDERSTANDING:
P.S. Ortega introduced three forms of alterations of cellular functions, which can be imagined, includes: 1] DEFICIENCY [perturbation], 2] EXCESS [accumulation], 3] PERVERSION [degeneration]. It is significant to the Hahnemannian concept of chronic Miasms – PSORA, SYCOSIS, SYPHILIS respectively.18
As in the above condition, complaints start with psoric symptoms of functional disturbance like pain and inflammatory changes, followed by sycosis in which tissues are produced in excess and calcium gets deposited to form spur, following prolonged suffering leading to degenerative changes in plantar fascia heading towards syphilitic miasm.
CONCLUSION:
Calcaneal spur, an abnormal bony outgrowth at the inferior and dorsal part of calcaneus has a huge impact on QOL of patients with chronic suffering. Homoeopathic applicability in these cases would be beacon light in improving the bony exostosis. The purpose of this study is a commencement for our further homoeopathic interventional study on CS.
REFERENCES:
1] Lindsay M: Bioarcheological implications of CSs in the Medieval Nubian population ofKulubnarti, University of Colorado at Boulder, April2016 https://www.google.com/search?q=Bioarcheological+implication+on+calcaneal+spur&oq=bio&aqs=chrome.0.69i59j69i57j0l5j69i60.21674j0j7&sourceid=chrome&ie=UTF-8# Accessed on 25/2/20202]
2] Calcaneal spur/Rehab my patient [ fig:2 reference]
https://www.rehabmypatient.com/ankle/heel-spur
3]Calcaneal spurs- Physio-pedia
https://www.physio-pedia.com/calcaneal-spur#. Access on 19/3/2020
4]Calcaneal spur-plantar fasciitis [fig:3 reference for types of CS]
https://www.vectorstock.com/royalty-free-vector/calcaneal-spur-plantar-fascitis-set-medical-vector-2938
5]The ICD-10-CM Codes, Classification of Diseases of the musculoskeletal system, Clinical Description and Diagnostic Guidelines; Geneva, World Health Organisation.
https:/www.icd10data.com
6] Joshua K, Omid Y, Mirjalili SA: The plantar CS: A review of anatomy, histology, etiology and key associations,March2017,doi:10.1111/joa.12607
https://www.google.com/search?q=calcaneal+spur+articles&oq=calcaneal+spur+articles&aqs=chrome..69i57j0l3.11855j0j8&sourceid=chrome&ie=UTF-8# accessed on 20/3/2020
7] Kullar JS, Randhawa GK, Kullar KK: A study of calcaneal enthesophytes in Indian population, March 2014
http://www.ijabmr.org/text.asp?2014/4/3/13/140709 accessed on 13/1/2020
8] Parveen S: A Retrospective study of homoeopathic treatment in patient with heel pain with or without CS, India J Res Homoeopathy 2017; 11:6473
http://www.ijrh.org/text.asp?2017/11/1/64/200844 Accessed on 5/12/2019
9] Haglund’s Syndrome: A commonly seen Mysterious condition
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5101401
10] Sever Disease- Orthoinfo
https://orthinfo.aaos.org/en/diseases—condition
11] Thordarson David B: Orthopaedic Surgery Essentials Foot & Ankle; second edition; Series editors, chapter -9,page -217
12]Ersinkuyucu, Figenkocyigit, Mehmet erdil: The association of calcaneal spur length and clinical and functional parameters in plantar fasciitis, International journal of Surgery 2015, Elsevier publications
http://dx.doi.org/10.1016/j.ijsu.2015.06.078
13]Boericke W, Dewey W: The Twelve Tissue Remedies of Schussler, Sixth edition, B Jain publications, page no:37-43
14] Gupta Das DC: Characteristic Materia medica with Leading Therapeutics, revised fourteenth Edition, reprint Edition-2005,B. Jain publication ltd, Pg. No-186-187
15]Clarke JH, A dictionary of practical Materia medica 3 volume, first edition, Jan 2005, B.Jain publications ltd.
16] Kent JT, L[D1] ectures on Homeopathic Materia medica, reprint edition July 2018, B.Jain publications ltd.
17]Boericke W, Pocket manual of homeopathic Materia medica and repertory, edition 2002, B. Jain publications ltd.
18] Ortega P, English translation by Coulter H: Notes on the Miasm, First English edition-1980, Published by National Homoeopathic Pharmacy New-Delhi, pg.no- 53-54
About the authors:
Dr Smita Balunnavar, PG Scholar, Department of Practice of Medicine, A.M. Shaikh HomoeopathicMedical College, Hospital and P.G. Research Centre,Nehru Nagar, Belagavi-590010, Karnataka.
Dr Jyothi Vijayakumar, M.D., Professor, Guide and Head of Department,Department of Practice of Medicine, A.M. Shaikh Homoeopathic Medical College, Hospital and P.G. Research Centre, Nehru Nagar, Belagavi-590010, Karnataka.
Dr Shweta Nanjannavar, M.D., Associate Professor and Guide o Practice of Medicine, A.M. Shaikh Homoeopathic Medical College, Hospital and P.G. Research Centre, Nehru Nagar, Belagavi-590010, Karnataka.