Abstract: In medical research, the case study approach allows in depth and multi-dimensional exploration of complex issues in real life settings of the SICK. Perceiving complex issues in a given time axis with emphasis on cause effect, conation cognition and affect in accordance to the evolving adaptation pattern and the defense mechanisms that come to the surface in the form of emotional disturbances. Eventually there is breakdown of the coping mechanism and the status of health turns into disease. This case demonstrates the above concept of genesis of a psychiatric disease evaluated on various psychiatric assessment scales and demonstration of methodology for arriving at the simillimum.
Keywords: Anxiety, homoeopathy, psychiatric, assessment scales, research.
Abbreviations: BAI: beck’s anxiety inventory, CBT: cognitive behavioral therapy, DSM V: diagnostic and statistical manual of mental disorders, 5th edition, GAD: generalised anxiety disorder, HAM-A: Hamilton anxiety rating scale, H-husband, MSE: mental state examination, PSS: perceived stress scale, BDS – bachelor of dental surgery.
Introduction:
Generalised anxiety disorder (GAD) is the manifestation of excessive worry in one or more areas of one’s life. The worries may be focused on keeping schedules, family finances, relationships, and perfectionism-themes that are more typically concerns for adults. [1] GAD is a prevalent, chronic, debilitating disorder. [2] The prevalence of mental disorders is high, with reports of up to 30% in the general population. [3] Anxiety and mood disorders account for the largest percentage of mental disorders by far. Results of the national comorbidity survey replication indicate a 12-month prevalence of 18.1% for anxiety disorders and 9.5% for mood disorders. [4]
Psychiatric assessment scales are short, easy to administer and sensitive to change, therefore particularly applicable where there is the need for screening chronic psychotic populations. [5] These scales helps to arrive at a particular diagnosis and to judge the impact of ongoing disease on the quality of life of that individual. Therefore, homoeopathic health professionals should record every individual case as per the case taking guidelines mentioned in aphorisms 83 to 104. [6] After case recording, individualisation of disease and the patient as a person is of prime importance. For individualisation of disease in context to psychiatric disease diagnosis made as per the DSM because it provides a common language for clinicians to communicate about their patients and establishes consistent and reliable diagnosis that can be used in the research of mental disorders. [7]
Case record:
Mrs. KT, 49 years old lady, an english teacher in ZP school came for her anxiety related complaints. Her husband is 52 years, civil engineer in govt. sector, daughter is in BDS 1st year and son is in 12th standard engineering group. Patient stays in a nuclear family structure and her socio-economic status is upper middle class. Her chief complaints were as follows: –
| Location | Sensation | Modalities | Concomitant |
| Mind Since 1 year Increased since 1 ½ months Frequency: daily Intensity: moderate Duration: continuous Pace: gradually increasing | Anxiety2 Lack of confidence2 Concentration difficult2 Restlessness2 Irritability2 | Ailments from husband’s angioplasty (2 months back) |
= No history of psychiatric illness
= Physical generals: Lean built up, fair complexion, thermal status was hot. Her obstetrical and gynaecological history was uneventful. Rest of the physical generals were normal.
Life space investigation:
- Phase: childhood, teenage, adult and married life: uneventful
- Maternal and in-laws are having well to do family background and they are having respectful position in their community and amongst their relatives.
- Patient is calm by disposition with fondness of being social.
- There is no stress as such.
- Hobbies: Interested in doing household work and studies.
- Shares good interpersonal relationship (IPR) with children, in laws, relatives, friends, neighbours and school staff.
On examination: Vitals normal
Mental State Examination:
1. Appearance: Age appropriate, good level of cleanliness, medium physical condition, well dressed as per Indian tradition.
2. Behaviour: Restlessness, mild anxiety, occasionally avoiding eye contact, no distractions.
3. Speech: Medium to fast rate, loud tone without any flights of dissociation.
4. Mood: Angry when asked about husband. Depressed on enquiry about IPR with husband.
5. Perception: Good.
6. Thought Form: Emotional and associated with the facts.
7. Thought Content: Fixed ideas
8. Cognition: Attention and concentration: Total. Orientation to time, place and person: Normal. Level of comprehension: Normal
9. Insight: Moderate but predominated by emotions.
Psychiatric assessment scales: for evaluation of the cause and severity of the psychiatric illness.
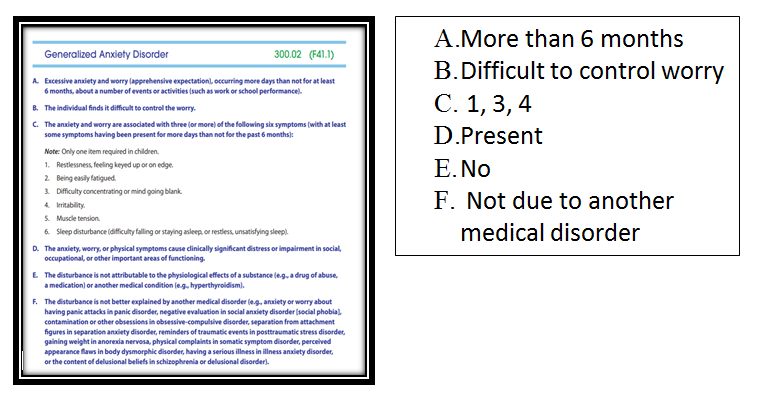
| Fig 5: DSM V Diagnostic Criteria [12] |
| Fig 7: Repertorization |
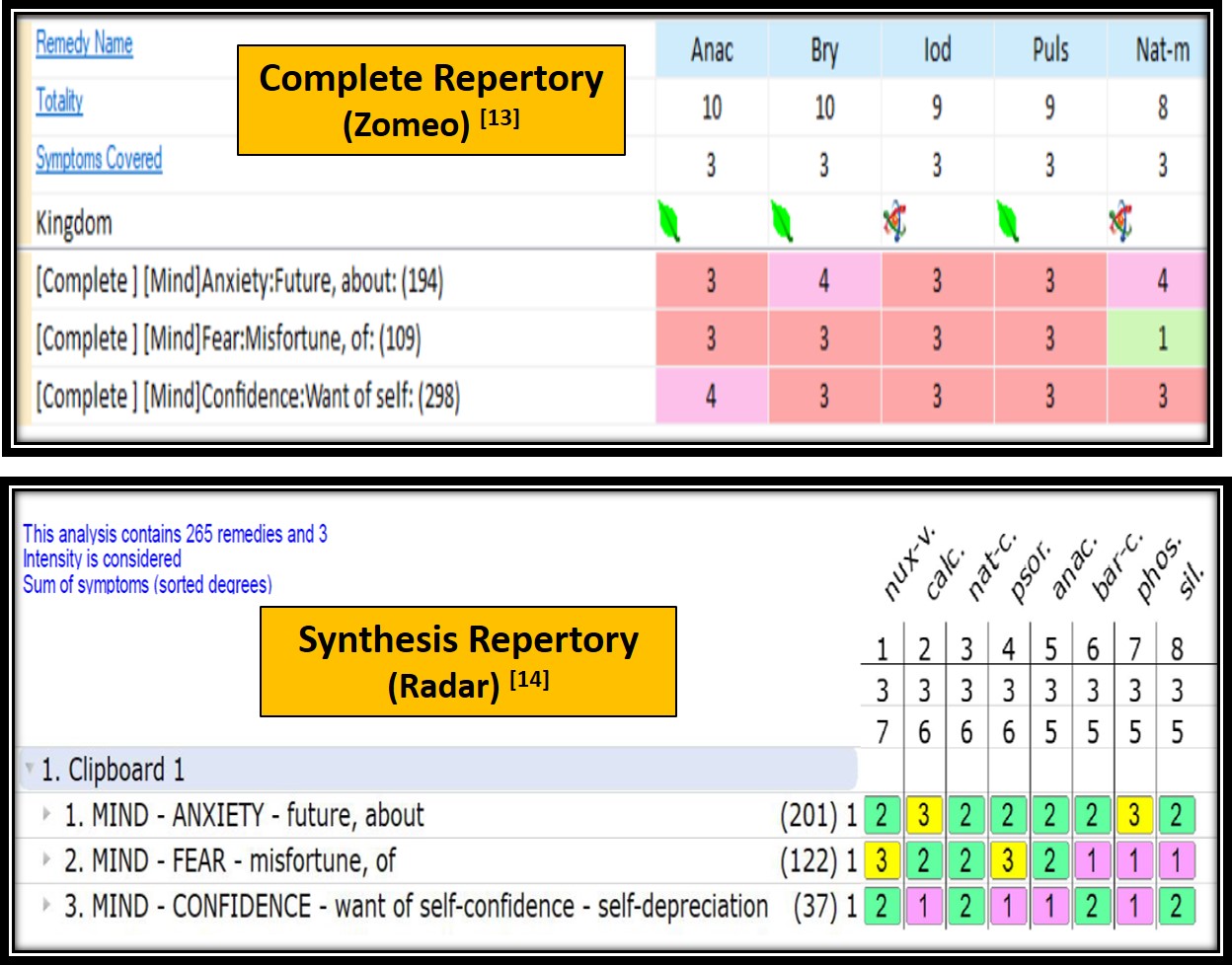
After repertorisation, Anacardium orientale (10/3, 5/3), Bryonia alba (10/3), Calcarea carbonicum (6/3), Iodium (9/3), Nux vomica (7/3) and Pulsatilla nigricans (9/3) were the closely coming remedies. Anacardium orientale was studied as it is covered in Complete and Synthesis repertory.
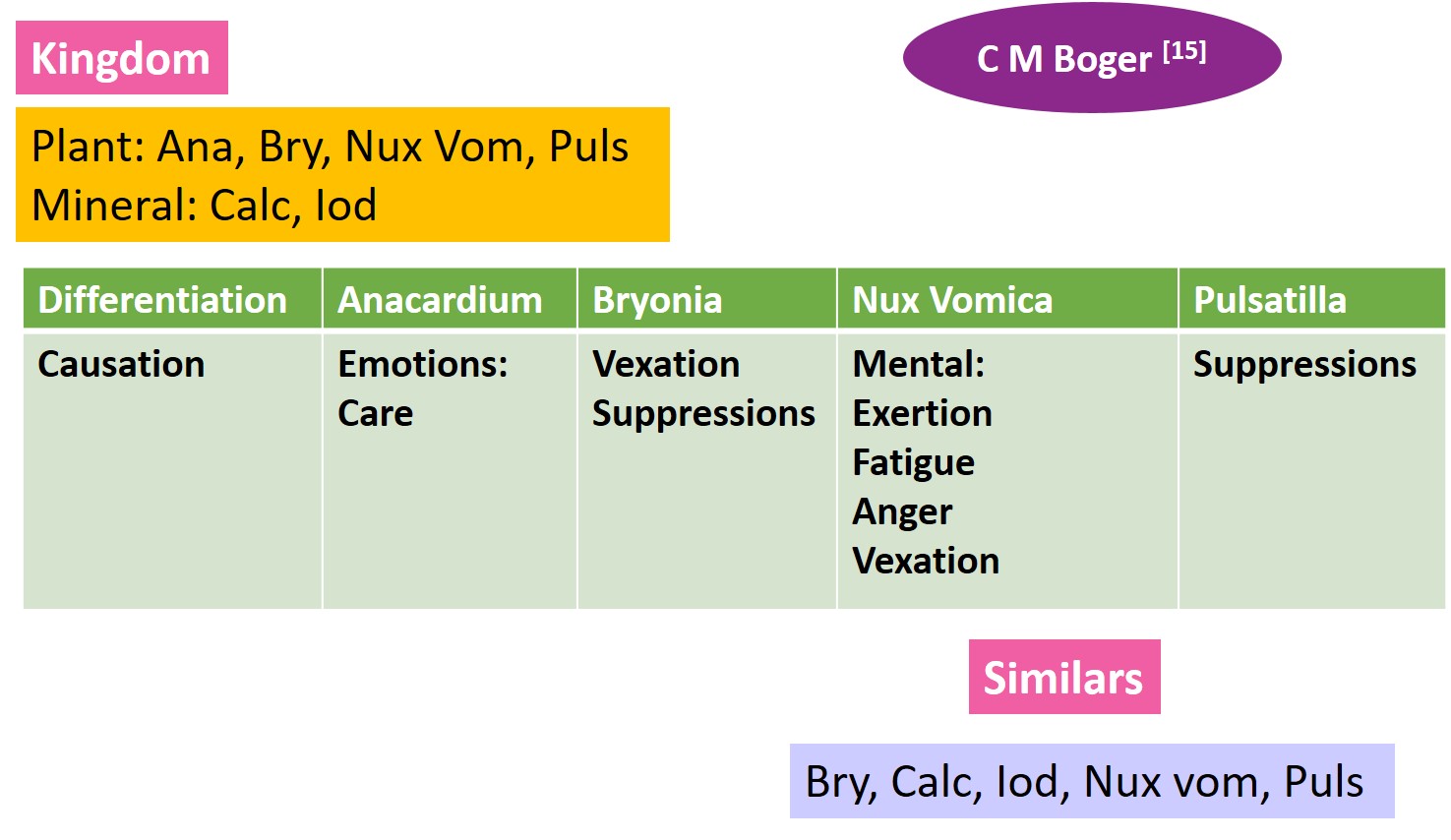
| Fig 8: Materia Medica Differentiation |
Perceiving mind of Anacardium orientale: –
1} The Chronic Diseases [16]: –
- Sadness. {1st symptom}
- Anguish and apprehension as of imminent misfortune. [Becher.]. {2nd symptom}
- Anxiety and apprehension in the evening, after cheerfulness during the day. [Langhammer.]. {3rd symptom}
- Anxious apprehension and deep thoughts, on meditating over his present and his future fate. [Langhammer.]. {7th symptom}
- The future seems to him very dangerous, as if nothing were imminent but misfortune and danger; distrust in his own power, and despondency. {8th symptom}
- He is at odds with the whole world, and has so little confidence in himself that he despairs of being able to accomplish what is demanded of him. {9th symptom}
2} A Synoptic Key of the Materia Medica: –
REGION:
- MIND.
- Nerves: Stomach.
- Skin. Palms.
- Muscles.
- Joints.
WORSE:
MENTAL EXERTION.
Emotions: Anger, fright, care, etc.
3} RADAR: – Section on remedies
- Lack of self-confidence/inferior feeling. Internal conflict.
- Two types: 1] Cruel 2] Helpless, hopeless, pleading, needy.
- Great insecurity and lack of self-confidence (Baryta carbonicum). Irresolution.
- Feels inferior. Often seems very mild during consultation.
- Refuses to admit these feelings, tries to prove himself, creating an INTERNAL CONFLICT.
| Table 1: Planning and programming of homoeopathic Rx |
| Stage of disease | Functional |
| Type of disease | Chronic |
| Classification of disease | One sided mental disease arising from prolonged emotional causes (psycho-somatic) |
| Dominant miasm | Psora |
| Sensitivity | Moderate |
| Susceptibility | Moderate |
| Suppressions (if any) | Emotional |
| Repetition | Infrequently |
| Potency | Moderate (200) |
| Repetition | Infrequently |
| Correspondence | Total |
| General vitality | Good |
| Prognosis | Favourable |
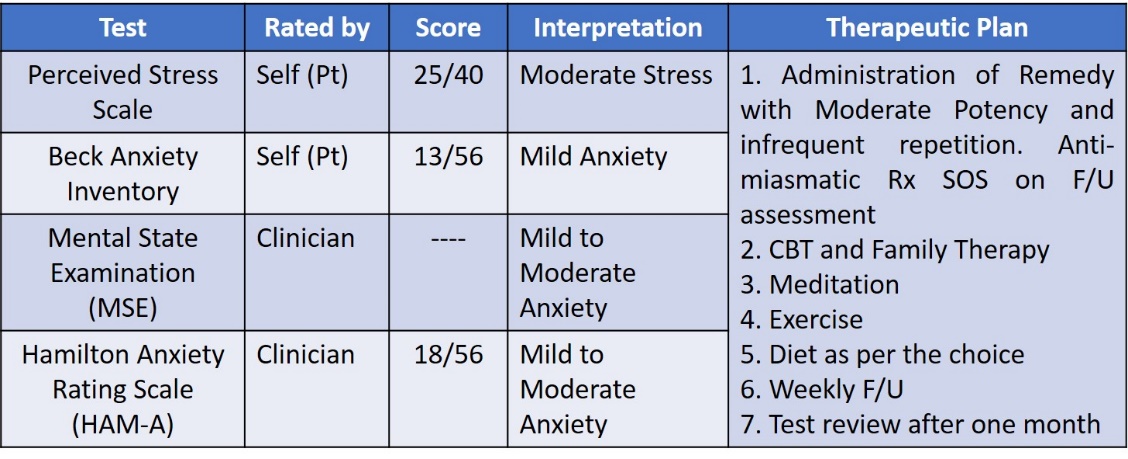
| Table 2: Before homoeopathic intervention |
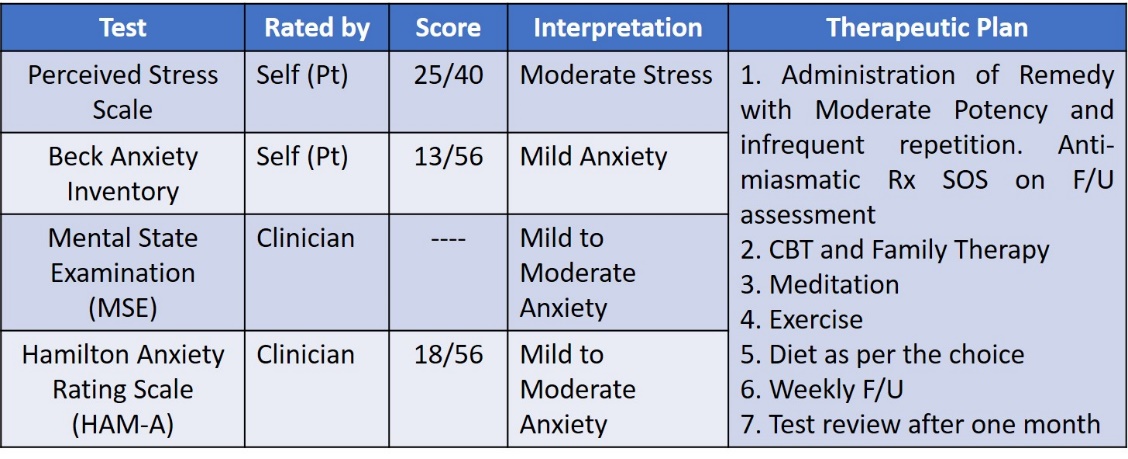
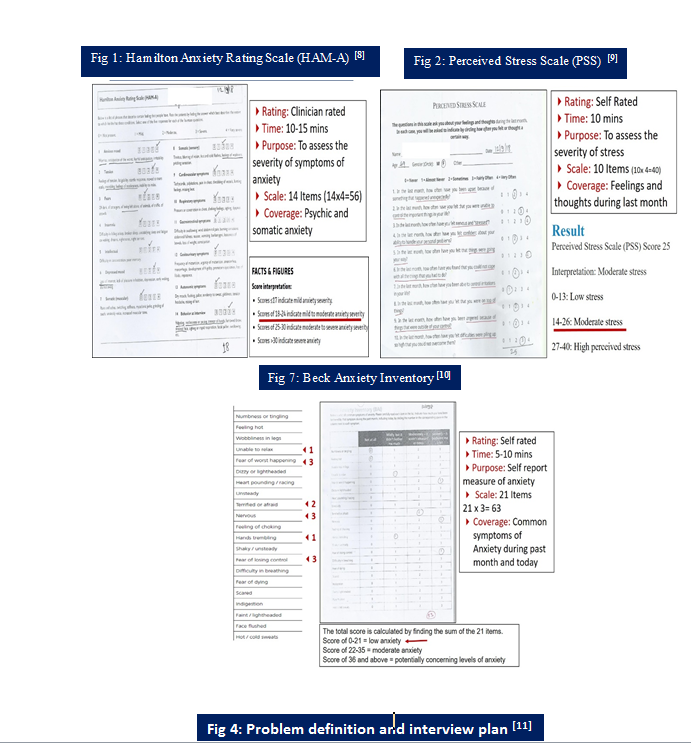
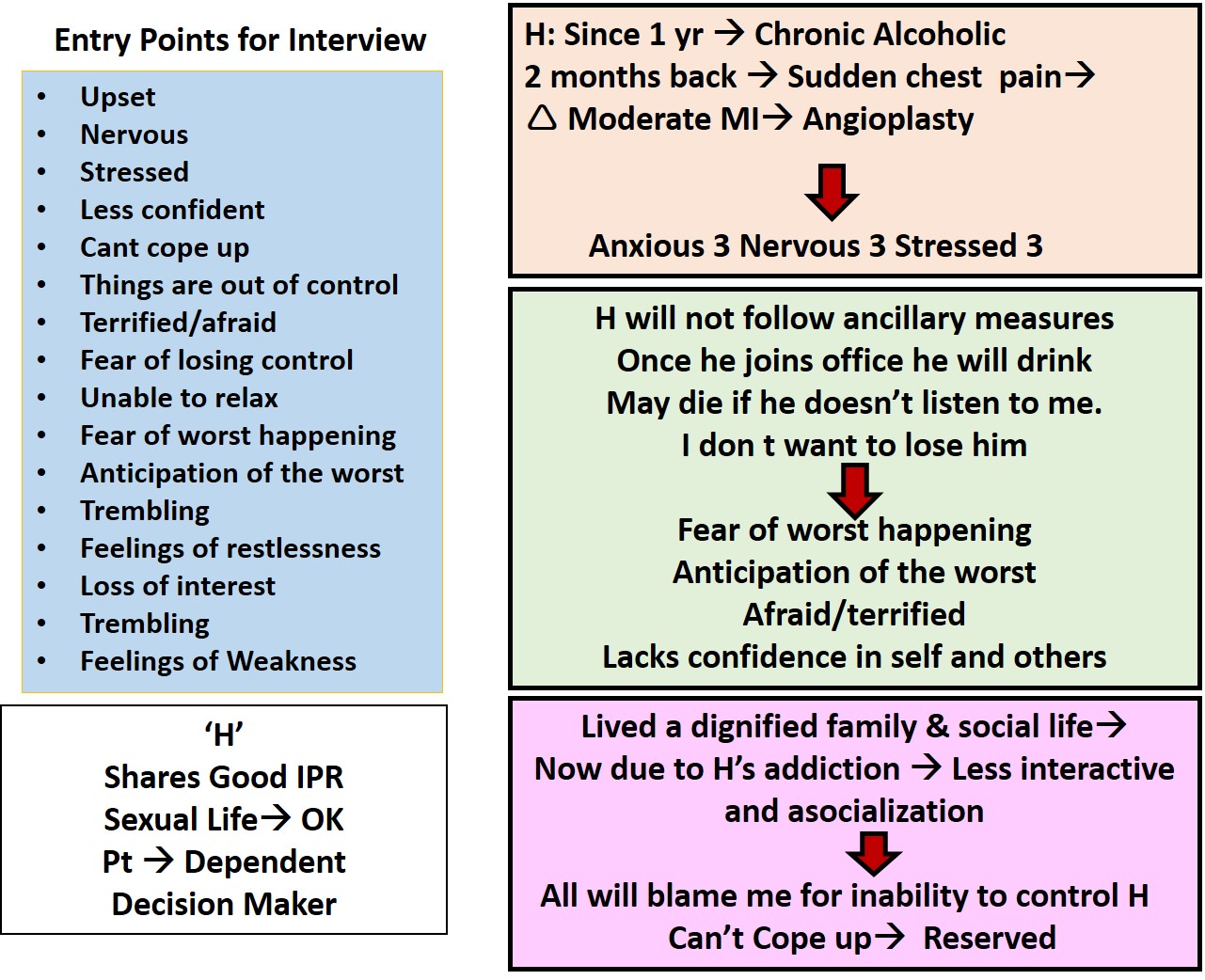
Discussion: – In this case, there were few symptoms and understanding the core feeling of the patient as a person in view of the underlying emotion was of prime importance. There was paucity of data in this case. To evaluate the cause and effect relationship and severity of the disease, psychiatric assessment scales were used viz. Hamilton Anxiety Rating scale (HAM-A) clinician rated and Perceived Stress scale (PSS) and Beck Anxiety Inventory (BAI) self-rated scales were used. HAM-A (Fig.1) the clinician rated scale having coverage of somatic and psychic anxiety for the assessment of severity of anxiety is built upon scale of 14 having different phrases that describes certain feelings people have and rating is done by finding the answer that describes the extent to which he/she has these conditions. For the selection there are five responses (0- not present, 1- mild, 2- moderate, 3-severe and 4- very severe). After assessment of the patient score was 18; interpreted as mild to moderate anxiety severity. PSS (Fig. 2) self-rated scale having coverage of feelings and thoughts during the last month for the assessment of the severity of stress. The scale is built upon 10 items indicating how often he/she has felt or thought in a certain way. For the selection there are 5 responses (0-Never, 1-almost never, 2- sometimes, 3- fairly often and 4-very often). The score was 25; interpreted as moderate anxiety. BAI (Fig. 3) self-rated scale having a list of common symptoms of anxiety. It indicates how much he/she have been bothered by that symptom during the past month, including today, by circling the number in the corresponding space in the column next to each symptom. For the selection there are 4 responses (0-not at all, 1-mildly, but didn’t bother me much, 2- moderately- it wasn’t pleasant at times, 4- severely- it bothered me a lot). The score was 13; interpreted as low (mild) anxiety. Mental state examination (MSE) a clinician based assessment was interpreted as mild to moderate anxiety. MSE and psychiatric assessment scales helped to identify the emotional turmoil of the patient with identification of entry points to the case for further enquiry of the patient. (Fig.4). Based upon MSE, HAM-A, PSS and BAI scales the disease diagnosis was done as generalised anxiety disorder. (Fig. 5).
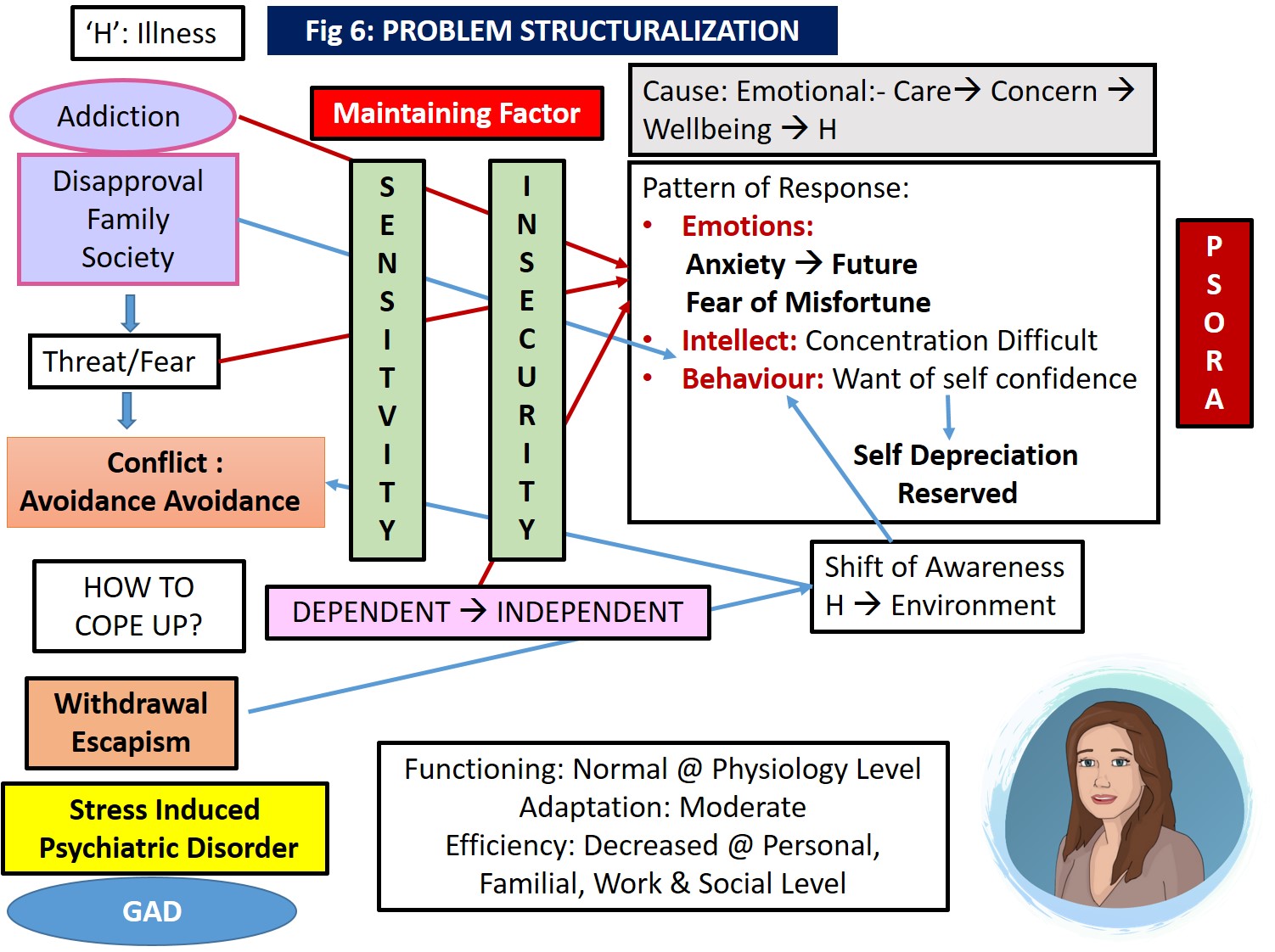
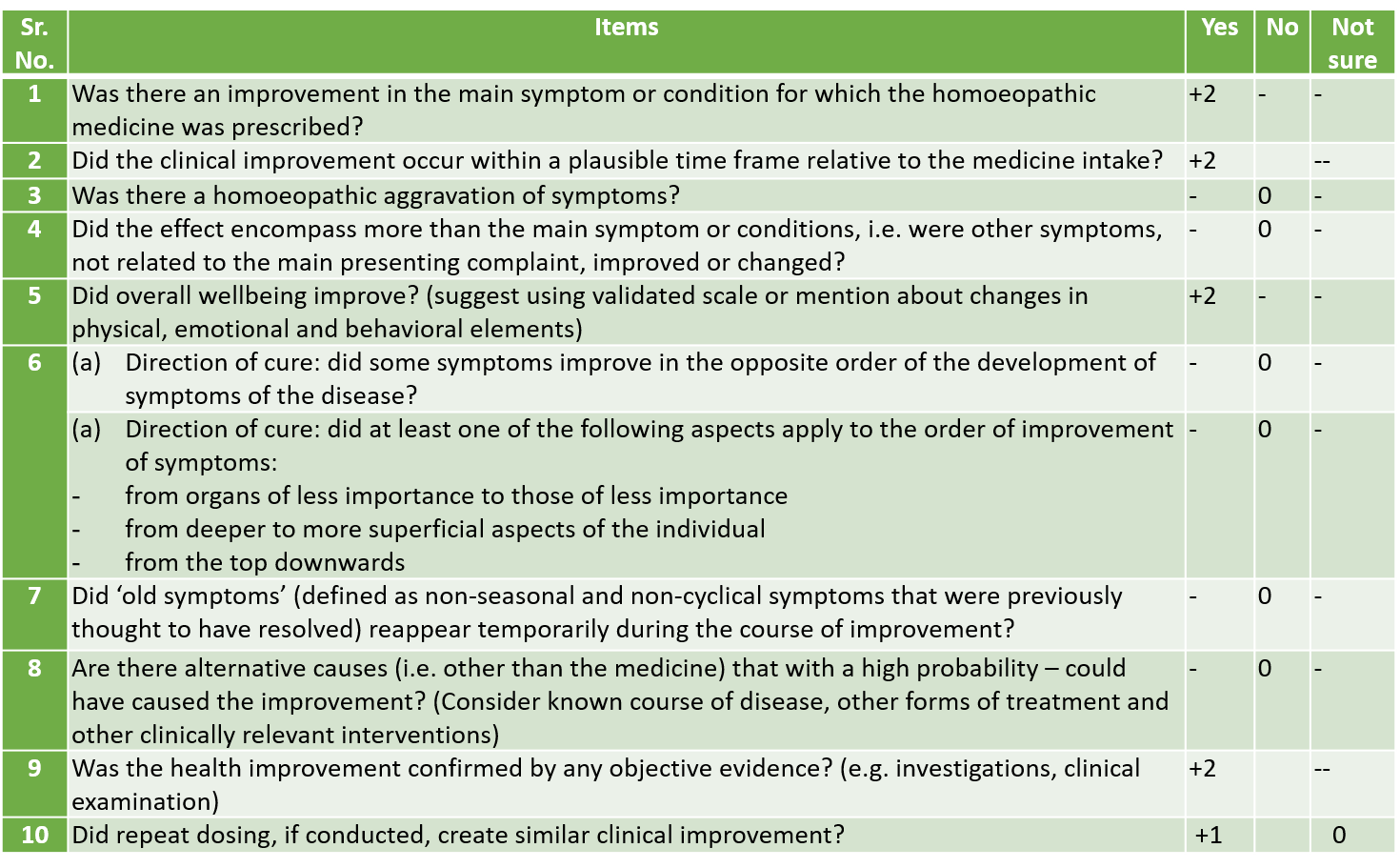
Problem structuralisation (Fig. 6) was done in view to evolve the portrait of patient as a person for perceiving the evolution of disease. Use of MSE, HAM-A, PSS, BAI scales and the interview helped to identify causation, maintaining factors and the resultant expression in the form of emotional, behavioral and intellectual. The underlying cause for the suffering was identified as emotions generated out of care and concern for the wellbeing of her husband. Maintaining factors were the sensitivity towards husband’s addiction that will be disapproved by the family and society leading into being held responsible for the situation. This generated threat and fear out of insecurity towards self-existence as everything was going normal until the husband’s angioplasty. She anticipates that husband will not follow ancillary measures and he may die. Anticipation and fear of worst happening. She had lived a dignified family and social life and now due to husband’s addiction she anticipates that all will blame for her inability to control husband’s addiction. She is finding difficulty in coping up with the state of dependency and how to turn in to the earlier state of independency? This conflict of avoidance- avoidance has affected her functioning at mind level with a pattern of moderate adaptation and decreased efficiency at family, work and social level. She has become less interactive and reserved. At surface level, there is functional integrity of physiological functions. The pattern of response seen is anxiety for future, fear of misfortune, difficulty in concentrating and self-depreciation, reserved behavior due to the want of self-confidence. All this led into shifting of awareness from husband towards environment leading to withdrawal by using defense mechanism of escapism resulting into stress induced psychiatric disorder i.e. GAD. The above understanding of psychodynamics depicts psora as a dominant miasm. After repertorisation (Fig. 7) Anacardium orientale was selected (Fig. 8) on the basis of materia medica understanding in relation with the core understanding of causation of disease as emotions care, fear of misfortune, internal conflict and lack of self-confidence/inferior feeling. Planning and programming of Homoeopathic treatment was done (Table 1). Before homoeopathic intervention, a therapeutic plan was made (Table 2). Follow up criteria was defined (Table 4). Follow up was recorded in view of subjective distress, mental generals, and any new symptoms. Follow up interpretation was done in view of susceptibility, reaction, sensitivity, clinical thinking and the direction of disease progress. On this basis action plan was formulated with expectations from the treatment. Homoeopathic treatment was started with Anacardium orientale 200 single dose at bedtime and after 2 weeks the intensity of anxiety was reduced with improvement in the interaction with husband, concentration was improved, restlessness and irritability was absent. Fear of misfortune was there. There was registration of remedy at emotional level but there is still impairment at other family, work and social areas therefore Anacardium orientale 200 3 packets at bedtime was administered for two weeks. In third follow up patient was asymptomatic and evaluation was done by using psychiatric assessment scales (Table 4) which showed that there is no stress/anxiety. Assessment by MONARCH inventory (improved version of the modified Naranjo Criteria) for homoeopathy (Table 5) had a score of 09 clearly shows casual attribution between homoeopathic intervention and the clinical outcome.
| Table 3: Follow up |
| Date | Follow Up Analysis | Interpretation | Action | Expectations | Reasons for Deviations | |||
| Subjective Distress + Generals: Mental | New Symptoms | Susceptibility Reaction Sensitivity | Clinical Thinking/ Disease Direction | |||||
| Baseline 12/08/18 | Case Definition & Processing Done Advice: Next time to come with H | Anacardium 200 1Pkt HS | Pt should be better within 1-2 months | —— | ||||
| First F/U 20/08/18 | Anxiety>+ Concentration improved Restlessness Ab Irritability Ab Rest SQ (CD & Family Counselling done: H à Lyco 200 1PHS) | No | Moderate | Same | Anacardium 200 1 Pkt HS x 2 Weeks | —— | ||
| II F/U 08/09/18 | H following Ancillary measures but still pt is having fear of misfortune (untimely death of H) Intensity of anxiety >++ Occ. feels that things are out of control Asocialization SQ Interaction with H improved but SQ with Society | No | Moderate | Same | Anacardium 200 3Pkt HS x 2 weeks Plan: Next F/U If Case –SQ Anti-miasmatic Rx | Restoration in the important areas of functioning (Family, Work, Social) | Registration of remedy at emotional level but with impairment at other areas SQ | |
| III F/U 28/10/18 | >+++ ‘H’ took VRS | >+++ | No | Moderate | Same | Assessment by Psychiatric Scales SL x 1 Month | Full time amelioration in the absence of exciting factors | ——- |
| IV F/U 4/01/19 | No C/o Her son was having Acute C/O ‘H’ is on Rx. Quited Alcohol | No Rx | ||||||
| Table 4: After Homoeopathic Intervention |
| Table 5: Assessment by MONARCH inventory (improved version of the Modified Naranjo Criteria) for Homoeopathy [17] |
Conclusion:
- Accurate case taking, recording, and analysis is necessary besides other types of evidence to convince about the specific sphere of action of homoeopathic medicines.
- Therefore, the documented case records must fulfill criteria of indications of the casual relationship between medicine and improvement, its significance in daily practice, and its agreement with similar cases.
- The impact of standardised case reports is useful if the document guides towards a clear algorithm i.e. what information led to build the totality of symptoms, repertorial approach and final remedial selection, if the results are reproducible, and last it gives valid information for extension of knowledge levels.
- In this context we need to strengthen the reporting of case records with the help of tools like HAM-A, BAL, MSE, and PSS aids into evaluating the severity of patient’s suffering.
- MONARCH helps to attribute the likelihood of causal relationship that are in tune with the homoeopathic principles.
| Management: 1. Remedial Anacardium Orientale 200 1PHS 2. Non Remedial Cognitive Behavioral Therapy:Insight about negative perception that change wont take.Desensitization: Compulsive thinking about misfortune.Modification in behavior & willingness to face challenges of life. |
References:
- Kendall, P. C., Pimentel, S., Rynn, M. A., Angelosante, A., & Webb, A. (2004). Generalized anxiety disorder. In T. H. Ollendick & J. S. March (Eds.), Phobic and anxiety disorders in children and adolescents: A clinician’s guide to effective psychosocial and pharmacological interventions (pp. 334–380). Oxford University Press. https://doi.org/10.1093/med:psych/9780195135947.003.0012
- Rowa, K., & Antony, M. M. (2008). Generalized anxiety disorder. In W. E. Craighead, D. J. Miklowitz, & L. W. Craighead (Eds.), Psychopathology: History, diagnosis, and empirical foundations (pp. 78–114). John Wiley & Sons Inc.
- Kessler RC, Demler O, and Frank RG. et al. Prevalence and treatment of mental disorders, 1990 to 2003. N Engl J Med. 2005 352:2515–2523. [PMC free article] [PubMed] [Google Scholar]
- Kessler RC, Chiu WT, and Demler O. et al. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005 62:617–627. [PMC free article] [PubMed] [Google Scholar]
- Krawiecka M, Goldberg D, Vaughan M. A standardized psychiatric assessment scale for rating chronic psychotic patients. Acta psychiatrica scandinavica. 1977 Apr;55(4):299-308.
- Hahnemann S. Organon of Medicine. Noida: B Jain Publishers; 2004.
- DSM–5: Frequently asked questions. DSM-5 FAQ. (n.d.). Retrieved October 2, 2021, from https://www.psychiatry.org/psychiatrists/practice/dsm/feedback-and-questions/frequently-asked-questions.
- Hamilton M. Hamilton anxiety scale. Group. 1959;1(4):10-37.
- Cohen S, Kamarck T, Mermelstein R. Perceived stress scale. Measuring stress: A guide for health and social scientists. 1994;10(2):1-2.
- Gphealth.org. [cited 2021 Oct 4]. Available from: https://www.gphealth.org/media/1087/anxiety.pdf
- Kapse AR. ICR Operational Manual. Mumbai: Dr M L Dhawale Memorial Trust; 2015.
- American Psychiatric Association A. Diagnostic and statistical manual of mental disorders 5th edition. Washington, DC: American Psychiatric Association; 2013.
- Complete repertory, ZOMEO 3.0 version.
- Synthesis repertorytreasure, 9.0 version, RADAR 2.1.11
- Boger CM. A Synoptic Key to the Materia Medica: (a Treatise for Homoeopathic Students). B. Jain publishers; 2002.
- Hahnemann S. The chronic diseases. Boericke & Tafel; 1904.
- Lamba CD, Gupta VK, van Haselen R, Rutten L, Mahajan N, Molla AM, Singhal R. Evaluation of the modified Naranjo criteria for assessing causal attribution of clinical outcome to homeopathic intervention as presented in case reports. Homeopathy. 2020 Nov;109(04):191-7.
About the author-
Dr YOGESH D. NITURKAR MD (Hom) ICR, Mumbai
Author has been practicing Classical Homeopathy at Mathura Homeopathic Clinic Latur, and he is author of many homeopathic articles. He is presently working as an Assistant Professor in Department of Organon of Medicine & Philosophy at V. K. Homoeopathic Medical College and Hospital, Latur.