Abstract: Benign paroxysmal positional vertigo (BPPV) is an inner ear disorder in which any positional change of head leads to sudden vertigo, i.e. a feeling that the room is spinning. The impact can range from a mild annoyance to a highly debilitating condition, and can affect risk of function, safety, and fall. The sense of losing equilibrium can result into medical shopping by the “SICK” for the sake of “CURE.” The below mentioned case demonstrates the scope of homoeopathy against the allopathic mode of treatment by a physician and an ENT specialist showcasing the journey of patient from IPD to OPD without any sigh of relief.
Keywords: audiology, BPPV, Phosphorus, simillimum, susceptibility, posology.
Abbreviations: BPPV – Benign paroxysmal positional vertigo, IPD – inpatient department, OPD – outpatient department, ENT – ear, nose, throat, Fr – frequency, M.A. – Master of Arts, Tab. – tablet, sos – si opus sit, ICD – International Classification of Diseases, O/E – on examination.
Introduction:
Benign paroxysmal positional vertigo (BPPV) is the most common peripheral vestibular end-organ disease. It is characterised by a sudden, transient gyratory sensation which is accompanied by characteristic nystagmus. Symptoms are provoked by positional changes of the head with respect to gravity and can range in severity from mild dizziness to debilitating episodes that may induce nausea or vomiting, and significantly hinder daily functioning. [1] BPPV has psychosocial consequences in terms of medical consultations, interruption in daily activities, sick leaves (work absenteeism). The association between BPPV and depression, anxiety and diminished quality of life has been shown in several studies. [2]
BPPV and its underlying psychosocial consequences can be managed with homoeopathic treatment. It needs perceiving of the individual disease, selection of the simillimum on the basis of totality of symptoms and administering the medicine in the required dosage. The selection of the dose is as much an integral part of the process of making a homoeopathic prescription as the selection of the remedy, and often quite as important. According to Jahr, in a given case, where the symptoms are not clearly developed and there is an absence or scarcity of characteristic features; or where two or three remedies seem about equally indicated, susceptibility and reaction may be regarded as low. We give, therefore, the remedy which seems most similar, in a low (third to twelfth) potency. But, when most symptoms of a case clearly indicate one remedy, whose characteristic symptoms correspond closely to the characteristic symptoms of the case, we give the high potencies – thirtieth, two hundredth, thousandth, or higher, according to the prescriber’s degree of confidence and the contents of his medicine case. [3]
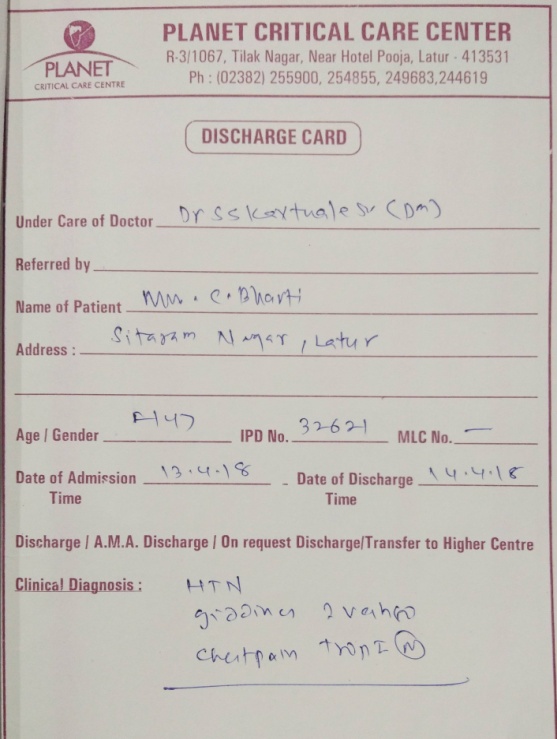
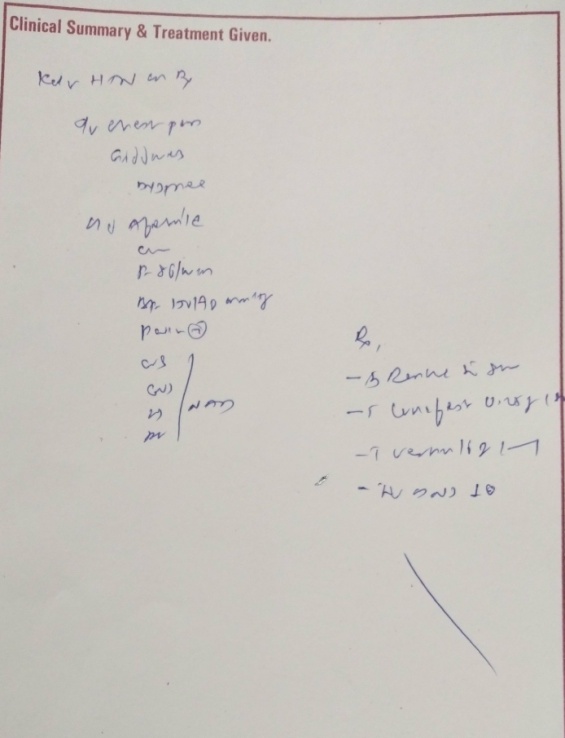
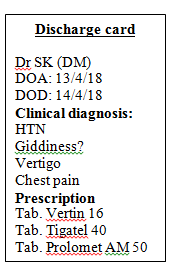
Background: Patient went to allopathic physician for her complaints of vertigo. The physician admitted her for 24 hours observation in order to evaluate her hypertension and vertigo. She was discharged from the hospital with routine prescription which didn’t give any relief to the patient so she consulted to an ENT specialist. Audiology was done and the case was diagnosed to have BPPV. Now the case was diagnosed but the treatment was not helping. Patient did her medical shopping from 13/4/18 to 24/4/18 without any relief and finally she stopped allopathic medicines and opted for homoeopathic treatment. After going through the brief history of her complaints and the allopathic prescriptions, physician decided to take her chronic case along with the acute case, in order to understand remedy relationship and the need of a deep acting constitutional remedy.
Case study
Preliminaries: Date: ► 24/04/18►Name: CBR ►Age:47 years ►Gender: Female ►Religion: Hindu ►Education: MA ►Occupation: House wife ►Marital Status: Married ►Husband: Private tuition Teacher ►Diet: Veg ►Children: No issue ►Address: Sitaram Nagar, Latur ►Native: Hyderabad
Chief Complaint:
| Location | Sensation | Modalities | Accompaniments |
| EaràInneràsemicircular canals of the vestibular labyrinth Onset: Since 10 days Fr: Daily Intensity: Moderate Duration: Till the effect of allopathic medicine or till she takes rest Pace: Status quo | Vertigo as if everything around her is moving2 No tinnitus No deafness No vomiting/nausea | < Morning2 < Head movement2 < Standing or sitting posture2 even without any head movement > By rest3 > Head at standstill3 > Closing/opening eyes3 | Fear of being alone3 |
►Family history (F/H): Father, mother and brother – hypertension
►Past history (P/H): hysterectomy, hypertension
Physical generals: ►Appearance: stocky ►Perspiration: normal ►Appetite: normal ►Cravings: milk products2 ►Aversion: onion2 ►Thirst: normal ►Sleep: normal ►Dreams: anxious feels better after waking3 ► Stool: normal ►Urine: normal ►Sexual function: normal ►Thermal state: chilly
Life space: Patient is from Hyderabad and belongs to a well to do family. Her childhood and educational period was uneventful. Parents were well educated and provided everything as per the need of the hour. Since childhood she used to be anxious on small issues. She played only with her siblings and had preferred to be within her comfort zone. After completing her M.A., she got married. Her husband is private tuition teacher. Ten years back, they came to Latur with reference of a friend and started private IIT foundation tuition classes. Within a short span, her husband became famous and a known figure in Latur. Patient occasionally helps her husband in administration work. She prefers to be at home with minimum socialisation. She is health conscious and gets worried with minute ailments. She is calm, emotional, and shy by nature. She likes reading and watching television serials. She took lots of treatment for her infertility but later on stopped it as she didn’t conceive. Patient and her husband accepted the fact and moved ahead in their life. Occasionally, patient becomes emotional on not having a child but later on neglects about it.
Examination findings: General appearance: Short stature, stocky built, well dressed in a typical south Indian attire. Afebrile, pulse: 84/min, blood pressure: 130/80 mm Hg, weight: 58 kg.
No nystagmus.
Romberg’s test: positive
Systemic examination (S/E): Central nervous system: Nothing abnormal detected. Cardiovascular system: normal. Respiratory system: clear. Per abdomen: soft.

Case processing
- Disease diagnosis: benign paroxysmal positional vertigo (BPPV) ICD- 10 CM: H81.10[4]
- Hahnemannian classification of disease: acute [5]
- Miasmatic considerations: Acute: psora: functional pathology and at mind level fear of being alone as a mental concomitant, anxiety; Chronic: sycosis: anxiety, indolence, reserved nature, infertility, and hypertension.
- Susceptibility: moderate
- Sensitivity: high
- Correspondence: total: simillimum
- Potency: 200 (functional pathology and moderate level of susceptibility)
- Repetition: infrequently [6]
- Repertorial totality of symptoms
Acute:
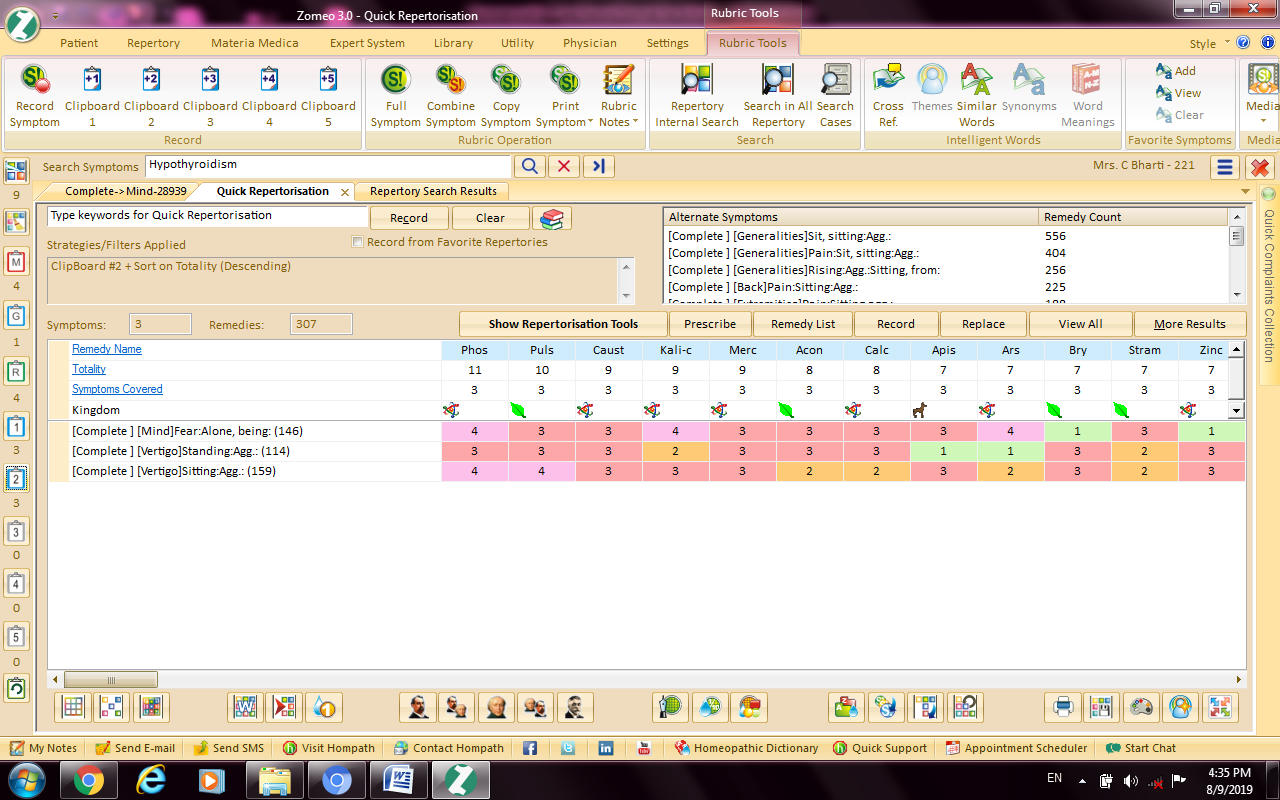
Phosphorus: 11/3(Chilly), Pulsatilla nigricans 10/3 (Hot), Causticum: 9/3 (Chilly)
Chronic:
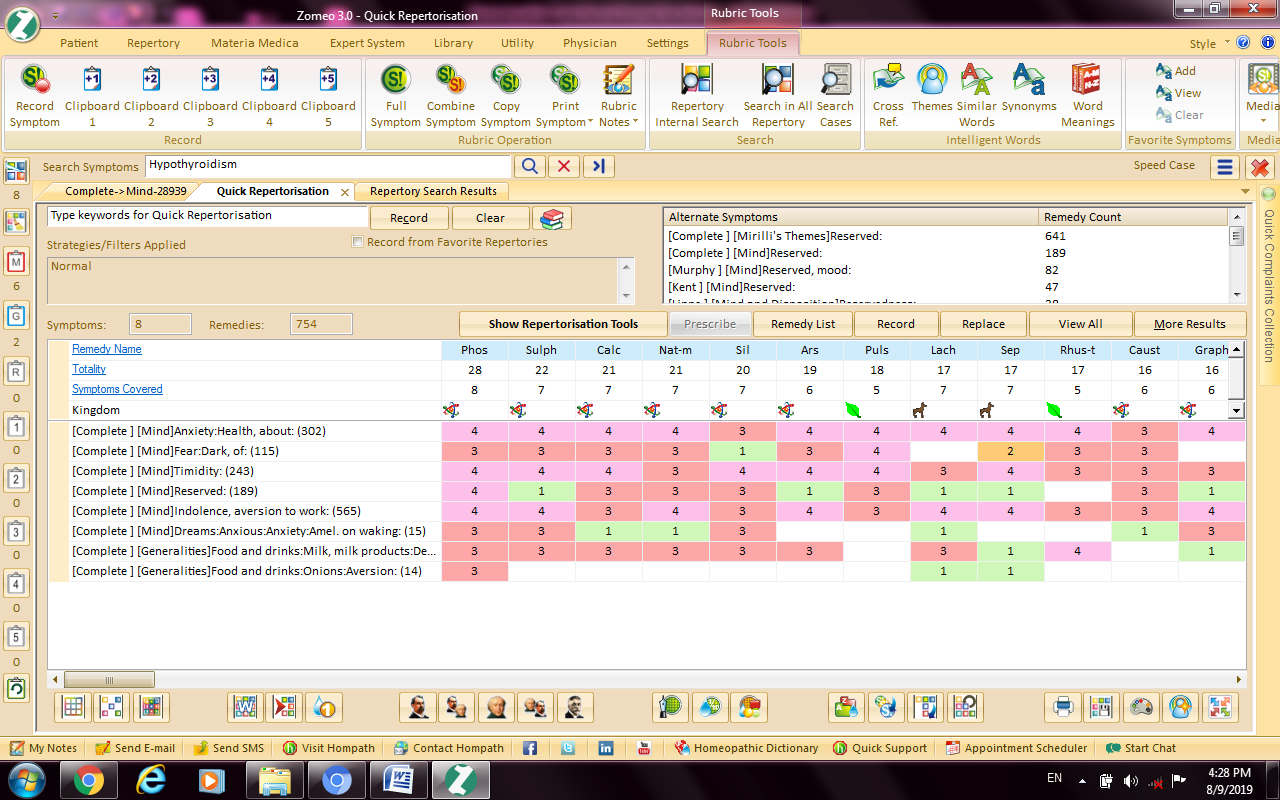
Phosphorus: 28/8 (Chilly), Sulphur: 22/7 (Hot), Calcarea carbonicum: 21/7 (Chilly)
Phosphorus was a well indicated remedy in this case as it was predominantly covering sector and dispositional totality, i.e. acute and chronic. The final selection of remedy is Phosphorus. The confronting question was whether to give Phosphorus in a single dose or repeated doses. The below mentioned conceptual understanding helped to select the appropriate dosage:
- Acute was having a striking and characteristic mental concomitant.
- Pathology of acute disease was functional with reversible nature having psora as dominant miasm, whereas the nature of chronic disease was of sycosis (fundamental miasm)
- Overall reactivity at mind and body was seen.
- Susceptibility was of moderate degree.
- Sector totality was same in spite of allopathic medication, i.e. there was no suppression.
- General vitality was good.
- Correspondence (simillimum) at acute and chronic level was total.
- Phosphorus is having a tendency to increase vitality or any genuine stimulation of function. [7]
Therefore, based upon this understanding first prescription was given Phosphorus 200/single dose at bedtime and awaited reaction. Patient was called after 8 days.
Follow up: 2/5/18: No vertigo. No fear of being alone. No complaints. She was going out of station to attend marriage at her native place. As she was going alone and will stay there for 1 month, she was having anxiety about recurrence of complaints. Patient complimented by saying, “Doctor you have restored my balance.” O/E – Blood pressure: 110/80 mm Hg. Romberg’s test – negative.
Action: Phosphorus 200/single dose once in 15 days.
6/6/18: No complaints. O/E – nothing abnormal detected. Action: Placebo.
Conclusion: Homoeopathy is having scope in the management of functional diseases with reference to BPPV where allopathic treatment seems ineffective. The selection of homoeopathic dose as per the sector and dispositional totality enhances better patient outcome.
Acknowledgement: Author would like to acknowledge Dr Sunil Bhalinge for his expert opinion on correlation between simillimum and the repetition strategy in acute case.
References:
- You P, Instrum R, Parnes L. Benign paroxysmal positional vertigo. Laryngoscope investigative otolaryngology. 2019 Feb;4(1):116-23.
- Von Brevern M, Radtke A, Lezius F, Feldmann M, Ziese T, Lempert T, Neuhauser H. Epidemiology of benign paroxysmal positional vertigo: a population based study. Journal of Neurology, Neurosurgery and Psychiatry. 2007 Jul 1;78(7):710-5.
- http://homeoint.org/books4/close/chapter13.htm
- https://www.icd10data.com/ICD10CM/Codes/H60-H95/H80-H83/H81-/H81.13
- Hahnemann S. Organon of Medicine. Noida: B Jain Publishers; 2004.
- Dhawale ML. ICR Symposium Volume on Hahnemannian Totality. 3rd ed. Mumbai: Dr M L Dhawale Memorial Trust; 2003.
- Farrington E. A. Clinical Materia Medica. 4th Revised and enlarge edition. New Delhi: B Jain Publishers (P) Ltd. 2014.
About the author-
Dr YOGESH D. NITURKAR MD (Hom) ICR, Mumbai
Author has been practicing Classical Homeopathy at Mathura Homeopathic Clinic Latur, and he is author of many homeopathic articles. He is Assistant Professor in Department of Organon of Medicine and Philosophy at V. K. Homoeopathic Medical College and Hospital, Latur.