
Generalized Anxiety Disorder is a common mental disorder marked by persistent anxiety and worries, which are excessive and difficult to control as well as multiple psychological and physical symptoms. GAD has often has a chronic course with a lifetime prevalence rate for DSM-IV criteria estimated at approximately 6%.
Persons suffering from GAD present significant impairments in work, social and family functioning, and health related quality of life. There is also increasing evidence regarding the economic burden of GAD in terms of lost work productivity and medical costs due to high utilization of medical services. GAD is highly associated with co-morbid psychiatric disorders, with major depressive disorder being the most frequent and co-morbid physical illness.
Difference between normal worry and GAD
| Normal worry | Generalized Anxiety Disorder |
| – Your worry doesn’t get in the way of your daily activities and responsibilities. – You’re able to control your worry. – Your worries, while unpleasant, don’t cause significant distress. – Your worries are limited to a specific, small number of realistic concerns. Your bouts of worrying last for only a short period of time. |
– Your worry significantly disrupts your job, activities or social life. – Your worry is uncontrollable. – Your worries are extremely upsetting and stressful. – You worry about all sorts of things, and tend to expect the worst. – You’ve been worrying almost every day for at least six months. |
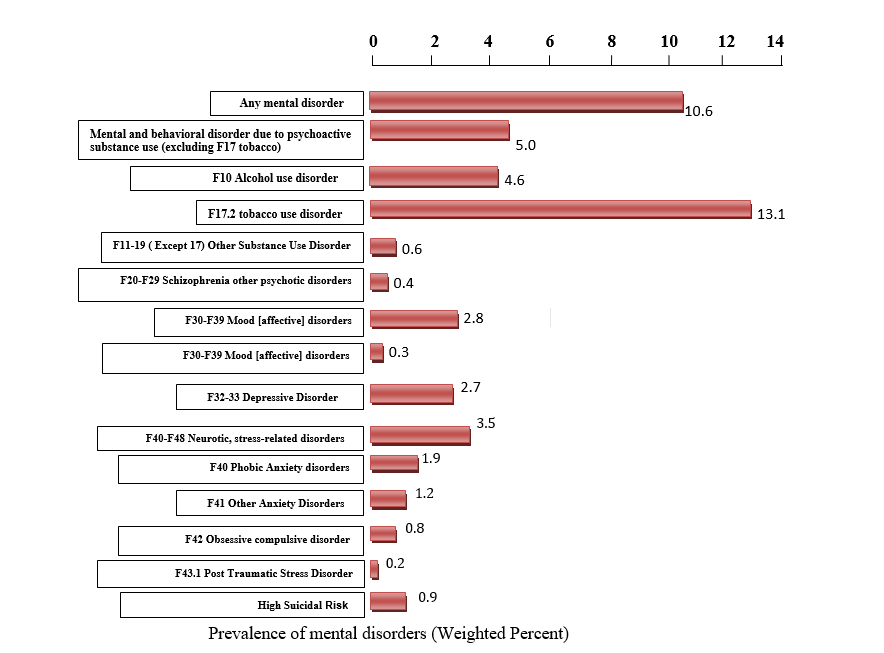
Epidemiology
In India an estimated prevalence rate is 20.7% (18.7-22.7) for all neurotic disorders,
which was reported to be highest among all psychiatric disorders. The weighted
prevalence rates of different anxiety disorders were –
- 4.2% (Phobia)
- 5.8% (GAD)
- 3.1% (Obsession) and
- 4.5% (Hysteria).
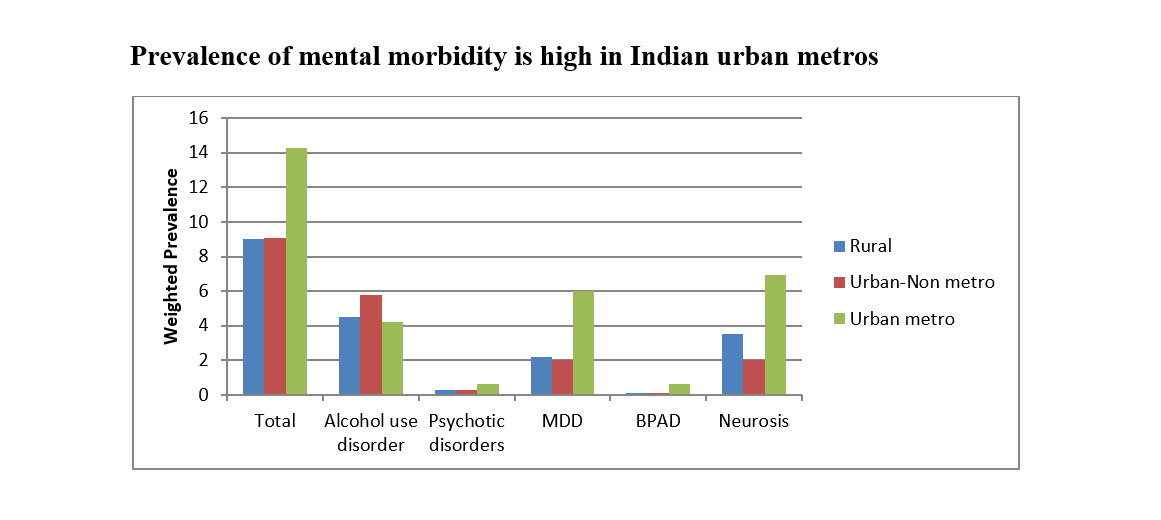
Prevalence of mental morbidity is high in Indian urban metros
PATHOPHYSIOLOGY
Anatomical and neuro-imaging findings in patients who have Generalized Anxiety Disorder
Structural imaging studies have shown high ratios of gray matter to white matter in the upper temporal lobe of pediatric patients who have generalized anxiety disorder (GAD). Pediatric patients who have GAD also exhibit increased amygdala volume, which may correspond to the stress-induced amygdalar hypertrophy observed in laboratory animal studies.
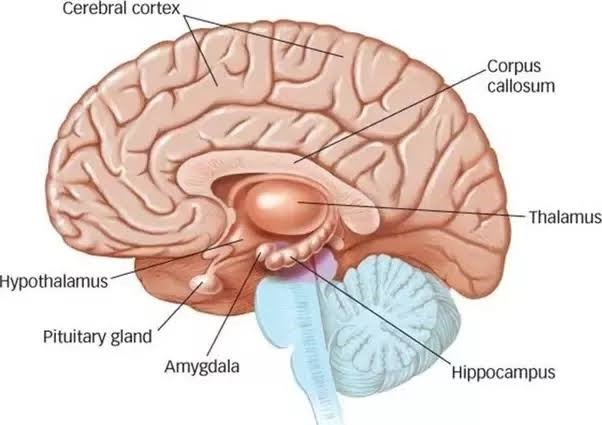
Figure 8: Structures of brain
In functional imaging studies of adolescent patients who have GAD, resting vlPFC activity is elevated relative to healthy control subjects. Because the vlPFC activity correlates negatively with symptom severity, the elevation in vlPFC metabolism is interpreted as a compensatory response rather than an underlying cause of GAD. Because of observed hyper-metabolism in the PFC of patients who have GAD, neuronal viability has been assessed in this region as measured by the ratio of N-ace-tylasparate to creatine using proton MRS. For patients who had GAD, neuronal viability was increased in the right dorsolateral PFC in those without early-life stress but was decreased in those who self-reported early-life trauma.
Functional brain imaging results obtained under resting conditions in patients who have GAD have tended to be inconsistent; provocative anxiety-inducing tasks have produced more robust and interpretable fMRI results. The pattern of brain activity in anxious patients who have GAD correlates well with results from laboratory animal studies in which limbic circuits, particularly the amygdala, play an important role in the fear response. In fact, many imaging studies of patients who have GAD show elevated amygdala and insula activation during negative emotional processing. In response to viewing angry faces, adolescent patients who had GAD exhibited an elevated right amygdala response; this activation correlated positively with symptom severity. The over-activity in the right amygdala also was correlated negatively with activity in the right vlPFC, suggesting top-down dis-inhibition as a potential mechanism for elevated amygdala activity. Interestingly, strong pretreatment activation of the left amygdala in pediatric patients who had GAD predicted a positive therapeutic response to fluoxetine or CBT. These results have been interpreted to suggest that a greater amygdaloid response to negative emotions represents a healthier signal-to-noise ratio. When adult patients who have GAD view fearful faces, lower pretreatment amygdala activity and higher ACC activity predict a positive treatment response to venlafaxine. Additional studies will be crucial in determining whether amygdala activation has clinical utility in predicting treatment outcome.
Interconnectivity with brain regions responsible for interpreting social behavior may be one mechanism by which the amygdala plays a substantial role in anxiety disorders. The brain regions responsible for interpreting social behavior include the superior temporal gyrus, thalamus, and PFC. Amygdala hyperactivity may mediate the inaccurate interpretations of social behavior in patients who have GAD.
Neurotransmitter and neuroendocrine signaling in Generalized Anxiety Disorder
The observed limbic overactivity in patients who have GAD could result from decreased inhibitory neurotransmission, increased excitatory neurotransmission, or a combination of these two processes. Dysregulation of GABA inhibitory neurotransmission has been documented in several anxiety disorders. GABAA receptor downregulation is observed in patients who have GAD and has been hypothesized to play a role in the etiology of this illness. In support of this hypothesis is the finding that symptoms of GAD, including excessive worry, hyper-vigilance, and psychomotor agitation, are treated effectively with GABAA facilitators such as benzodiazepines and barbiturates. Furthermore, treatment with riluzole, an anti-glutamatergic agent, seems to improve GAD symptoms.
Although all the SSRIs have shown efficacy in GAD, the drug most frequently studied in anxiety is paroxetine, which decreases symptoms of harm avoidance. It is important to note that GAD often is comorbid with other disorders, including MDD, PD, and SAD, each of which also has shown responsiveness to SSRI treatment.
More concrete evidence supporting a role for 5-HT circuitry in GAD includes challenge with the 5-HT2c/5-HT3 agonist mCPP, which elicits anxiety and anger in patients who have GAD.
Further evidence for a serotonergic component of GAD is provided by functional brain imaging studies that have found that midbrain SERT density correlates negatively with symptom severity. Recent studies have replicated the negative correlation between SERT density and anxiety symptoms in GAD, but there is no difference in SERT density in subjects who have GAD as compared with controls.
Patients who have GAD are hypersensitive to exogenously administered CCK agonists, leading to the study of CCK receptor–selective antagonists as a putative novel class of anxiolytics. One such drug was developed but was not demonstrated to possess anxiolytic efficacy. Additional research and development of unique CCK antagonists will be an important step in clarifying the role of CCK in anxiety and its potential as a therapeutic target.
To the authors’ knowledge, no studies have specifically examined the role of NPY in GAD. NPY does possess anxiolytic effects in laboratory animals. These anxiolytic effects may be caused by NPY–CRF interactions; these two neuro-peptides are co-localized in numerous limbic regions and exert opposing effects on the amygdala, LC, and periaqueductal gray matter, the last region is responsible for the motor output for the behavioral stress response.
Corticotropin-releasing factor and the hypothalamic-pituitary-adrenal axis
Although very few studies have specifically examined HPA axis reactivity in patients who have GAD, there is no evidence of hypercortisolism, dexamethasone non-suppression, or increased CSF CRF concentrations. That CRF and the HPA axis seem to play a less prominent role in GAD than in other anxiety disorders and MDD is perhaps surprising given that CRF antagonists have been demonstrated to possess anxiolytic effects . It is possible that the lack of evidence for a pathophysiological role for CRF circuits in GAD is an artifact of the paucity of endocrine studies in these patients. It is equally likely, however, that the difference in CRF/HPA axis observations in patients who have MDD and patients who have GAD represents a critical biological distinction between these two syndromes.
Genetic Contribution to Generalized Anxiety Disorder
Overall the genetic contribution is thought to be less substantial in GAD than in other anxiety disorders. Studies have shown that first-degree relatives of GAD pro-bands have elevated rates of mood and anxiety disorders in general and perhaps have a specifically increased risk for GAD. A recent study of more than 3000 twin pairs found modest familial aggregation of GAD with equal heritability in males and females in same-sex or opposite-sex twin pairs; there was no evidence for gender-specific genetic underpinnings of GAD. Results from twin studies estimate that approximately 32% of the variance for liability to GAD is caused by additive genetics in male and female twins and that the remaining variance is explained by environment specific to the individual, rather than the shared environment of the twin pair. Only a handful of genetic-association studies specific for GAD have been reported, and all are thus far un-replicated
DSM-V Diagnostic Criteria of Generalized Anxiety Disorder
A) Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of event or activities (such as work or school performance).
B) The individual finds it difficult to control the worry.
C) The anxiety or worry are associated with three(or more) of the following six symptoms(with at least some symptoms having been present for more days than not for the past 6 months):
Note: Only one item is required in children
- Restlessness or feeling keyed up or on edge.
- Being easily fatigued.
- Difficulty concentrating or mind going blank.
- Irritability
- Muscle tension.
- Sleep disturbance (difficulty falling or staying asleep, or restless, unsatisfying sleep).
D) The anxiety, worry or physical symptoms cause clinically significant distress or impairment in social, occupational or other areas of functioning.
E) The disturbance is not attributable to the physiological effects of a substance (e.g., a drug abuse, a medication) or another medical condition (e.g. hyperthyroidism).
F) The disturbance is not better explained by another medical disorder(e.g. anxiety or worry about having panic attacks in panic disorder, negative evaluation in social anxiety disorder[social phobia], contamination or obsessions in obsessive-compulsive disorder, separation from attachment figures in separation anxiety disorder, reminders of traumatic events in posttraumatic stress disorder, gaining weight in anorexia nervosa, physical complaints in somatic symptom disorder, perceived appearance flaws in body dysmorphic disorder, having a serious illness in illness anxiety disorder, or the content of delusional beliefs in schizophrenia or delusional disorder).
Co-morbidities of GAD
The most common co-morbidities of GAD are major depressive disorder (MDD), bipolar disorder (BD), and substance use disorder (SUD), due to the similar symptoms of these disorders.
GAD and Major Depressive Disorder
GAD presents with uncontrolled and persistent worry about a range of things like job, family, and financial status. It is a kind of floating condition, where the person drift from one worry to the next without end in such as way that it has an impact on their normal activities. MDD, often simply referred to as depression or clinical depression, is a serious mood disorder that also affects normal life. Patients with anxiety from a very young age, display low self-esteem, pessimism, and severe stress is accompanied by perpetual feelings of sadness or loss of interest over a long duration of time.
Patients at both initial and severe stages of GAD have episodes of depression (MDD). Longitudinal studies have found variations in the appearance of MDD in patients with GAD. In these studies, (a) one-third of patients showed signs of GAD leading to MDD; (b) one-third had symptoms of MDD leading to GAD; and finally (c) one-third of them had the onset of both GAD and MDD simultaneously. More than 70% of patients with lifetime GAD are also found to have lifetime MDD. Studies of twins have revealed that the same genetic factors of risk have a hand in both GAD and MDD. However, whether the patient develops GAD or MDD first depends on how they react to the environmental stressors in their life.
GAD and Bipolar Disorder
Formerly called manic depression, bipolar disorder is characterized by extreme mood variations, from high to low; at high, the patient is over-exultant, while at low he may harbor suicidal thoughts for no particular reason. It has been found that 51% of patients with BD have another anxiety disorder, which actually worsens the illness. Due to this co-morbidity, BD patients tend to have:
- Younger age of onset
- Lower quality of life
- Lower chance of recovery
- Increased risk of substance abuse, and, most importantly
- Greater lifetime suicidal tendencies
The average period of euthymia (normal positive state of mind) in BD with comorbid GAD is found to be less than half of that in patients with BD alone. Surveys have shown suicide attempts of 62% and 53% in BD and current and lifetime GAD comorbidity patients, respectively, as opposed to 22% in patients with BD alone.
Impulsiveness tends to be heightened in BD and current GAD patients, even after adjustments are made for age, gender, and presence of other comorbid anxieties.
GAD and Substance Use Disorder
Research studies have shown a significant link between patients of GAD and substance use or abuse. Most people with GAD are unaware of their illness and try to ease their anxiety by self-medication using alcohol or drugs.
One-third of individuals with GAD are sufferers of SUD, though they are mostly known to use and not abuse substances. A mutual pattern exists between these two disorders, which follow three pathways:
- Anxiety leading to substance use
- Substance use/abuse leading to anxiety
- Genetic risks that are central to both GAD and SUD.
Management of Generalized Anxiety Disorder
Cognitive behavioral therapy (CBT) of generalized anxiety disorder (GAD) is based on the theory that the disorder sterns from constant perceptions of the world as a dangerous place, resulting in a process of maladaptive and habitual interactions among cognitive, behavioral, and physiological response systems. Maladaptive cognitive responses include a pre-attentive bias to’ threat cues, negatively valenced images and worrisome thinking and cognitive avoidance of some aspects of anxious experience. Maladaptive behavioral responses include subtle behavioral avoidance and slowed decision-making. The physiological responses entail excessive muscle tension and an autonomic inflexibility based on a deficiency in parasympathetic tone.
Relaxation training
Relaxation is the voluntary letting go of tension. This tension can be physical tension in the muscles or it can be mental, or psychological, tension. When we physically relax, the impulses arising in the various nerves in the muscles change the nature of the signals that are sent to the brain. This change brings about a general feeling of calm, both physically and mentally. Muscle relaxation has a widespread effect on the nervous system and therefore should be seen as a physical treatment, as well as a psychological one. This section will discuss how to recognize tension, how to achieve deep relaxation, and how to relax in everyday situations. You will need to be an active participant in relaxation, committed to daily practice for two months or longer.
Components of relaxation training
In order to be more in control of your anxiety, emotions, and general physical well-being, it is important to be able to relax.
To do this you need to:
- Recognize tension.
- Relax your body in a general, total sense.
- Let tension go in specific muscles.
HOMOEOPATHIC REMEDIES FOR ANXIETY DISORDERS
- Aconitum napellus:
AILMENTS FROM: Sudden fright , fear , shock. great fear and anxiety of mind, with great nervous excitability. Afraid to go out in the crowd, cross the street. The countenance is expressive of fear. Restless, anxious, does things in haste. Must change position often; everything startles him.
- Argentum nitricum:
This remedy can be helpful when anxiety develops before a big event: an exam, an important interview, a public appearance or social engagement. Fearful and nervous; impulse to jump out of window. Faintish and tremulous. Melancholic, apprehensive of serious disease. TIME PASSES SLOWLY. IMPULSIVE; WANTS TO DO THINGS IN A HURRY. Fear, of impending evil, of crowds, passing a certain point, of high buildings, of dark. People who need this remedy are often enthusiastic and suggestible, with a tendency toward peculiar thoughts and impulses. They often crave sweets and salt (which usually make their symptoms worse). The patient is very nervous and impulsive by nature; extremely hurried in whatever he does. He dreads situations that may cause him anxiety and tries to avoid getting into such situations.
- Arsenicum album:
Restlessness with fear of death. Mentally restless, but physically too weak to move; changes place continually. Anxious with fear of death, incurable. Attacks of anxiety at night which drives him out of bed < midnight.
- Aurum-Met:
Such a patient shows an overly conscientious, work oriented attitude and an easily agitated conscience. There is also an obsession with certain ideas that cannot be easily shaken such as the feeling of being deserted by one’s best friends or the suicidal impulse to put an end to this worthless life.
- Calcarea carbonica:
Anxious. Fears she will lose her mind. People will observe her mental confusion. Longs fresh air. Coldness of single parts. Desire to be magnetised. Feels better when constipated.
- Carcinosin:
Fastidious in his work; Desire to come for appointment on time. Fears to make mistakes. Feeling guilty while taking rest without having finished all the work.; even when sitting he has the feeling that he must do something like reading, knitting etc. Inability to refuse anything and always wants to please everybody; feeling guilty when refusing anything, but unaware of his own needs and permits others to overstep his own boundaries15.
- Gelsemium:
Feelings of weakness, trembling, and mental dullness (being “paralyzed by fear”) suggest a need for this remedy. It is often helpful when a person has stage-fright about a public performance or interview. STAGE-FRIGHT, NERVOUS DREAD OF APPEARING IN PUBLIC THE ANTICIPATION OF ANY UNUSUAL ORDEAL, PREPARING FOR CHURCH,THEATRE, OR TO MEET AN ENGAGEMENT, BRINGS ON DIARRHOEA. Every exciting news causes diarrhea; bad effects from fright and fear. Bad effects from suddenly hearing bad new; from fright; diarrhea, abortion, etc. Emotional excitement even mere ANTICIPATION of any event brings on physical disorders. Chills, perspiration, diarrhea, and headaches will often occur with nervousness. Fear of crowds, a fear of falling, and even a fear that the heart might stop are other indications for Gelsemium.
- Ignatia amara:
nail driven into the side of the head, and cramping pains in the abdomen or back, are often seen when this remedy is needed15.
- Nat-mur:
Ailments from bad effects of anger, grief, fright, vexation. Awkward; drops things from nervous weakness. Marked disposition to weep, sad weeping mood without cause. Consolation aggravates.
- Kali Brom:
restlessness, strange illusions, fear of being alone; of being poisoned; of being pursued.
- Kali Carbonicum:
Great aversion to being alone. Timid and apprehensive of future and about her disease. Fear of being alone; fears she will die. Anxiety with fear. Very easily frightened. Full of apprehension. He is afraid that he might not get well. Apprehensive and anxious about her disease Easily startled; starts when touched esp. on feet; on dropping to sleep. Anxiety, with fear when alone. Anxiety felt in stomach. Never quiet or contented. Hypersensitive to pain, noise, touch. Fear of future, of ghosts, of death. Anxious about his own diseased condition.
- Causticum:
Ailments from long lasting grief and sorrow; from sudden emotions, fear, fright, from anger or vexation; from suppressed eruptions. Melancholy, the least thing makes the person cry.
- Nux vomica:
Person with ardent character, of irritable, impatient temperament, disposed to anger, spite or deception. Anxiety with irritability &inclination to commit suicide, but is afraid to die.
- Lycopodium:
Individuals likely to respond to this remedy feel anxiety from mental stress and suffer from a lack of confidence. They can be self-conscious and feel intimidated by 43 people they perceive as powerful yet may also swagger or be domineering toward those with whom they feel more comfortable.
- Phosphorus:
Apprehensiveness when alone; anxiety about the future; irritability and anxiety. Apprehension, as if she was grieved about something, frequently recurring. Anguish, as if about to die. Restlessness during thunderstorms. Fearfulness and horror. Great anxiety and irritability on being alone. He is fearful of many things, afraid of the dark, of being left alone, of things creeping out of corners, respecting the issue of his disease, There are anxiety and apprehension, which are often associated with a sensation as of fear at the pit of the stomach. Anxiety and restlessness are worse at twilight and may be accompanied by palpitation , palpitations, thirst, and a strong desire for cold, refreshing foods are other indications for Phosphorus.
- Pulsatilla:
People who need this remedy often express anxiety as insecurity and clinginess, with a need for constant support and comforting. The person may be moody, tearful, whiny, even emotionally childish. (Pulsatilla is a very useful remedy for children.) She is most nervous, fidgety. Tremulous anxiety, as if death were near. Anxiety, even to suicide. Palpitation of the heart and great anxiety so that he must throw off the clothes. Palpitation of the heart after dinner; from speaking Anxiety in the region of the heart, even to suicide, in the evening, associated with a sensation of qualmishness in the pit of the stomach. Anxiety with trembling of the hand. Anxious solicitude about his health.
- Silicea:
People who need this remedy are capable and serious, yet are also nervous, shy, and subject to bouts of temporary loss of confidence. Anxiety can be extreme when they are faced with a public appearance, interview, examination, or any new job or task. Worry and overwork can bring on headaches, difficulty concentrating, and states of 44 exhaustion, oversensitivity, and dread. Responsible and diligent, they often overreact and devote attention to tiny details—making their worries (and their work) more difficult. Marked anticipatory anxiety is an important feature of this drug. Sensitiveness to noise, and anxiety there from. Over-anxious about himself. Frequent attacks of anxiety Fidgety. Complaints from anticipation. Starts from slight noise.
References
- Pasquale Roberge et.al. , Generalized anxiety disorder in primary care: mental health services use and treatment adequacy, Oct 2015
- TrivediJK, Gupta PK, an overview of Indian research in anxiety disorders, Indian Journal of psychiatry 2010 Jan;52 (suppl1):S210-S218.
- http://indianmhs.nimhans.ac.in/Docs/Report2.pdf
- Elizabeth I. Martin et.al. , The Neurobiology of Anxiety Disorders: Brain Imaging, Genetics, and Psychoneuroendocrinology, Sept 2009; 32(3): 549-575.
- Sadock BJ, Sadock VA, Ruiz P (2017); Kaplan and Sadock’s Synopsis of Psychiatry Behavioral Sciences/Clinical Psychiatry ; 11th edition, Wolters Kluwer(India)Pvt. Ltd., New Delhi;p.409.
- https://www.news-medical.net/health/Generalized-Anxiety-Disorder-Comorbidities.aspx
- Kent JT, Lectures on Homoeopathic Material Medica; B Jain Publishers (P) Ltd.
Author
Dr. Urvashi Vidyarthi
BHMS, MD (Department of Psychiatry)
Dr. Himani Dhaka
BHMS, MD (Department of Pharmacy)
Bakson Homoeopathic Medical College and
Hospital, Greater Noida.



